Impetigo: Pathogenesis and clinical findings
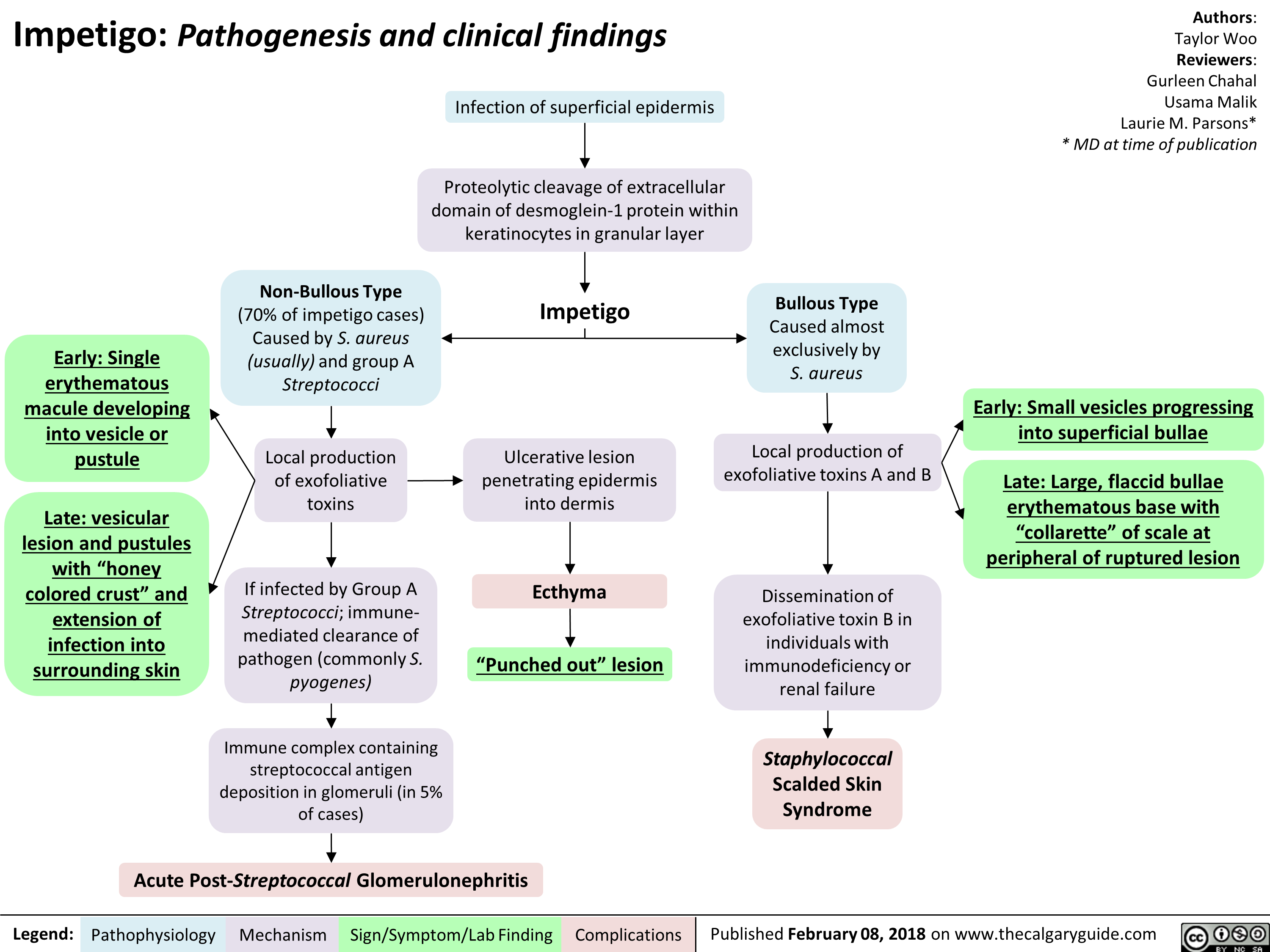
Early: Single erythematous macule developing into vesicle or pustule
Late: vesicular lesion and pustules with “honey colored crust” and extension of infection into surrounding skin
Legend:
Infection of superficial epidermis
Proteolytic cleavage of extracellular domain of desmoglein-1 protein within keratinocytes in granular layer
Non-Bullous Type (70% of impetigo cases) Caused by S. aureus (usually) and group A Streptococci
Local production of exofoliative toxins
If infected by Group A Streptococci; immune-mediated clearance of pathogen (commonly S. pyogenes)
Immune complex containing streptococcal antigen deposition in glomeruli (in 5% of cases)
1
Impetigo
Ulcerative lesion penetrating epidermis into dermis
Bullous Type Caused almost exclusively by S. aureus
Local production of exofoliative toxins A and B
Ecthyma
“Punched out” lesion
Acute Post-Streptococcal Glomerulonephritis
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Dissemination of exofoliative toxin B in individuals with immunodeficiency or renal failure
Staphylococcal Scalded Skin Syndrome
Authors: Taylor Woo Reviewers: Gurleen Chahal Usama Malik Laurie M. Parsons* * MD at time of publication
Early: Small vesicles progressing into superficial bullae
Late: Large, flaccid bullae erythematous base with “collarette” of scale at peripheral of ruptured lesion