Zenker’s Diverticulum: Pathogenesis and Clinical Findings
Author:
Juliette Hall
Reviewers:
Sunawer Aujla *Dr. Derrick Randall Illustrator: Erica Lindquist * MD at time of publication
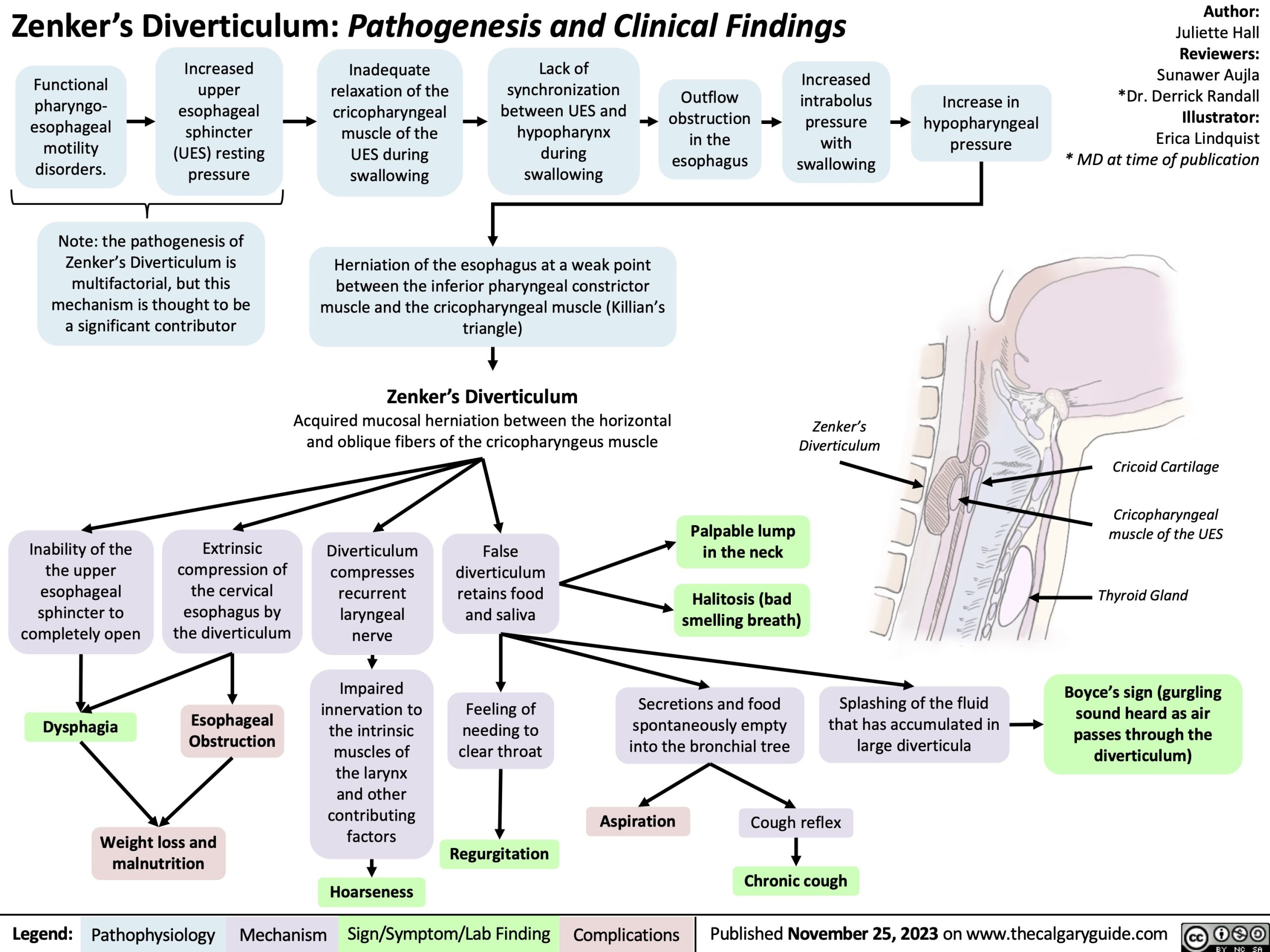
Functional pharyngo- esophageal motility disorders.
Increased upper esophageal sphincter (UES) resting pressure
Inadequate relaxation of the cricopharyngeal muscle of the UES during swallowing
Lack of synchronization between UES and hypopharynx during swallowing
Outflow obstruction in the esophagus
Increased intrabolus pressure with swallowing
Increase in hypopharyngeal pressure
Note: the pathogenesis of Zenker’s Diverticulum is multifactorial, but this mechanism is thought to be a significant contributor
Herniation of the esophagus at a weak point
between the inferior pharyngeal constrictor muscle and the cricopharyngeal muscle (Killian’s triangle)
Zenker’s Diverticulum
Acquired mucosal herniation between the horizontal and oblique fibers of the cricopharyngeus muscle
Inability of the the upper esophageal sphincter to completely open
Dysphagia
Extrinsic compression of the cervical esophagus by the diverticulum
Esophageal Obstruction
Diverticulum compresses recurrent laryngeal nerve
Impaired
innervation to
the intrinsic
muscles of
the larynx
and other
contributing
factors
False diverticulum retains food and saliva
Feeling of needing to clear throat
Palpable lump in the neck
Halitosis (bad smelling breath)
Secretions and food spontaneously empty into the bronchial tree
Splashing of the fluid that has accumulated in large diverticula
Cricoid Cartilage
Cricopharyngeal muscle of the UES
Thyroid Gland
Boyce’s sign (gurgling sound heard as air passes through the diverticulum)
Zenker’s Diverticulum
Weight loss and malnutrition
Aspiration
Cough reflex
Chronic cough
Regurgitation Hoarseness
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com