Wilson Disease: Pathogenesis and clinical findings
Authors: Sean Spence Reviewers: Danny Guo Yan Yu Crystal Liu Natalie Arnold Sam Lee* * MD at time of initial publication
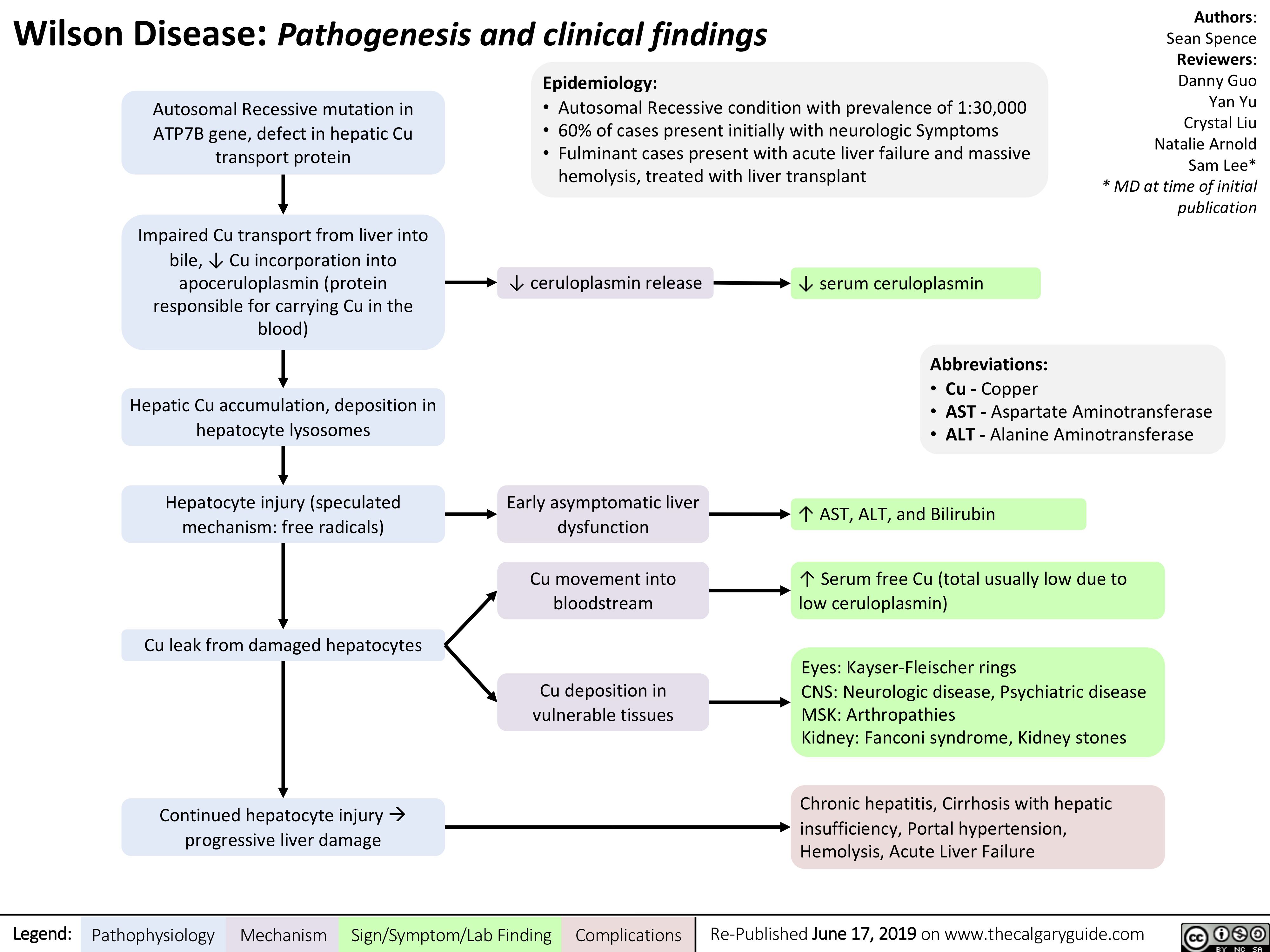
Autosomal Recessive mutation in ATP7B gene, defect in hepatic Cu transport protein
Impaired Cu transport from liver into bile, ↓ Cu incorporation into
apoceruloplasmin (protein responsible for carrying Cu in the blood)
Hepatic Cu accumulation, deposition in hepatocyte lysosomes
Hepatocyte injury (speculated mechanism: free radicals)
Cu leak from damaged hepatocytes
Epidemiology:
• Autosomal Recessive condition with prevalence of 1:30,000 • 60% of cases present initially with neurologic Symptoms
• Fulminant cases present with acute liver failure and massive
hemolysis, treated with liver transplant
↓ ceruloplasmin release ↓ serum ceruloplasmin
Early asymptomatic liver dysfunction
Cu movement into bloodstream
Cu deposition in vulnerable tissues
Abbreviations:
• Cu – Copper
• AST – Aspartate Aminotransferase • ALT – Alanine Aminotransferase
↑ AST, ALT, and Bilirubin
↑ Serum free Cu (total usually low due to low ceruloplasmin)
Eyes: Kayser-Fleischer rings
CNS: Neurologic disease, Psychiatric disease MSK: Arthropathies
Kidney: Fanconi syndrome, Kidney stones
Chronic hepatitis, Cirrhosis with hepatic insufficiency, Portal hypertension, Hemolysis, Acute Liver Failure
Continued hepatocyte injuryà progressive liver damage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 17, 2019 on www.thecalgaryguide.com