Varicocele: Pathogenesis and clinical findings
Authors: Luc Wittig Ryan Brenneis Reviewers: Alec Mitchell Darren Desantis* * MD at time of publication
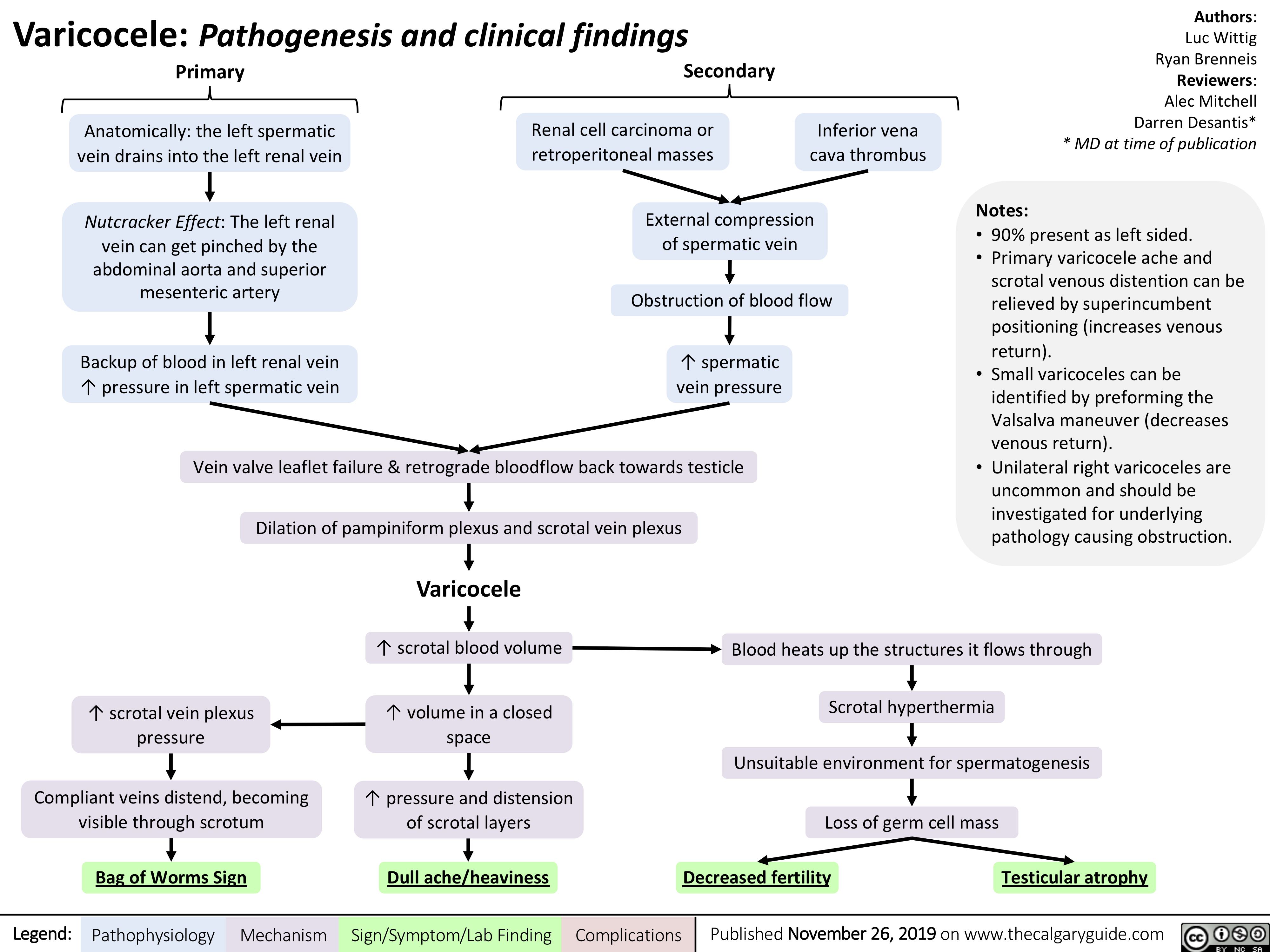
Notes:
• 90% present as left sided.
• Primary varicocele ache and
scrotal venous distention can be relieved by superincumbent positioning (increases venous return).
• Small varicoceles can be identified by preforming the Valsalva maneuver (decreases venous return).
• Unilateral right varicoceles are uncommon and should be investigated for underlying pathology causing obstruction.
Primary
Anatomically: the left spermatic vein drains into the left renal vein
Nutcracker Effect: The left renal vein can get pinched by the abdominal aorta and superior mesenteric artery
Backup of blood in left renal vein ↑ pressure in left spermatic vein
Secondary
Renal cell carcinoma or retroperitoneal masses
Inferior vena cava thrombus
External compression of spermatic vein
Obstruction of blood flow
↑ spermatic vein pressure
Vein valve leaflet failure & retrograde bloodflow back towards testicle
Dilation of pampiniform plexus and scrotal vein plexus
Varicocele
↑ scrotal blood volume ↑ volume in a closed
space
↑ pressure and distension of scrotal layers
↑ scrotal vein plexus pressure
Compliant veins distend, becoming visible through scrotum
Blood heats up the structures it flows through
Scrotal hyperthermia
Unsuitable environment for spermatogenesis
Loss of germ cell mass
Bag of Worms Sign
Dull ache/heaviness
Decreased fertility Testicular atrophy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com