Umbilical Cord Prolapse: Pathogenesis and clinical findings
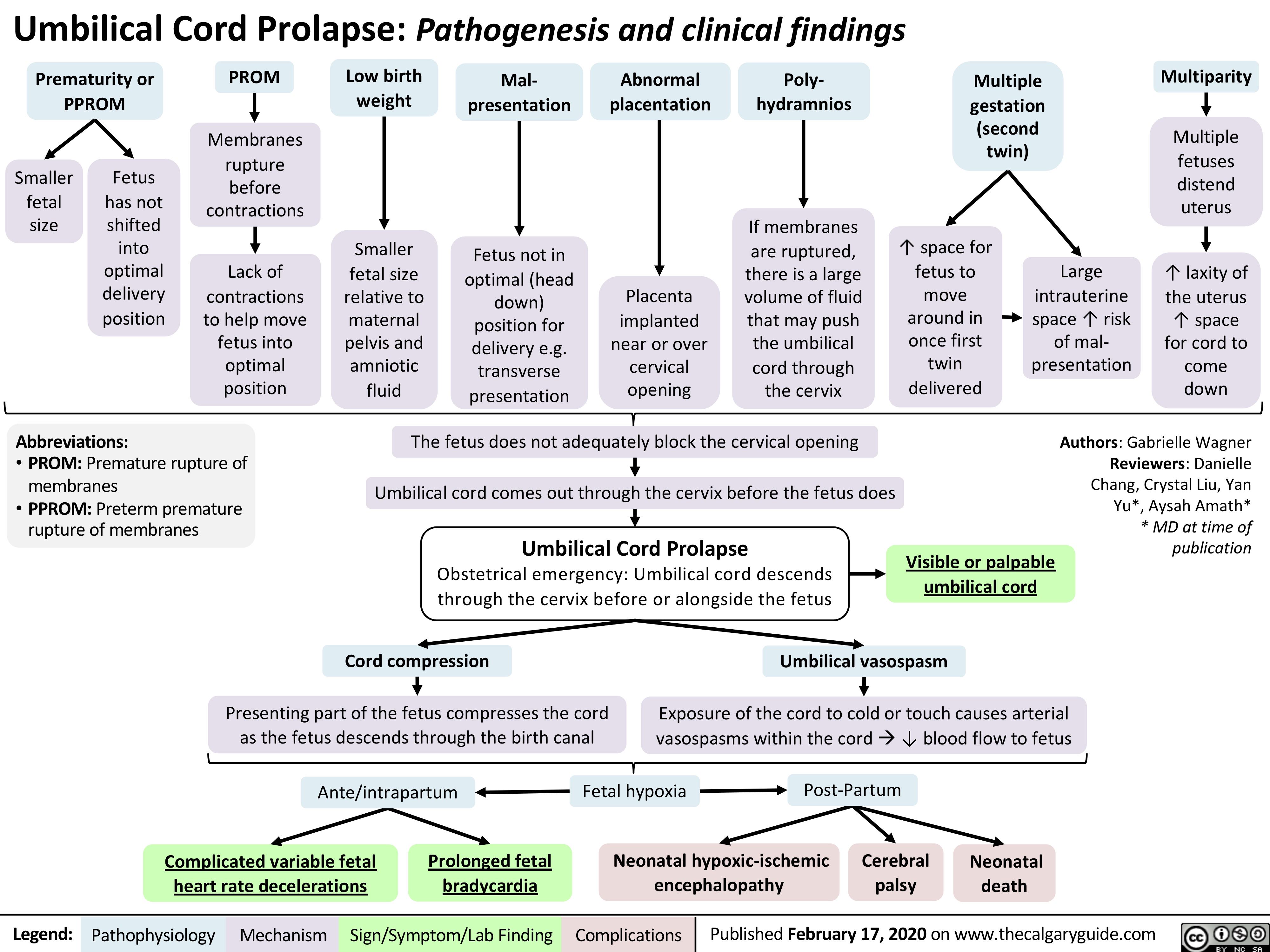
Prematurity or PPROM
PROM
Membranes rupture
before contractions
Lack of contractions to help move fetus into optimal position
rupture of
Low birth weight
Smaller fetal size
relative to maternal pelvis and amniotic fluid
Mal- presentation
Fetus not in optimal (head
down) position for delivery e.g. transverse presentation
Abnormal placentation
Poly- hydramnios
If membranes are ruptured, there is a large volume of fluid that may push the umbilical cord through the cervix
Multiple gestation
(second twin)
Multiparity
Multiple fetuses distend uterus
↑ laxity of the uterus ↑ space for cord to come down
Smaller fetal size
Fetus has not shifted into optimal delivery position
↑ space for fetus to move around in once first twin delivered
Placenta implanted near or over cervical opening
Large intrauterine space ↑ risk of mal- presentation
Abbreviations:
• PROM: Premature
The fetus does not adequately block the cervical opening Umbilical cord comes out through the cervix before the fetus does
Umbilical Cord Prolapse
Obstetrical emergency: Umbilical cord descends through the cervix before or alongside the fetus
Authors: Gabrielle Wagner Reviewers: Danielle Chang, Crystal Liu, Yan Yu*, Aysah Amath* * MD at time of publication
membranes
• PPROM: Preterm premature
rupture of membranes
Visible or palpable umbilical cord
Cord compression
Presenting part of the fetus compresses the cord as the fetus descends through the birth canal
Umbilical vasospasm
Exposure of the cord to cold or touch causes arterial vasospasms within the cordà↓ blood flow to fetus
Ante/intrapartum
Fetal hypoxia Post-Partum
Neonatal hypoxic-ischemic Cerebral Neonatal encephalopathy palsy death
Complicated variable fetal Prolonged fetal heart rate decelerations bradycardia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 17, 2020 on www.thecalgaryguide.com