Sustained Monomorphic Ventricular Tachycardia: Pathogenesis
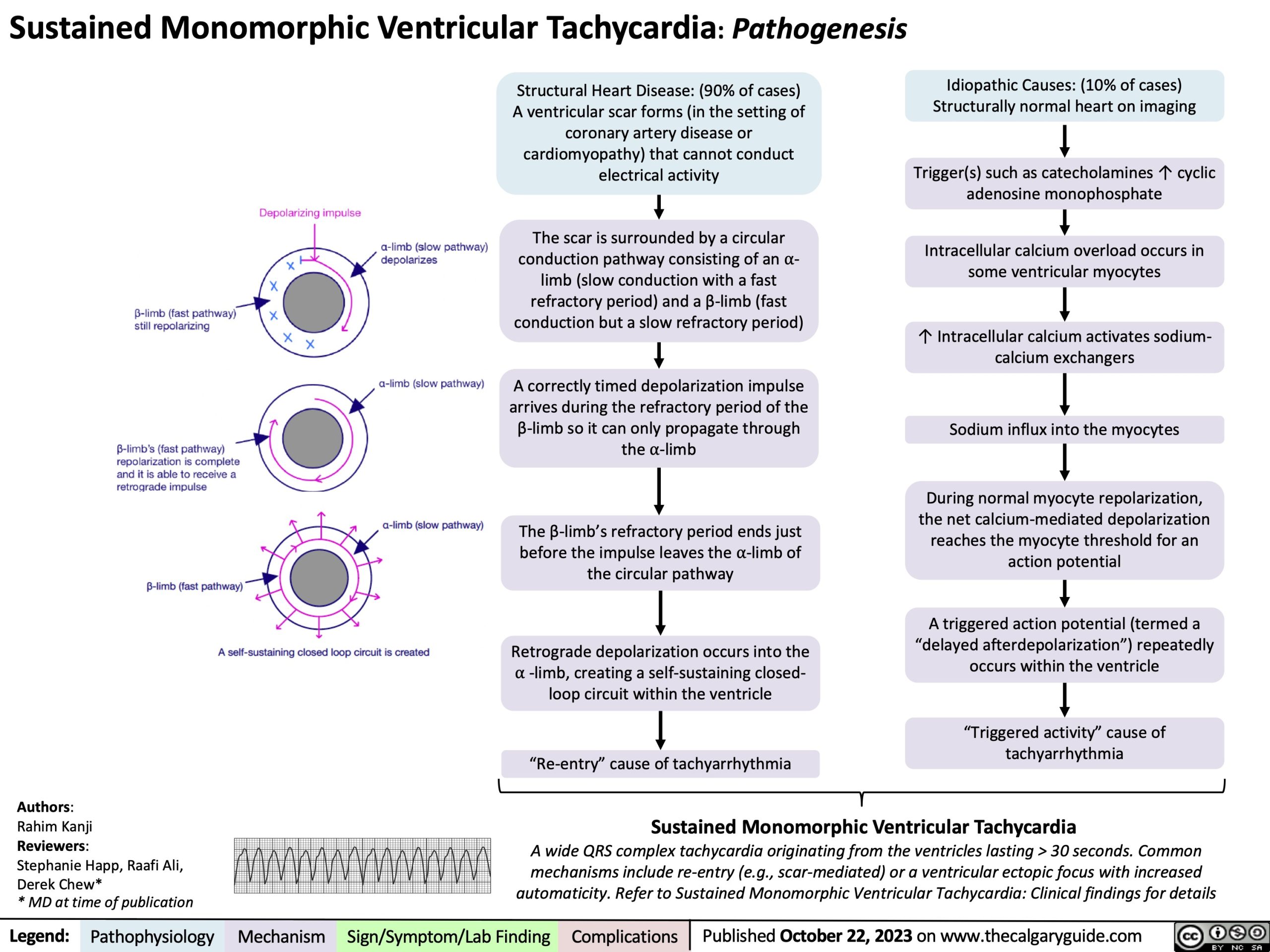
Structural Heart Disease: (90% of cases) A ventricular scar forms (in the setting of coronary artery disease or cardiomyopathy) that cannot conduct electrical activity
The scar is surrounded by a circular conduction pathway consisting of an ⍺- limb (slow conduction with a fast refractory period) and a β-limb (fast conduction but a slow refractory period)
A correctly timed depolarization impulse arrives during the refractory period of the β-limb so it can only propagate through the ⍺-limb
The β-limb’s refractory period ends just before the impulse leaves the ⍺-limb of the circular pathway
Retrograde depolarization occurs into the ⍺ -limb, creating a self-sustaining closed- loop circuit within the ventricle
“Re-entry” cause of tachyarrhythmia
Idiopathic Causes: (10% of cases) Structurally normal heart on imaging
Trigger(s) such as catecholamines ↑ cyclic adenosine monophosphate
Intracellular calcium overload occurs in some ventricular myocytes
↑ Intracellular calcium activates sodium- calcium exchangers
Sodium influx into the myocytes
During normal myocyte repolarization, the net calcium-mediated depolarization reaches the myocyte threshold for an action potential
A triggered action potential (termed a “delayed afterdepolarization”) repeatedly occurs within the ventricle
“Triggered activity” cause of tachyarrhythmia
Authors:
Rahim Kanji
Reviewers:
Stephanie Happ, Raafi Ali, Derek Chew*
* MD at time of publication
Sustained Monomorphic Ventricular Tachycardia
A wide QRS complex tachycardia originating from the ventricles lasting > 30 seconds. Common
mechanisms include re-entry (e.g., scar-mediated) or a ventricular ectopic focus with increased automaticity. Refer to Sustained Monomorphic Ventricular Tachycardia: Clinical findings for details
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 22, 2023 on www.thecalgaryguide.com