Summary of Acyanotic Congenital Heart Diseases (Left-to-Right Shunts)
Authors: Gaya Narendran, Winnie Nagesh Reviewers: Jack Fu, Usama Malik, Yan Yu*, Deborah Fruitman* * MD at time of publication
Asymptomatic M, ↑ respiratory tract infections, rarely: failure to thrive
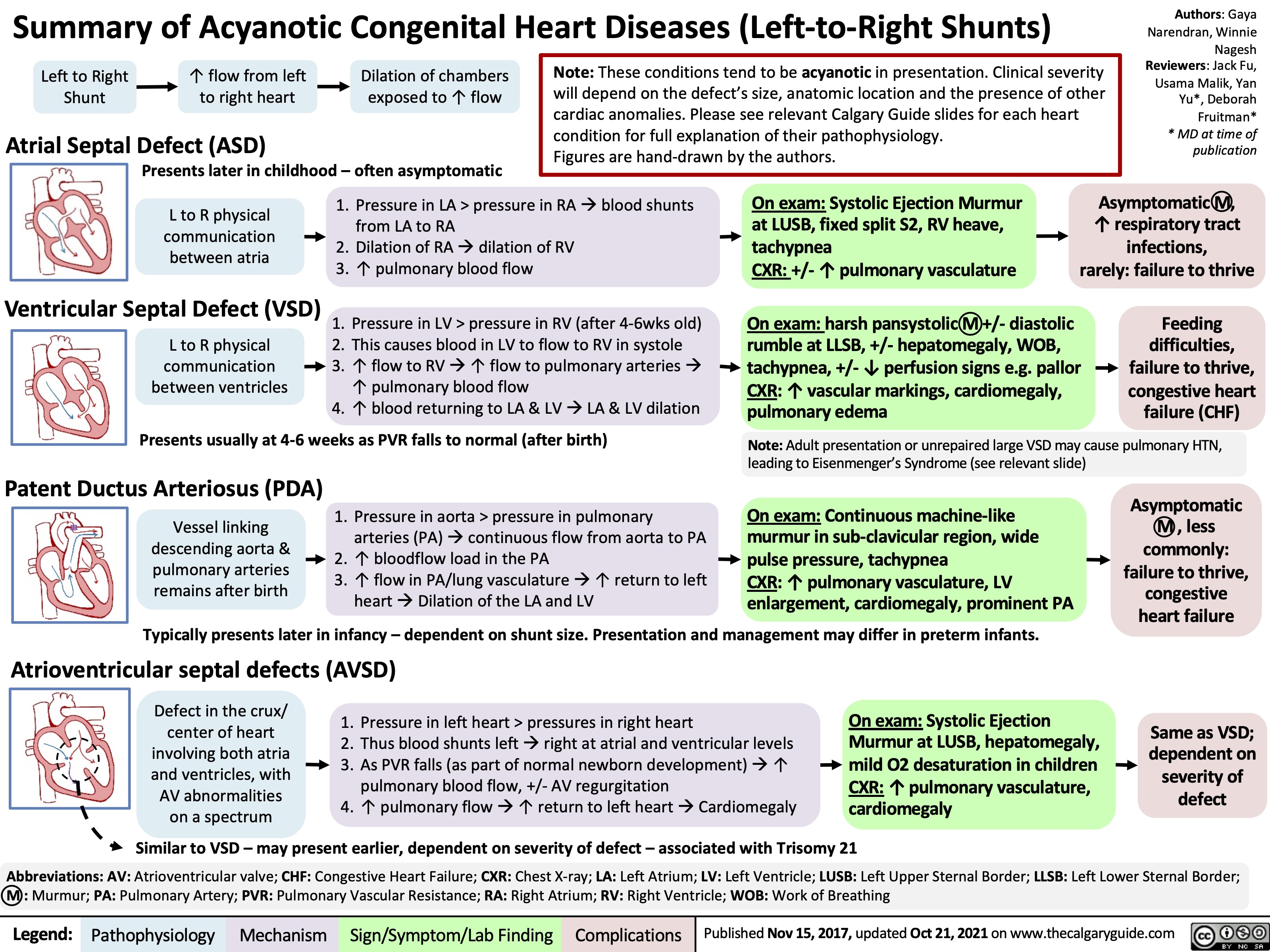
Left to Right Shunt
↑ flow from left to right heart
Dilation of chambers exposed to ↑ flow
Atrial Septal Defect (ASD)
Presents later in childhood – often asymptomatic
Note: These conditions tend to be acyanotic in presentation. Clinical severity will depend on the defect’s size, anatomic location and the presence of other cardiac anomalies. Please see relevant Calgary Guide slides for each heart condition for full explanation of their pathophysiology.
Figures are hand-drawn by the authors.
L to R physical communication between atria
1. Pressure in LA > pressure in RA à blood shunts from LA to RA
2. Dilation of RAàdilation of RV 3. ↑ pulmonary blood flow
On exam: Systolic Ejection Murmur at LUSB, fixed split S2, RV heave, tachypnea
CXR: +/- ↑ pulmonary vasculature
Ventricular Septal Defect (VSD) 1. Pressure in LV > pressure in RV (after 4-6wks old)
On exam: harsh pansystolic M +/- diastolic rumble at LLSB, +/- hepatomegaly, WOB, tachypnea, +/- ↓ perfusion signs e.g. pallor CXR: ↑ vascular markings, cardiomegaly, pulmonary edema
Feeding difficulties, failure to thrive, congestive heart failure (CHF)
L to R physical communication between ventricles
2. This causes blood in LV to flow to RV in systole
3. ↑ flow to RVà↑ flow to pulmonary arteriesà
↑ pulmonary blood flow
4. ↑ blood returning to LA & LVàLA & LV dilation
Presents usually at 4-6 weeks as PVR falls to normal (after birth) Patent Ductus Arteriosus (PDA)
1. Pressure in aorta > pressure in pulmonary arteries (PA) à continuous flow from aorta to PA
2. ↑ bloodflow load in the PA
3. ↑ flow in PA/lung vasculature à ↑ return to left
Note: Adult presentation or unrepaired large VSD may cause pulmonary HTN, leading to Eisenmenger’s Syndrome (see relevant slide)
Vessel linking descending aorta & pulmonary arteries remains after birth
On exam: Continuous machine-like murmur in sub-clavicular region, wide pulse pressure, tachypnea
CXR: ↑ pulmonary vasculature, LV enlargement, cardiomegaly, prominent PA
Asymptomatic M , less commonly: failure to thrive, congestive heart failure
heart à Dilation of the LA and LV
Typically presents later in infancy – dependent on shunt size. Presentation and management may differ in preterm infants.
Atrioventricular septal defects (AVSD)
Defect in the crux/ center of heart involving both atria and ventricles, with AV abnormalities on a spectrum
1. Pressure in left heart > pressures in right heart
2. Thus blood shunts left à right at atrial and ventricular levels 3. As PVR falls (as part of normal newborn development) à ↑
pulmonary blood flow, +/- AV regurgitation
4. ↑ pulmonary flow à ↑ return to left heart à Cardiomegaly
On exam: Systolic Ejection
Murmur at LUSB, hepatomegaly,
mild O2 desaturation in children
CXR: ↑ pulmonary vasculature,
cardiomegaly defect
Similar to VSD – may present earlier, dependent on severity of defect – associated with Trisomy 21
Abbreviations: AV: Atrioventricular valve; CHF: Congestive Heart Failure; CXR: Chest X-ray; LA: Left Atrium; LV: Left Ventricle; LUSB: Left Upper Sternal Border; LLSB: Left Lower Sternal Border; M : Murmur; PA: Pulmonary Artery; PVR: Pulmonary Vascular Resistance; RA: Right Atrium; RV: Right Ventricle; WOB: Work of Breathing
Same as VSD; dependent on severity of
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 15, 2017, updated Oct 21, 2021 on www.thecalgaryguide.com