Rotator Cuff Disease: Pathogenesis and clinical findings
Authors: Jared Topham Reviewers: Raafi Ali, Yan Yu*, Kelley DeSouza* * MD at time of publication
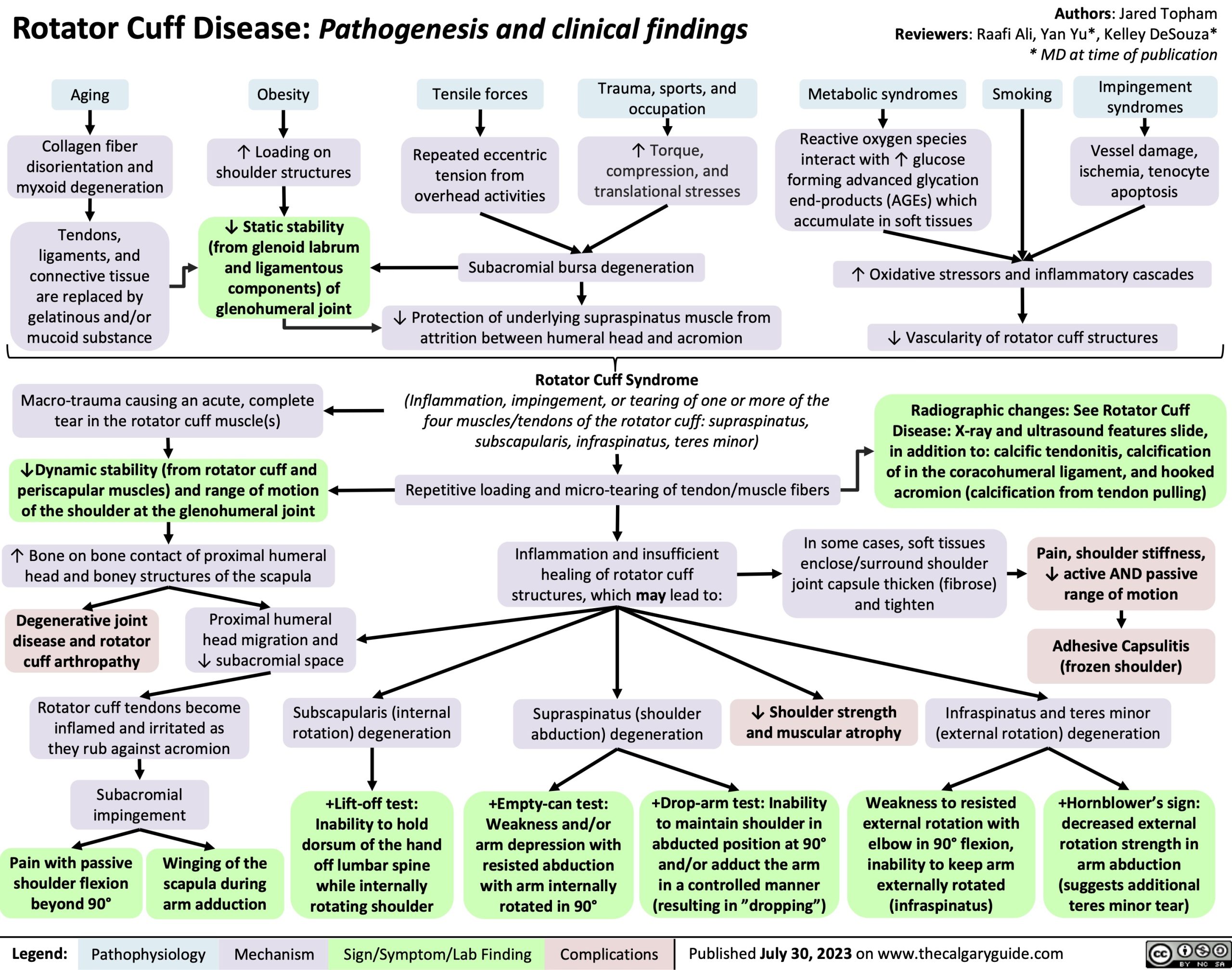
Aging
Collagen fiber disorientation and myxoid degeneration
Tendons, ligaments, and connective tissue are replaced by gelatinous and/or mucoid substance
Obesity
↑ Loading on shoulder structures
↓ Static stability (from glenoid labrum and ligamentous components) of glenohumeral joint
Tensile forces
Repeated eccentric tension from overhead activities
Trauma, sports, and occupation
↑ Torque, compression, and translational stresses
Metabolic syndromes
Reactive oxygen species
interact with ↑ glucose forming advanced glycation end-products (AGEs) which accumulate in soft tissues
Smoking
Impingement syndromes
Vessel damage, ischemia, tenocyte apoptosis
Macro-trauma causing an acute, complete tear in the rotator cuff muscle(s)
↓Dynamic stability (from rotator cuff and periscapular muscles) and range of motion of the shoulder at the glenohumeral joint
↑ Bone on bone contact of proximal humeral head and boney structures of the scapula
Subacromial bursa degeneration
↓ Protection of underlying supraspinatus muscle from attrition between humeral head and acromion
Rotator Cuff Syndrome
(Inflammation, impingement, or tearing of one or more of the four muscles/tendons of the rotator cuff: supraspinatus, subscapularis, infraspinatus, teres minor)
Repetitive loading and micro-tearing of tendon/muscle fibers
↑ Oxidative stressors and inflammatory cascades
↓ Vascularity of rotator cuff structures
Radiographic changes: See Rotator Cuff Disease: X-ray and ultrasound features slide, in addition to: calcific tendonitis, calcification of in the coracohumeral ligament, and hooked acromion (calcification from tendon pulling)
In some cases, soft tissues enclose/surround shoulder joint capsule thicken (fibrose) and tighten
Degenerative joint disease and rotator cuff arthropathy
Proximal humeral head migration and ↓ subacromial space
Inflammation and insufficient healing of rotator cuff structures, which may lead to:
Supraspinatus (shoulder abduction) degeneration
Pain, shoulder stiffness, ↓ active AND passive range of motion
Adhesive Capsulitis (frozen shoulder)
Infraspinatus and teres minor (external rotation) degeneration
Rotator cuff tendons become inflamed and irritated as they rub against acromion
Subacromial impingement
Subscapularis (internal rotation) degeneration
+Lift-off test: Inability to hold dorsum of the hand off lumbar spine while internally rotating shoulder
↓ Shoulder strength and muscular atrophy
Pain with passive shoulder flexion beyond 90°
Winging of the scapula during arm adduction
+Empty-can test: Weakness and/or arm depression with resisted abduction with arm internally rotated in 90°
+Drop-arm test: Inability to maintain shoulder in abducted position at 90° and/or adduct the arm in a controlled manner (resulting in ”dropping”)
Weakness to resisted external rotation with elbow in 90° flexion, inability to keep arm externally rotated (infraspinatus)
+Hornblower’s sign: decreased external rotation strength in arm abduction (suggests additional teres minor tear)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 30, 2023 on www.thecalgaryguide.com