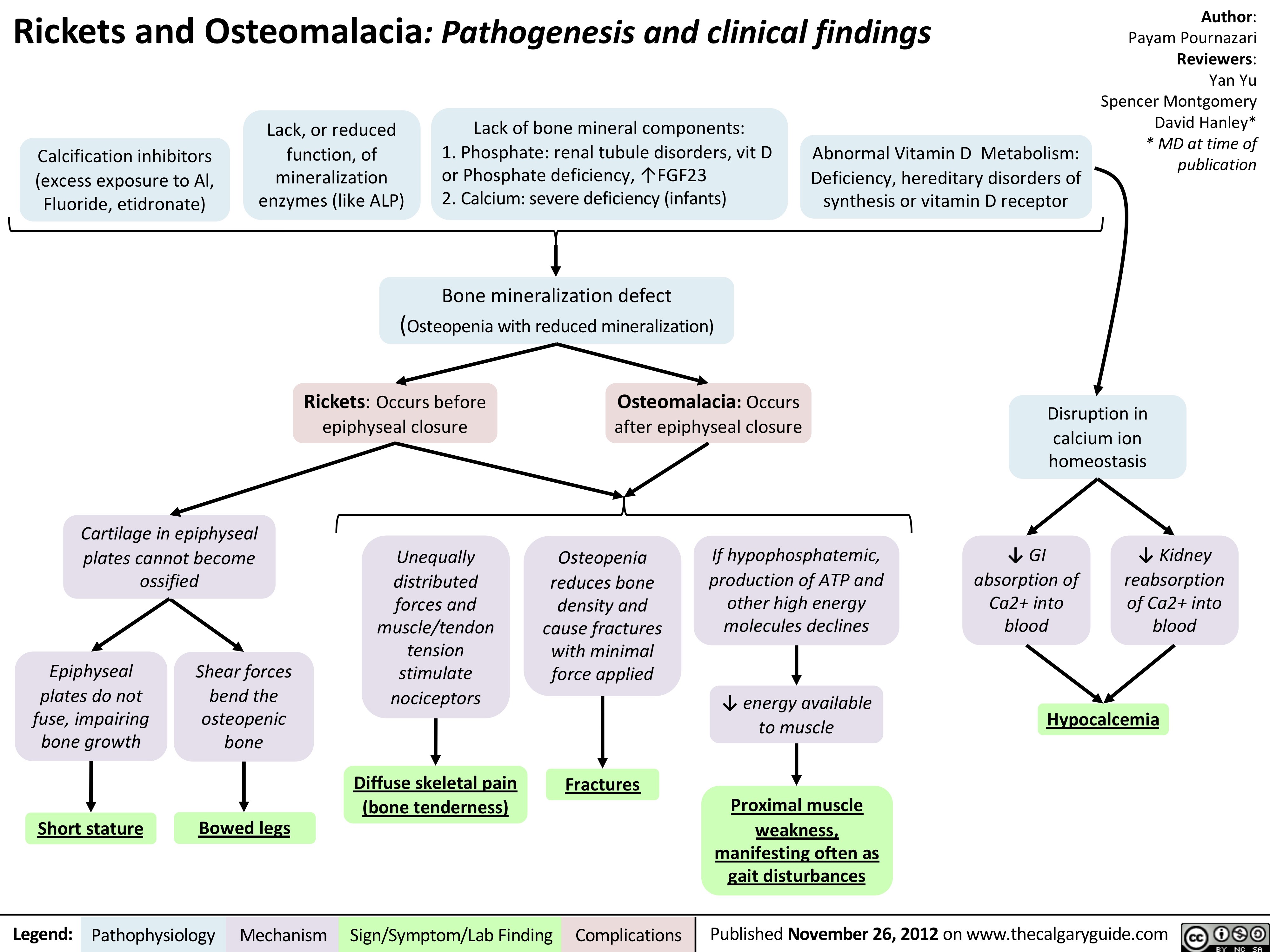
Hypocalcemia
Rickets and Osteomalacia: Pathogenesis and clinical findings
Abnormal Vitamin D Metabolism:
Deficiency, hereditary disorders of
synthesis or vitamin D receptor
Fractures
Proximal muscle
weakness,
manifesting often as
gait disturbances
Osteomalacia: Occurs
after epiphyseal closure
Bone mineralization defect
(Osteopenia with reduced mineralization)
Shear forces
bend the
osteopenic
bone
Short stature
Diffuse skeletal pain
(bone tenderness)
Osteopenia
reduces bone
density and
cause fractures
with minimal
force applied
If hypophosphatemic,
production of ATP and
other high energy
molecules declines
Unequally
distributed
forces and
muscle/tendon
tension
stimulate
nociceptors
Legend: Published November 26, 2012 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Calcification inhibitors
(excess exposure to Al,
Fluoride, etidronate)
Lack, or reduced
function, of
mineralization
enzymes (like ALP)
Lack of bone mineral components:
1. Phosphate: renal tubule disorders, vit D
or Phosphate deficiency, ↑FGF23
2. Calcium: severe deficiency (infants)
Rickets: Occurs before
epiphyseal closure
Epiphyseal
plates do not
fuse, impairing
bone growth
Bowed legs
Cartilage in epiphyseal
plates cannot become
ossified
Disruption in
calcium ion
homeostasis
↓ GI
absorption of
Ca2+ into
blood
↓ Kidney
reabsorption
of Ca2+ into
blood
↓ energy available
to muscle
Author:
Payam Pournazari
Reviewers:
Yan Yu
Spencer Montgomery
David Hanley*
* MD at time of
publication