Rapid Sequence Induction and Intubation (RSII): Clinical Approach
Authors:
Sandy Ly Reviewers: Wendy Yao
Melinda Davis*
* MD at time of publication
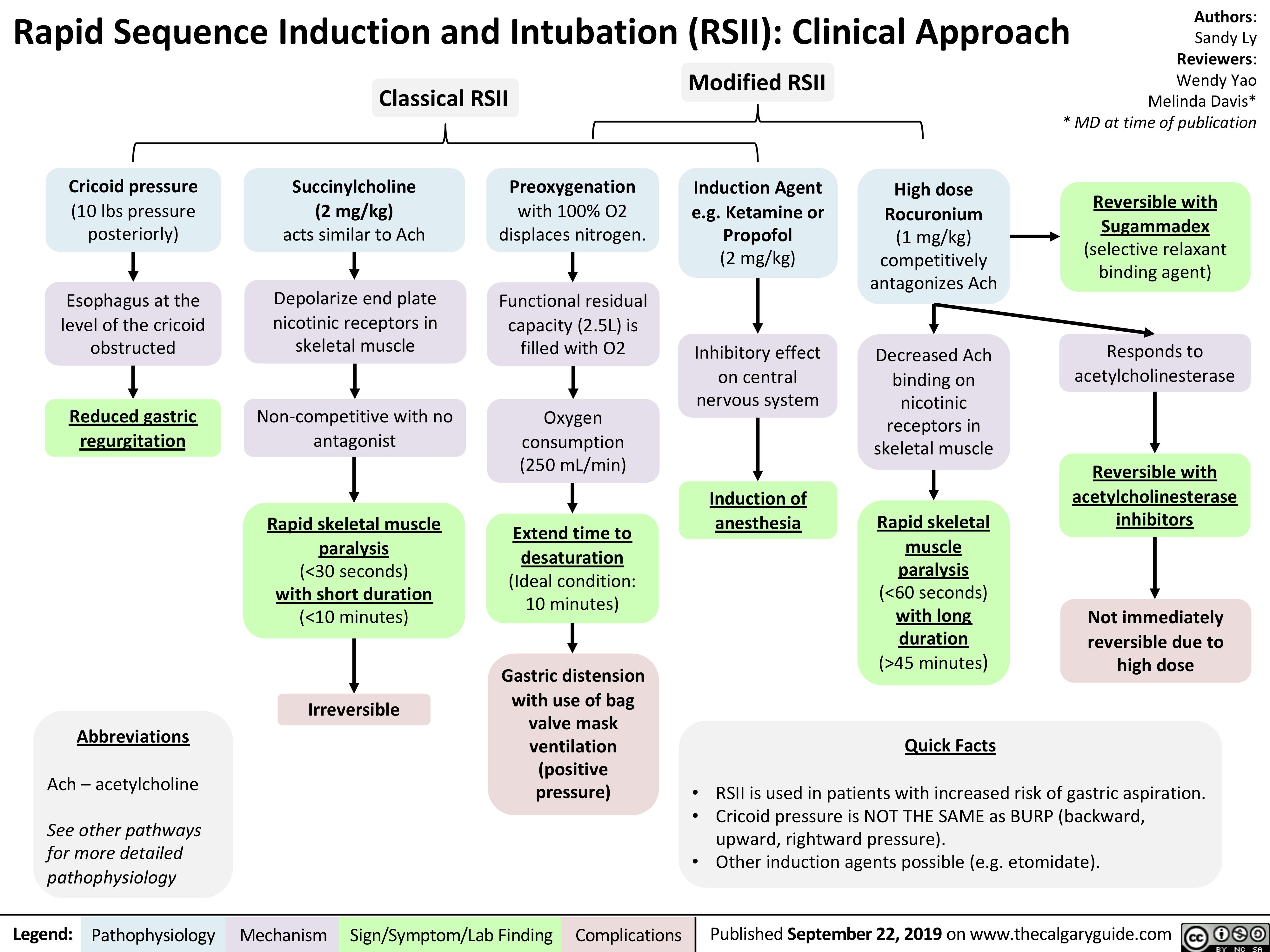
Reversible with Sugammadex (selective relaxant binding agent)
Responds to acetylcholinesterase
Reversible with acetylcholinesterase inhibitors
Not immediately reversible due to high dose
Classical RSII
Modified RSII
Induction Agent e.g. Ketamine or Propofol
(2 mg/kg)
Inhibitory effect on central nervous system
Cricoid pressure
(10 lbs pressure posteriorly)
Esophagus at the level of the cricoid obstructed
Reduced gastric regurgitation
Succinylcholine (2 mg/kg) acts similar to Ach
Depolarize end plate nicotinic receptors in skeletal muscle
Non-competitive with no antagonist
Rapid skeletal muscle paralysis
(<30 seconds) with short duration (<10 minutes)
Irreversible
Preoxygenation
with 100% O2 displaces nitrogen.
Functional residual capacity (2.5L) is filled with O2
Oxygen consumption (250 mL/min)
Extend time to desaturation (Ideal condition: 10 minutes)
Gastric distension with use of bag valve mask ventilation (positive pressure)
High dose Rocuronium (1 mg/kg) competitively antagonizes Ach
Decreased Ach binding on
nicotinic receptors in skeletal muscle
Rapid skeletal muscle paralysis (<60 seconds) with long duration (>45 minutes)
Quick Facts
Induction of anesthesia
Abbreviations
Ach – acetylcholine
See other pathways for more detailed pathophysiology
• •
•
RSII is used in patients with increased risk of gastric aspiration. Cricoid pressure is NOT THE SAME as BURP (backward, upward, rightward pressure).
Other induction agents possible (e.g. etomidate).
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 22, 2019 on www.thecalgaryguide.com