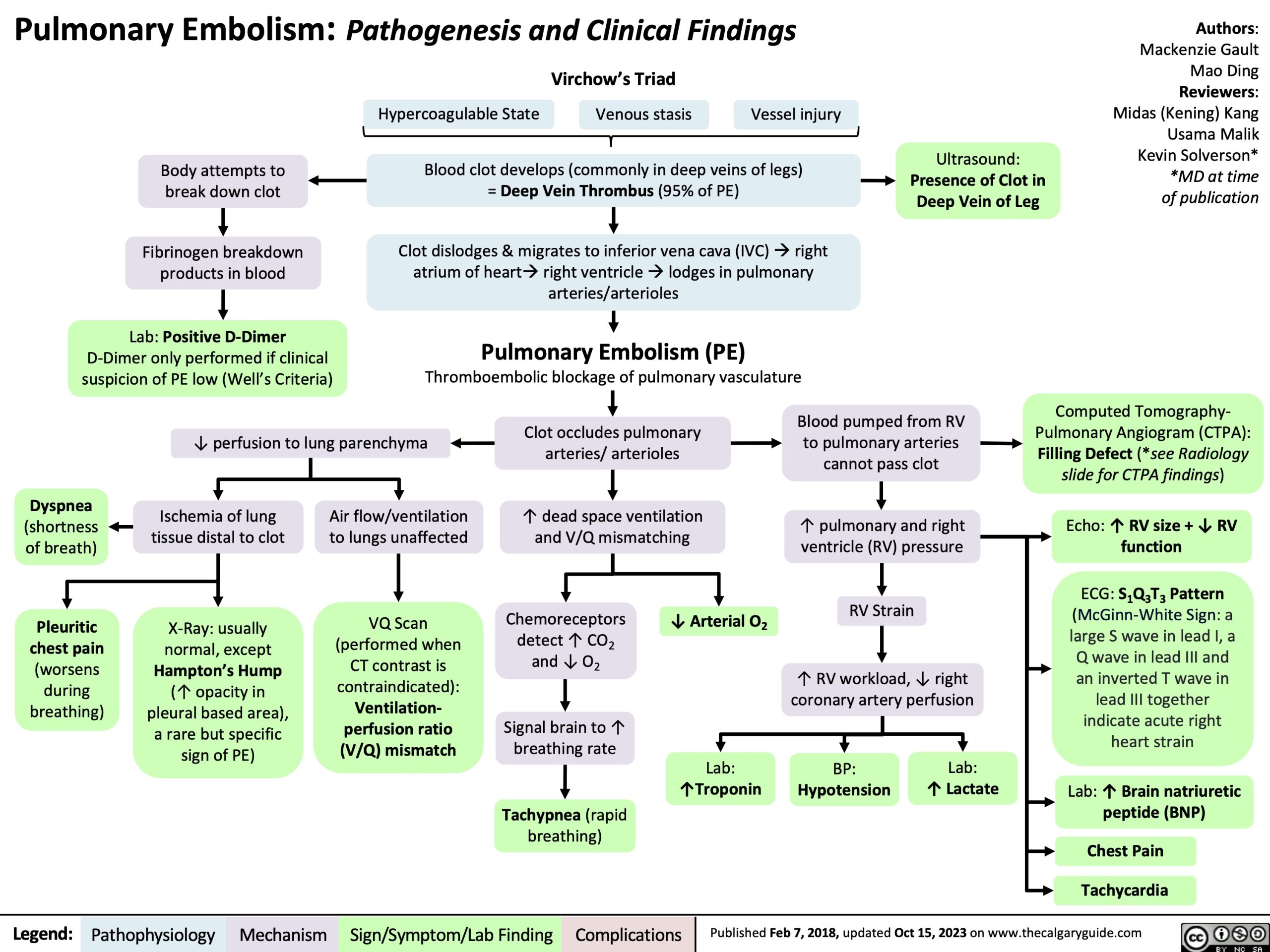
Pulmonary Embolism: Pathogenesis and Clinical Findings Virchow’s Triad
Body attempts to break down clot
Fibrinogen breakdown products in blood
Lab: Positive D-Dimer D-Dimer only performed if clinical suspicion of PE low (Well’s Criteria)
Authors: Mackenzie Gault Mao Ding Reviewers: Midas (Kening) Kang Usama Malik Kevin Solverson* *MD at time of publication
Hypercoagulable State
Blood clot develops (commonly in deep veins of legs)
Venous stasis
= Deep Vein Thrombus (95% of PE)
Vessel injury
Ultrasound:
Presence of Clot in Deep Vein of Leg
Clot dislodges & migrates to inferior vena cava (IVC)àright atrium of heartàright ventricleàlodges in pulmonary arteries/arterioles
Pulmonary Embolism (PE)
Thromboembolic blockage of pulmonary vasculature
↓ perfusion to lung parenchyma
Clot occludes pulmonary arteries/ arterioles
↑ dead space ventilation and V/Q mismatching
Blood pumped from RV to pulmonary arteries cannot pass clot
↑ pulmonary and right ventricle (RV) pressure
RV Strain
↑ RV workload, ↓ right coronary artery perfusion
Computed Tomography- Pulmonary Angiogram (CTPA): Filling Defect (*see Radiology slide for CTPA findings)
Echo: ↑ RV size + ↓ RV function
ECG: S1Q3T3 Pattern (McGinn-White Sign: a large S wave in lead I, a Q wave in lead III and an inverted T wave in lead III together indicate acute right heart strain
Lab: ↑ Brain natriuretic peptide (BNP)
Chest Pain Tachycardia
Dyspnea
(shortness of breath)
Pleuritic chest pain (worsens during breathing)
Ischemia of lung tissue distal to clot
X-Ray: usually normal, except Hampton’s Hump (↑ opacity in pleural based area), a rare but specific sign of PE)
Air flow/ventilation to lungs unaffected
VQ Scan (performed when CT contrast is contraindicated): Ventilation- perfusion ratio (V/Q) mismatch
Chemoreceptors detect ↑ CO2 and ↓ O2
Signal brain to ↑ breathing rate
Tachypnea (rapid breathing)
↓ Arterial O2
Lab:
↑Troponin
BP:
Hypotension
Lab:
↑ Lactate
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 7, 2018, updated Oct 15, 2023 on www.thecalgaryguide.com
Pulmonary Embolism: Pathogenesis and Laboratory Findings Virchow’s Triad
Authors: Mackenzie Gault Reviewers: Midas (Kening) Kang Usama Malik Kevin Solverson * * MD at time of publication
Body attempts to break down clot
Fibrinogen breakdown products in blood
Positive D-Dimer
↓ perfusion to lung parenchyma
Vessel injury = Deep Vein Thrombus (95% of PE)
Ultrasound:
Presence of Clot in Deep Vein of Leg
Notes:
Hypercoagulable State Venous stasis
Blood clot develops (commonly in deep veins of legs)
Clot dislodges, migrates to IVCàright atrium of heartà right ventricleàlodges in pulmonary artery
Pulmonary Embolism (PE):
Thromboembolic blockage of pulmonary vasculature
Clot occludes pulmonary artery/ arterioles
• D-Dimer is only performed if clinical suspicion of PE low (Well’s Criteria)
• CT-PA is the current diagnostic test for PE
• V/Q Scan is performed when CT contrast is contraindicated
• X-Ray is usually normal in PE (Except Hampton’s Hump, a rare but specific sign of PE)
Ischemia of lung tissue distal to clot
X-Ray:
Hampton’s Hump pleural based area of ↑ opacity
Air flow/ ventilation to lungs unaffected
Pleuritic Chest Pain + Dyspnea
VQ Scan: V/Q Mismatch
↑ dead space ventilation and V/Q mismatching
Chemoreceptors detect ↑ CO2 and ↓ O2
Signal brain to ↑ breathing rate
Tachypnea
↓ Arterial O2
Blood pumped from RV to pulmonary arteries cannot pass clot
↑ pulmonary and RV pressure
RV Strain
CT-PA: Filling Defect
Echo: ↑ RV size + ↓ RV Function
ECG: S1Q3T3 Pattern
Lab:↑ BNP Chest Pain Tachycardia
↑ RV work load, ↓ right coronary artery perfusion
Abbreviations:
• BNP – Brain Natriuretic Peptide
• CT-PA – Computed Tomography-Pulmonary Angiogram
• ECG – Electrocardiogram
• IVC – Inferior Vena Cava
• RV – Right Ventricle
• V/Q – Ventilation-Perfusion ratio
↑ Troponin
Hypotension
↑ Lactate
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 07, 2018 on www.thecalgaryguide.com