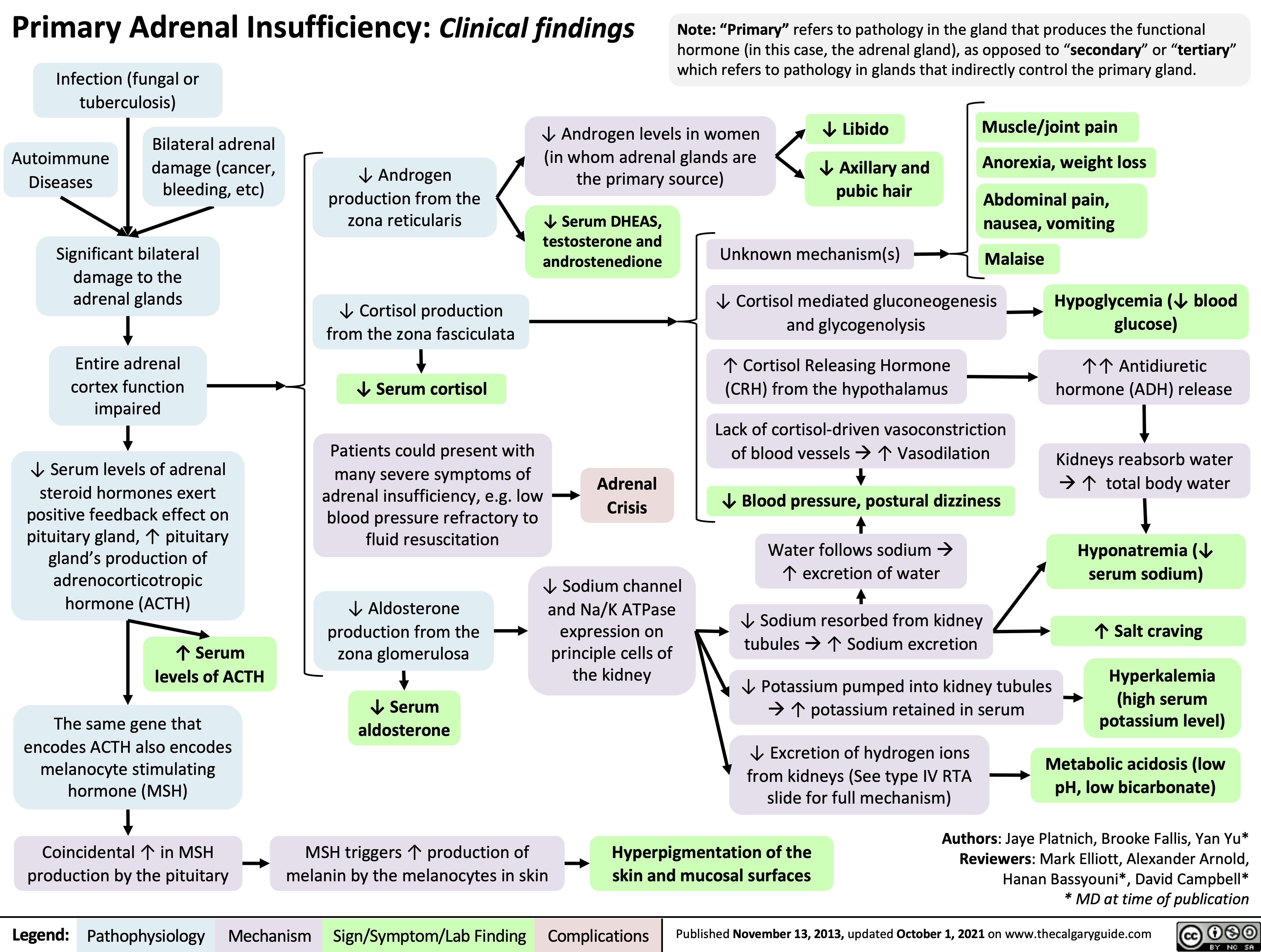
Primary Adrenal Insufficiency: Clinical findings Infection (fungal or
tuberculosis)
Note: “Primary” refers to pathology in the gland that produces the functional hormone (in this case, the adrenal gland), as opposed to “secondary” or “tertiary” which refers to pathology in glands that indirectly control the primary gland.
Bilateral adrenal Autoimmune damage (cancer,
↓ Androgen levels in women (in whom adrenal glands are the primary source)
↓ Libido
↓ Axillary and pubic hair
Muscle/joint pain
Anorexia, weight loss
Abdominal pain, nausea, vomiting
Diseases bleeding, etc)
↓ Androgen production from the zona reticularis
↓ Cortisol production from the zona fasciculata
↓ Serum cortisol
Patients could present with many severe symptoms of
adrenal insufficiency, e.g. low blood pressure refractory to fluid resuscitation
Significant bilateral damage to the adrenal glands
Entire adrenal cortex function impaired
↓ Serum levels of adrenal steroid hormones exert positive feedback effect on pituitary gland, ↑ pituitary gland’s production of adrenocorticotropic hormone (ACTH)
↑ Serum levels of ACTH
The same gene that encodes ACTH also encodes melanocyte stimulating hormone (MSH)
Coincidental ↑ in MSH production by the pituitary
↓ Serum DHEAS, testosterone and androstenedione
Unknown mechanism(s)
Malaise
Adrenal Crisis
↓ Cortisol mediated gluconeogenesis and glycogenolysis
↑ Cortisol Releasing Hormone (CRH) from the hypothalamus
Lack of cortisol-driven vasoconstriction of blood vesselsà↑ Vasodilation
↓ Blood pressure, postural dizziness
Water follows sodiumà ↑ excretion of water
↓ Sodium resorbed from kidney tubulesà↑ Sodium excretion
↓ Potassium pumped into kidney tubules à↑ potassium retained in serum
Hypoglycemia (↓ blood glucose)
↑↑ Antidiuretic hormone (ADH) release
Kidneys reabsorb water à↑ total body water
Hyponatremia (↓ serum sodium)
↑ Salt craving
Hyperkalemia (high serum potassium level)
↓ Aldosterone production from the zona glomerulosa
↓ Serum aldosterone
MSH triggers ↑ production of melanin by the melanocytes in skin
↓ Excretion of hydrogen ions from kidneys (See type IV RTA slide for full mechanism)
Metabolic acidosis (low pH, low bicarbonate)
↓ Sodium channel and Na/K ATPase
expression on principle cells of the kidney
Hyperpigmentation of the skin and mucosal surfaces
Authors: Jaye Platnich, Brooke Fallis, Yan Yu* Reviewers: Mark Elliott, Alexander Arnold, Hanan Bassyouni*, David Campbell* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 13, 2013, updated October 1, 2021 on www.thecalgaryguide.com