Start of ECG waveform Physiology of the Normal ECG Waveform (Lead II)
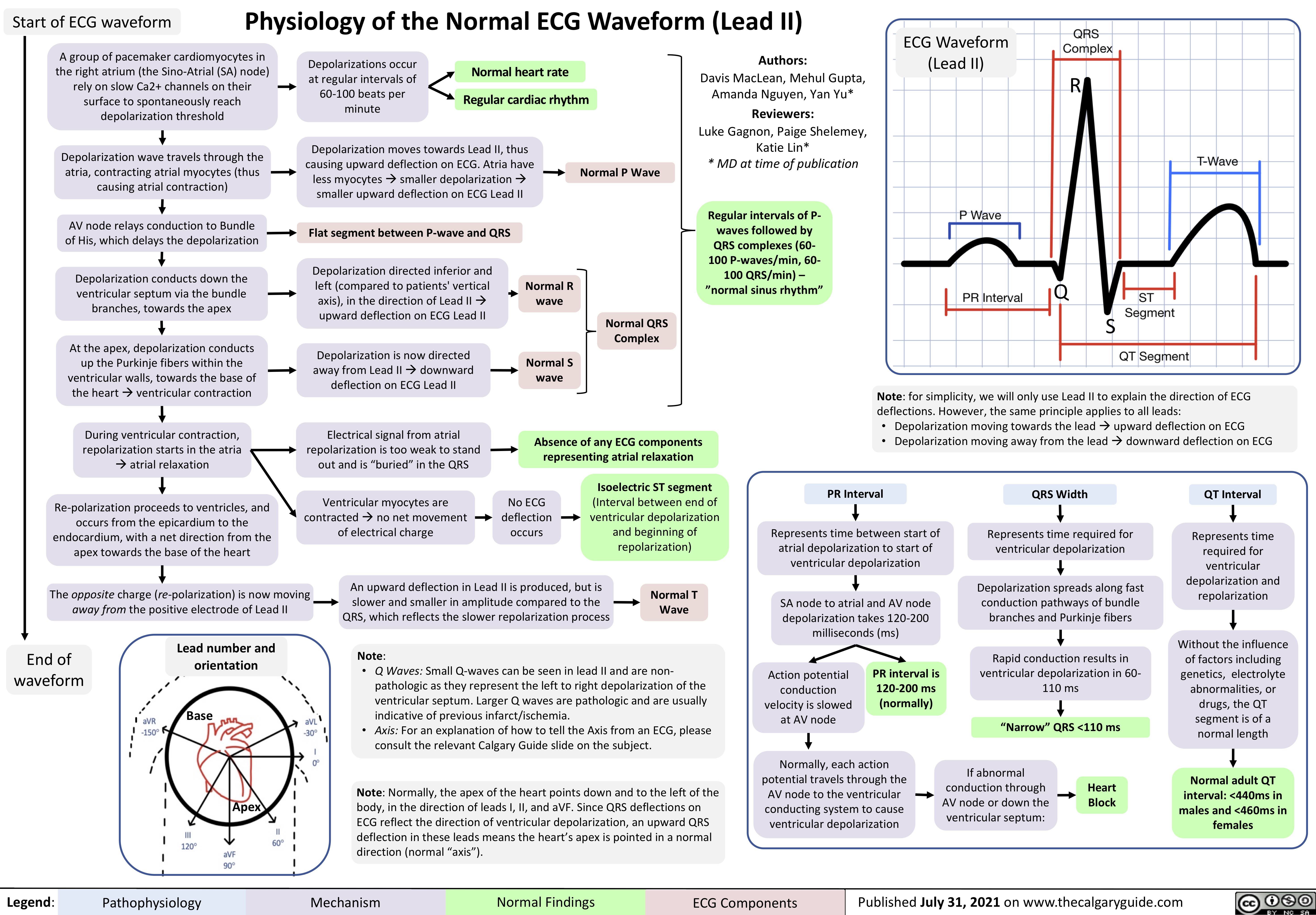
ECG Waveform (Lead II)
A group of pacemaker cardiomyocytes in the right atrium (the Sino-Atrial (SA) node) rely on slow Ca2+ channels on their surface to spontaneously reach depolarization threshold
Depolarization wave travels through the atria, contracting atrial myocytes (thus causing atrial contraction)
AV node relays conduction to Bundle of His, which delays the depolarization
Depolarization conducts down the ventricular septum via the bundle branches, towards the apex
At the apex, depolarization conducts up the Purkinje fibers within the ventricular walls, towards the base of the heartàventricular contraction
During ventricular contraction, repolarization starts in the atria àatrial relaxation
Re-polarization proceeds to ventricles, and occurs from the epicardium to the endocardium, with a net direction from the apex towards the base of the heart
Depolarizations occur at regular intervals of 60-100 beats per minute
Normal heart rate Regular cardiac rhythm
Authors:
Davis MacLean, Mehul Gupta, Amanda Nguyen, Yan Yu*
Reviewers:
Luke Gagnon, Paige Shelemey, Katie Lin*
* MD at time of publication
Regular intervals of P- waves followed by QRS complexes (60- 100 P-waves/min, 60- 100 QRS/min) – ”normal sinus rhythm”
R
Depolarization moves towards Lead II, thus causing upward deflection on ECG. Atria have less myocytesàsmaller depolarizationà smaller upward deflection on ECG Lead II
Normal P Wave
Flat segment between P-wave and QRS
Depolarization directed inferior and left (compared to patients’ vertical axis), in the direction of Lead IIà upward deflection on ECG Lead II
Depolarization is now directed away from Lead IIàdownward deflection on ECG Lead II
Electrical signal from atrial repolarization is too weak to stand out and is “buried” in the QRS
Ventricular myocytes are contractedàno net movement of electrical charge
Normal R wave
Normal S wave
Q
Normal QRS Complex
S
Note: for simplicity, we will only use Lead II to explain the direction of ECG deflections. However, the same principle applies to all leads:
Depolarization moving towards the leadàupward deflection on ECG Depolarization moving away from the leadàdownward deflection on ECG
Absence of any ECG components representing atrial relaxation
• •
PR Interval
Represents time between start of atrial depolarization to start of ventricular depolarization
SA node to atrial and AV node depolarization takes 120-200 milliseconds (ms)
No ECG deflection occurs
Isoelectric ST segment
(Interval between end of ventricular depolarization and beginning of repolarization)
QRS Width
Represents time required for ventricular depolarization
Depolarization spreads along fast conduction pathways of bundle branches and Purkinje fibers
Rapid conduction results in ventricular depolarization in 60- 110 ms
“Narrow” QRS <110 ms
QT Interval
Represents time required for ventricular depolarization and repolarization
Without the influence of factors including genetics, electrolyte abnormalities, or drugs, the QT segment is of a normal length
Normal adult QT interval: <440ms in males and <460ms in females
The opposite charge (re-polarization) is now moving away from the positive electrode of Lead II
An upward deflection in Lead II is produced, but is slower and smaller in amplitude compared to the QRS, which reflects the slower repolarization process
Normal T Wave
End of waveform
Lead number and orientation
Base
Apex
Note:
• Q Waves: Small Q-waves can be seen in lead II and are non-
pathologic as they represent the left to right depolarization of the ventricular septum. Larger Q waves are pathologic and are usually indicative of previous infarct/ischemia.
• Axis: For an explanation of how to tell the Axis from an ECG, please consult the relevant Calgary Guide slide on the subject.
Note: Normally, the apex of the heart points down and to the left of the body, in the direction of leads I, II, and aVF. Since QRS deflections on ECG reflect the direction of ventricular depolarization, an upward QRS deflection in these leads means the heart’s apex is pointed in a normal direction (normal “axis”).
Action potential conduction velocity is slowed at AV node
PR interval is 120-200 ms (normally)
Normally, each action potential travels through the AV node to the ventricular conducting system to cause ventricular depolarization
If abnormal conduction through AV node or down the ventricular septum:
Heart Block
Legend:
Pathophysiology
Mechanism
Normal Findings
ECG Components
Published July 31, 2021 on www.thecalgaryguide.com