Pertussis: Pathogenesis, clinical findings and complications
Authors: Morgan Sosniuk Yan Yu* Reviewers: Jessica Tjong Crystal Liu Timothy Fu Luis Murguia-Favela* * MD at time of publication
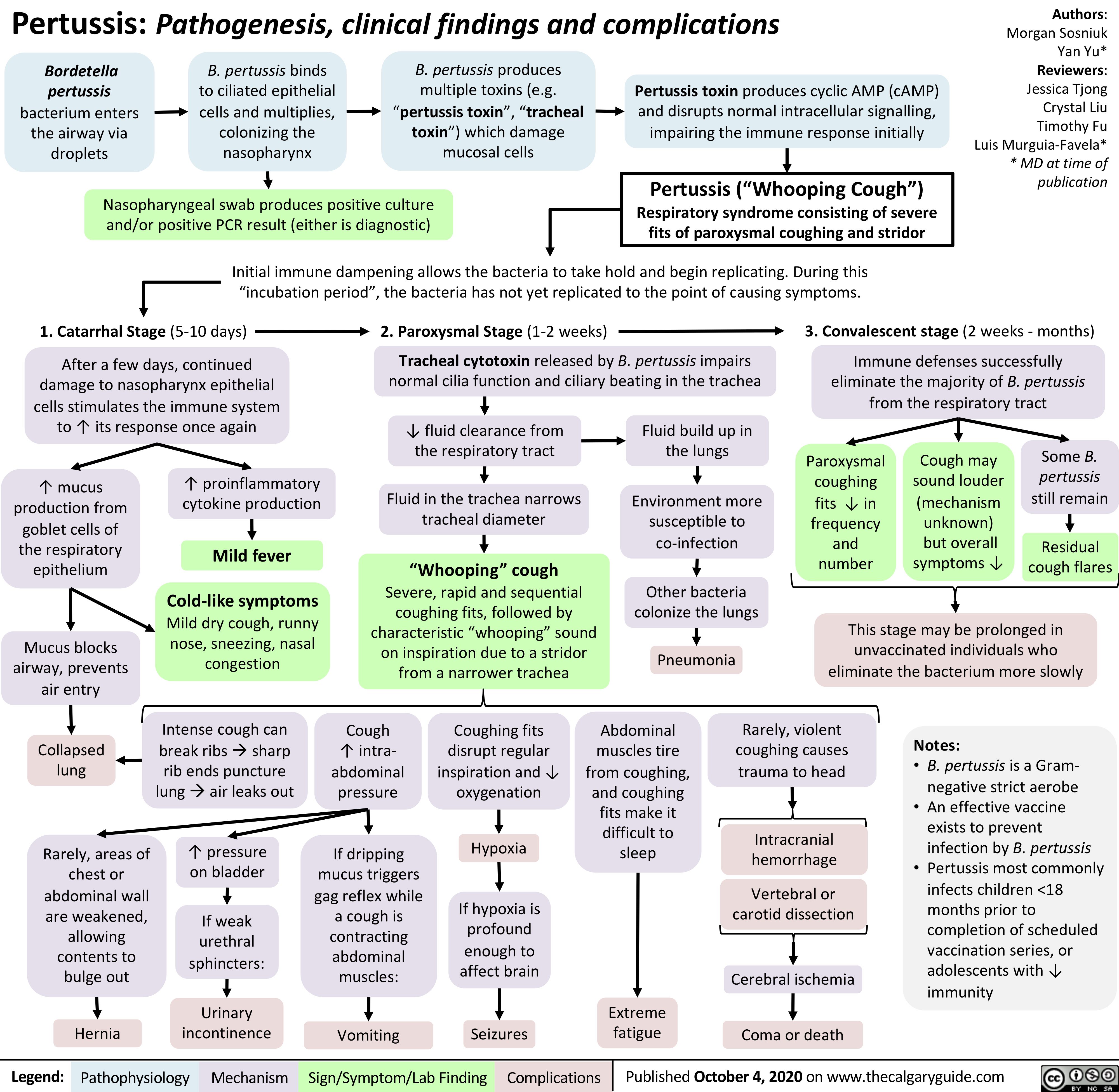
Bordetella pertussis bacterium enters the airway via droplets
B. pertussis binds to ciliated epithelial cells and multiplies, colonizing the nasopharynx
B. pertussis produces multiple toxins (e.g. “pertussis toxin”, “tracheal toxin”) which damage mucosal cells
Pertussis toxin produces cyclic AMP (cAMP) and disrupts normal intracellular signalling, impairing the immune response initially
Pertussis (“Whooping Cough”) Respiratory syndrome consisting of severe fits of paroxysmal coughing and stridor
Nasopharyngeal swab produces positive culture and/or positive PCR result (either is diagnostic)
Initial immune dampening allows the bacteria to take hold and begin replicating. During this “incubation period”, the bacteria has not yet replicated to the point of causing symptoms.
1. Catarrhal Stage (5-10 days) After a few days, continued
damage to nasopharynx epithelial cells stimulates the immune system to ↑ its response once again
2. Paroxysmal Stage (1-2 weeks)
Tracheal cytotoxin released by B. pertussis impairs normal cilia function and ciliary beating in the trachea
3. Convalescent stage (2 weeks – months) Immune defenses successfully
eliminate the majority of B. pertussis from the respiratory tract
↑ mucus production from goblet cells of the respiratory epithelium
Mucus blocks airway, prevents air entry
Collapsed lung
Rarely, areas of chest or abdominal wall are weakened, allowing contents to bulge out
Hernia
↑ proinflammatory cytokine production
Mild fever
Cold-like symptoms
Mild dry cough, runny nose, sneezing, nasal congestion
↓ fluid clearance from the respiratory tract
Fluid in the trachea narrows tracheal diameter
“Whooping” cough
Severe, rapid and sequential coughing fits, followed by characteristic “whooping” sound on inspiration due to a stridor from a narrower trachea
Fluid build up in the lungs
Environment more susceptible to co-infection
Other bacteria colonize the lungs
Pneumonia
Paroxysmal coughing fits ↓ in frequency and number
Cough may sound louder (mechanism unknown)
but overall symptoms ↓
Some B. pertussis still remain
Residual cough flares
This stage may be prolonged in unvaccinated individuals who eliminate the bacterium more slowly
Intense cough can break ribsàsharp rib ends puncture lungàair leaks out
↑ pressure on bladder
If weak urethral sphincters:
Urinary incontinence
Cough ↑ intra- abdominal pressure
If dripping mucus triggers gag reflex while a cough is contracting abdominal muscles:
Vomiting
Coughing fits disrupt regular inspiration and ↓ oxygenation
Hypoxia
If hypoxia is profound enough to affect brain
Seizures
Abdominal muscles tire from coughing, and coughing fits make it difficult to sleep
Extreme fatigue
Rarely, violent coughing causes trauma to head
Intracranial hemorrhage
Vertebral or carotid dissection
Cerebral ischemia Coma or death
Notes:
• B. pertussis is a Gram- negative strict aerobe
• An effective vaccine exists to prevent infection by B. pertussis
• Pertussis most commonly infects children <18 months prior to completion of scheduled vaccination series, or adolescents with ↓ immunity
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 4, 2020 on www.thecalgaryguide.com
Include a sentence!
When sending in the final draft of a slide, please include in the email a sentence that describes the slide that you've produced in detail. This will help us boost the relevance of the slide with search engines.
E.g., Disease X presents with symptom Y due to pathophysiology Z
Pertussis presents with fits of severe paroxysmal coughing due to impaired mucociliary clearance.