Yu Yan – MI Findings on Physical Exam – FINAL.pptx
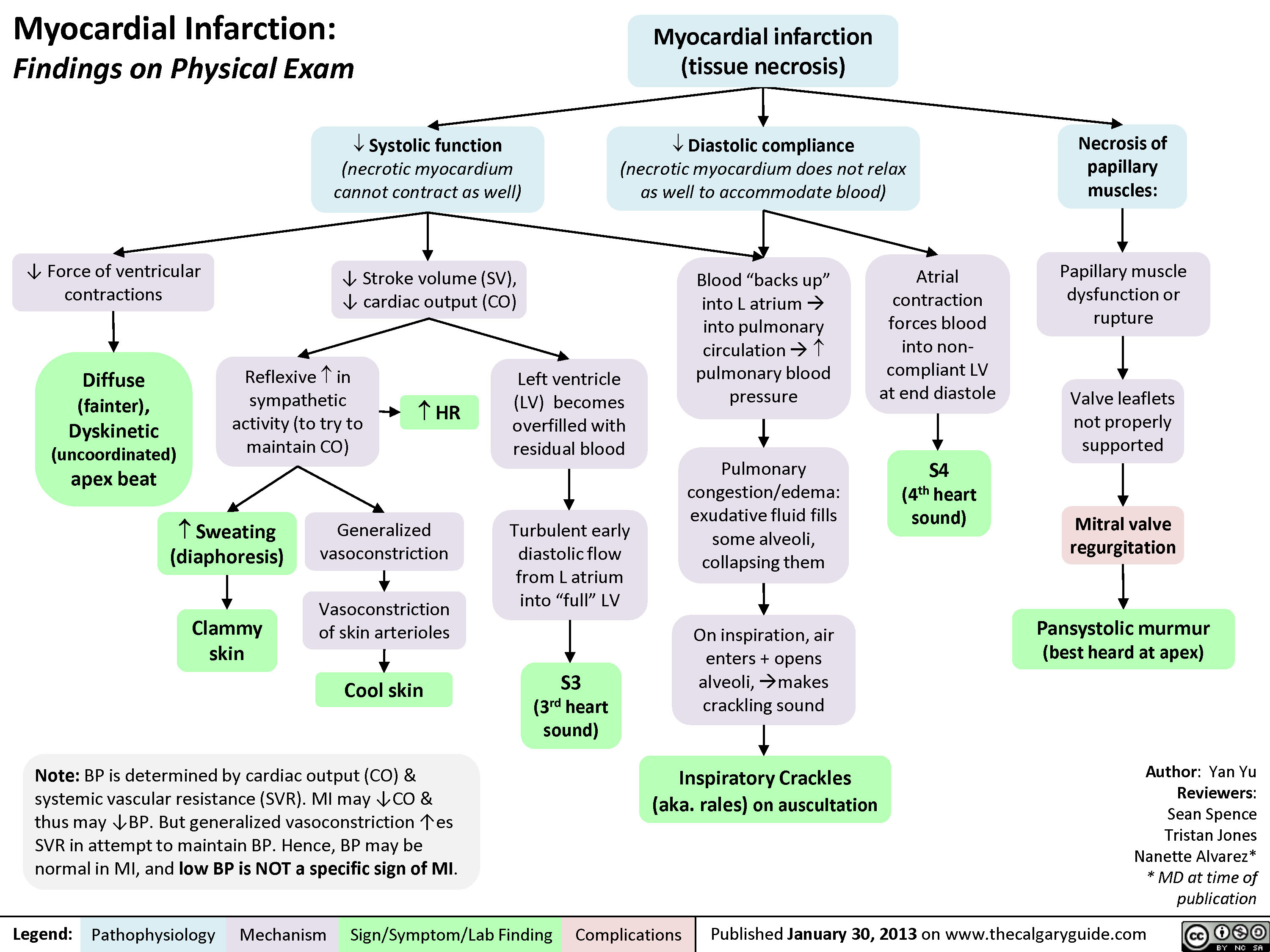
Myocardial Infarction: Findings on Physical Exam Author: Yan YuReviewers:Sean SpenceTristan JonesNanette Alvarez** MD at time of publication Systolic function(necrotic myocardium cannot contract as well) Diastolic compliance (necrotic myocardium does not relax as well to accommodate blood)Necrosis of papillary muscles:S4(4th heart sound)? Force of ventricular contractionsMitral valve regurgitationBlood “backs up” into L atrium ? into pulmonary circulation ? ? pulmonary blood pressureReflexive ? in sympathetic activity (to try to maintain CO)Inspiratory Crackles (aka. rales) on auscultationClammy skinAtrial contraction forces blood into non-compliant LV at end diastole? Stroke volume (SV), ? cardiac output (CO)On inspiration, air enters + opens alveoli, ?makes crackling soundPulmonary congestion/edema: exudative fluid fills some alveoli, collapsing themPansystolic murmur (best heard at apex)Diffuse (fainter), Dyskinetic (uncoordinated)apex beatMyocardial infarction (tissue necrosis)Note: BP is determined by cardiac output (CO) & systemic vascular resistance (SVR). MI may ?CO & thus may ?BP. But generalized vasoconstriction ?es SVR in attempt to maintain BP. Hence, BP may be normal in MI, and low BP is NOT a specific sign of MI.Generalized vasoconstrictionVasoconstriction of skin arteriolesCool skin? HR Turbulent early diastolic flow from L atrium into “full” LVS3(3rd heart sound)Left ventricle (LV) becomes overfilled with residual bloodPapillary muscle dysfunction or ruptureValve leaflets not properly supported? Sweating (diaphoresis)Legend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications
103 kB / 210 words