Molluscum Contagiosum: Pathogenesis and clinical findings
Authors: Kara Hawker Reviewers: Taylor Woo Sean Doherty Dr. Laurie Parsons* * MD at time of publication
4 main subtypes of molluscipox virus (MCV):
• MCV I *more prevalent than other
subtypes except in
immunocompromised individuals
• MCVII
• MCV III
• MCVIV
Abbreviations:
– MCV: Molluscum contagiosum virus – NF-KB: nuclear factor kappa-light- chain-enhancer of activated B cells
(a transcription factor regulating genes responsible for innate & adaptive immune responses)
Sexually active adults: abdomen, genitals, inner thighs Children: face, trunk, limbs
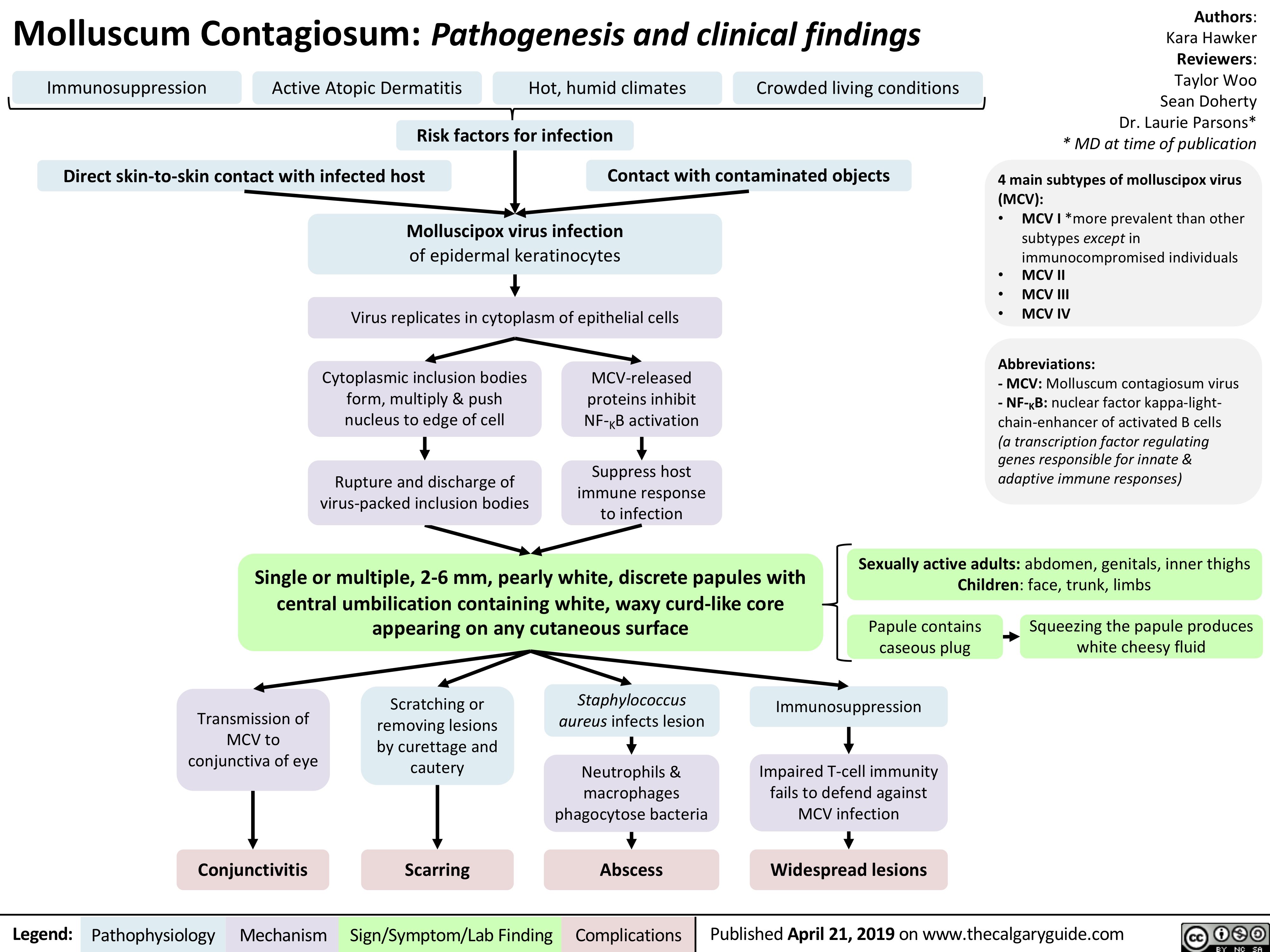
Immunosuppression
Active Atopic Dermatitis Hot, humid climates Crowded living conditions
Risk factors for infection
Direct skin-to-skin contact with infected host Contact with contaminated objects
Molluscipox virus infection
of epidermal keratinocytes
Virus replicates in cytoplasm of epithelial cells
Cytoplasmic inclusion bodies form, multiply & push nucleus to edge of cell
Rupture and discharge of virus-packed inclusion bodies
MCV-released proteins inhibit NF-KB activation
Suppress host immune response to infection
Single or multiple, 2-6 mm, pearly white, discrete papules with central umbilication containing white, waxy curd-like core appearing on any cutaneous surface
Papule contains caseous plug
Squeezing the papule produces white cheesy fluid
Transmission of MCV to conjunctiva of eye
Scratching or removing lesions by curettage and cautery
Staphylococcus aureus infects lesion
Neutrophils & macrophages phagocytose bacteria
Immunosuppression
Impaired T-cell immunity fails to defend against MCV infection
Conjunctivitis
Scarring
Abscess
Widespread lesions
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 21, 2019 on www.thecalgaryguide.com