Content
Collaboration
About Us
Contact Us
Foundations
Pharmacology
Physiology
Population Health
Radiology
Systems
Anesthesia
Cardiology
Clinical Immunology
Dermatology
Endocrinology
Ear/Nose/Throat
Gastroenterology
Geriatrics
Gynecology
Hematology
Infectious Diseases
Nephrology
Neurology
Obstetrics
Ophthalmology
Orthopedics
Pediatrics
Psychiatry
Respirology
Rheumatology
Urology
Other Languages
Arabic (عربي)
Chinese(中文)
French (Français)
German (Deutsch)
Indonesian (bahasa Indonesia)
Italian (Italiano)
Persian (فارسی)
Polish (Polski)
Portuguese (Português)
Russian (Pусский)
Slovene (Slovenščina)
Spanish (Español)
Vietnamese (Việt Nam)
Cardiology
Valvular Disorders
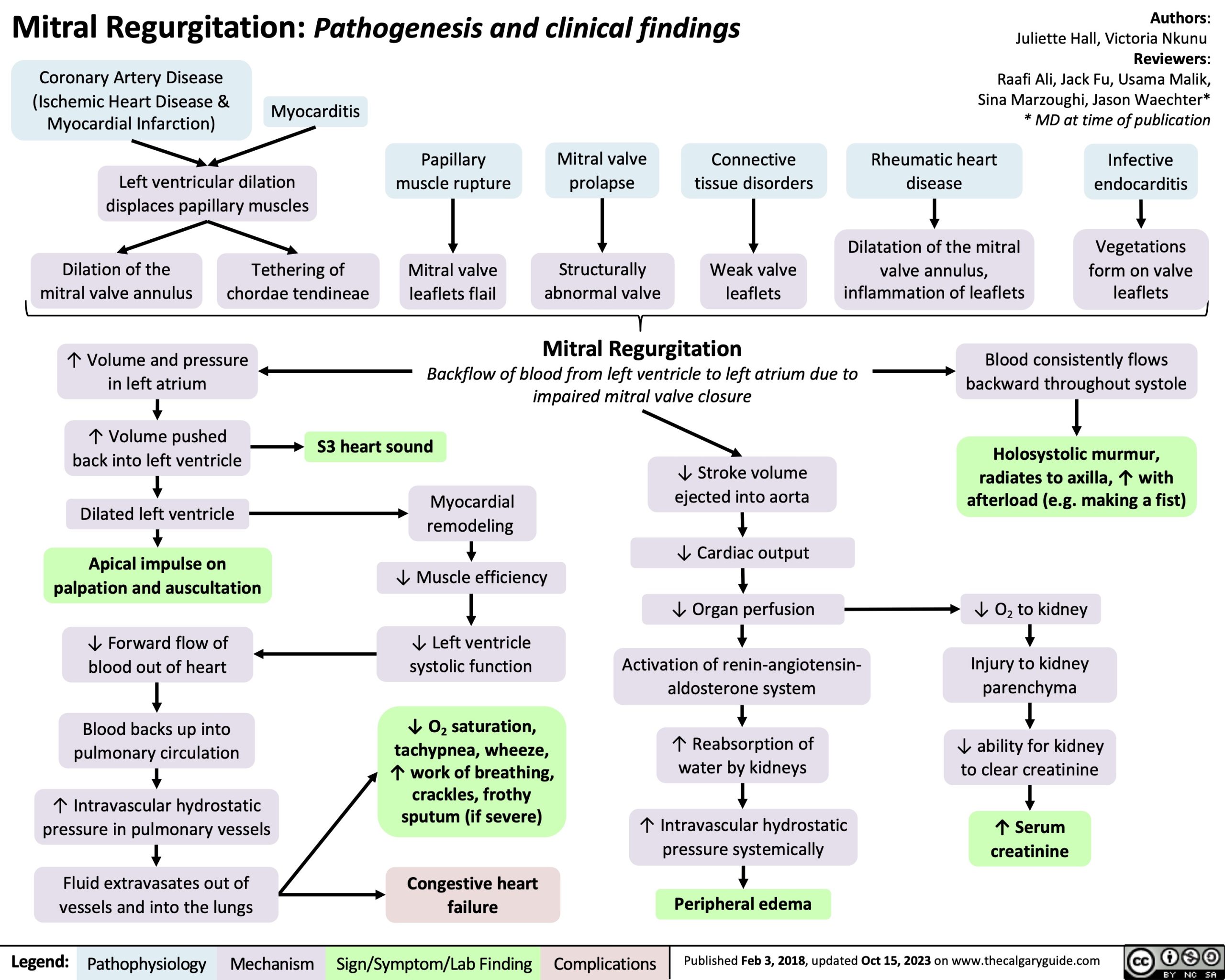
Mitral Regurgitation: Pathogenesis and clinical findings
Mitral Regurgitation: Pathogenesis and clinical findings
Post Views:
48,668
Associated Relevant Slides