Mechanical Ventilation: Mechanisms of Action and Complications
Authors: Madison Amyotte
Reviewers:
Victória Silva, Mao Ding Eric Leung*
* MD at time of publication
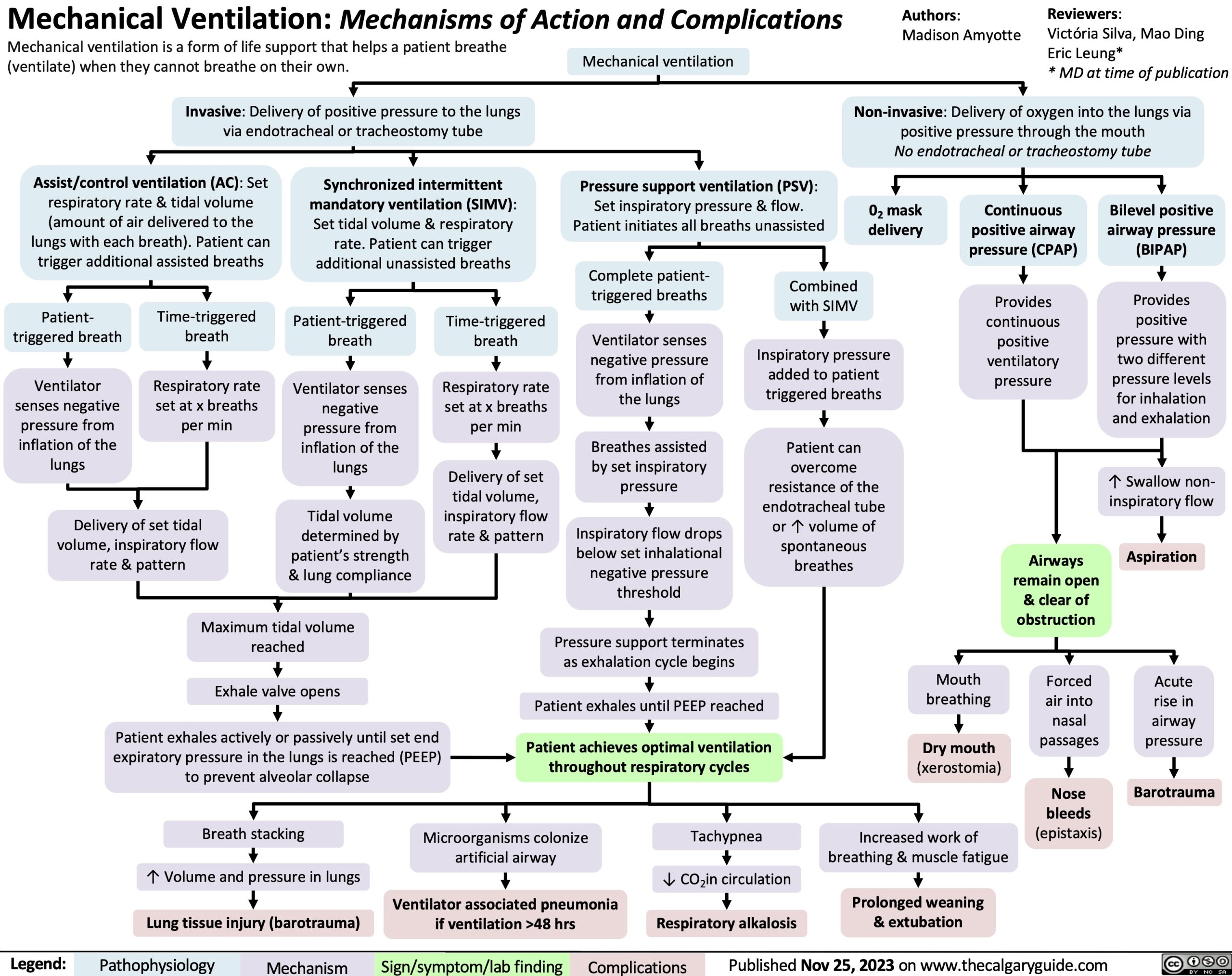
Mechanical ventilation is a form of life support that helps a patient breathe (ventilate) when they cannot breathe on their own.
Invasive: Delivery of positive pressure to the lungs via endotracheal or tracheostomy tube
Mechanical ventilation
Pressure support ventilation (PSV): Set inspiratory pressure & flow. Patient initiates all breaths unassisted
Non-invasive: Delivery of oxygen into the lungs via positive pressure through the mouth
No endotracheal or tracheostomy tube
Assist/control ventilation (AC): Set respiratory rate & tidal volume (amount of air delivered to the lungs with each breath). Patient can trigger additional assisted breaths
Synchronized intermittent mandatory ventilation (SIMV): Set tidal volume & respiratory rate. Patient can trigger additional unassisted breaths
02 mask delivery
Continuous positive airway pressure (CPAP)
Provides continuous positive ventilatory pressure
Bilevel positive airway pressure (BIPAP)
Provides positive pressure with two different pressure levels for inhalation and exhalation
↑ Swallow non- inspiratory flow
Aspiration
Acute rise in airway pressure
Barotrauma
Patient- triggered breath
Ventilator senses negative pressure from inflation of the lungs
Time-triggered breath
Respiratory rate set at x breaths per min
Patient-triggered breath
Ventilator senses negative pressure from inflation of the lungs
Tidal volume determined by patient’s strength & lung compliance
Time-triggered breath
Respiratory rate set at x breaths per min
Delivery of set tidal volume, inspiratory flow rate & pattern
Complete patient- triggered breaths
Ventilator senses negative pressure from inflation of the lungs
Breathes assisted by set inspiratory pressure
Inspiratory flow drops below set inhalational negative pressure threshold
Pressure support terminates as exhalation cycle begins
Combined with SIMV
Inspiratory pressure added to patient triggered breaths
Patient can overcome resistance of the endotracheal tube or ↑ volume of spontaneous breathes
Delivery of set tidal volume, inspiratory flow rate & pattern
Airways remain open & clear of obstruction
Forced air into nasal passages
Nose bleeds (epistaxis)
Maximum tidal volume reached
Exhale valve opens
Patient exhales actively or passively until set end expiratory pressure in the lungs is reached (PEEP) to prevent alveolar collapse
Patient exhales until PEEP reached
Patient achieves optimal ventilation throughout respiratory cycles
Mouth breathing
Dry mouth
(xerostomia)
Increased work of breathing & muscle fatigue
Prolonged weaning & extubation
Breath stacking
↑ Volume and pressure in lungs Lung tissue injury (barotrauma)
Microorganisms colonize artificial airway
Ventilator associated pneumonia if ventilation >48 hrs
Tachypnea
↓ CO2in circulation Respiratory alkalosis
Legend:
Pathophysiology
Mechanism
Sign/symptom/lab finding
Complications
Published Nov 25, 2023 on www.thecalgaryguide.com