Mastoiditis: Pathogenesis and clinical findings
Authors:
Amanda Marchak
Reviewers:
Nicola Adderley Jim Rogers Emily Ryznar Danielle Nelson* * MD at time of publication
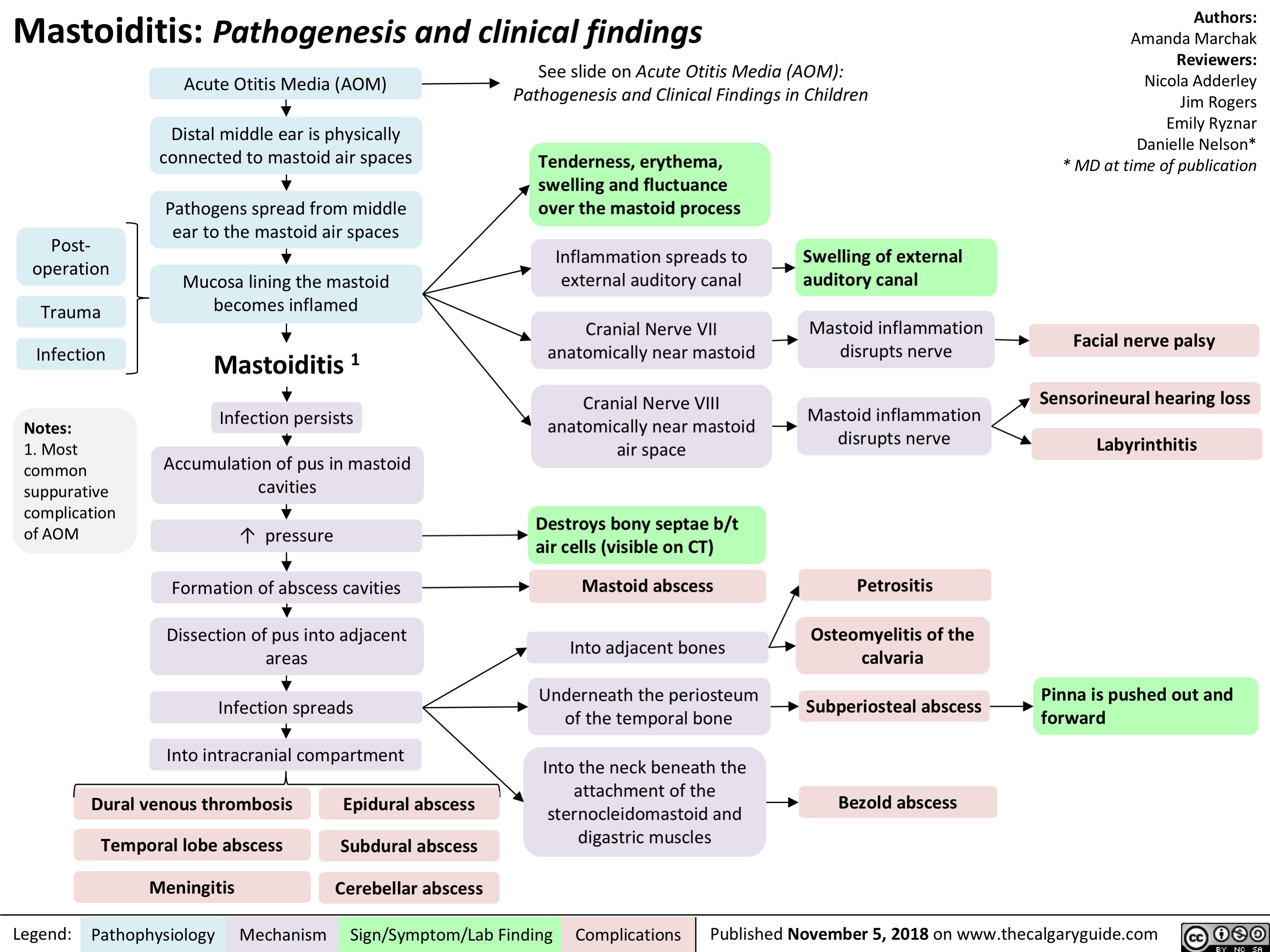
Acute Otitis Media (AOM)
Distal middle ear is physically connected to mastoid air spaces
Pathogens spread from middle ear to the mastoid air spaces
Mucosa lining the mastoid becomes inflamed
Mastoiditis 1
Infection persists
Accumulation of pus in mastoid cavities
↑ pressure Formation of abscess cavities
Dissection of pus into adjacent areas
Infection spreads
Into intracranial compartment
See slide on Acute Otitis Media (AOM): Pathogenesis and Clinical Findings in Children
Post- operation
Trauma Infection
Notes:
1. Most common suppurative complication of AOM
Tenderness, erythema, swelling and fluctuance over the mastoid process
Inflammation spreads to external auditory canal
Cranial Nerve VII anatomically near mastoid
Cranial Nerve VIII anatomically near mastoid air space
Destroys bony septae b/t air cells (visible on CT)
Mastoid abscess
Swelling of external auditory canal
Mastoid inflammation disrupts nerve
Mastoid inflammation disrupts nerve
Petrositis
Facial nerve palsy
Sensorineural hearing loss Labyrinthitis
Osteomyelitis of the calvaria
Into adjacent bones
Underneath the periosteum Subperiosteal abscess Pinna is pushed out and
of the temporal bone
Into the neck beneath the attachment of the sternocleidomastoid and digastric muscles
forward
Dural venous thrombosis Temporal lobe abscess Meningitis
Epidural abscess Subdural abscess Cerebellar abscess
Bezold abscess
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com