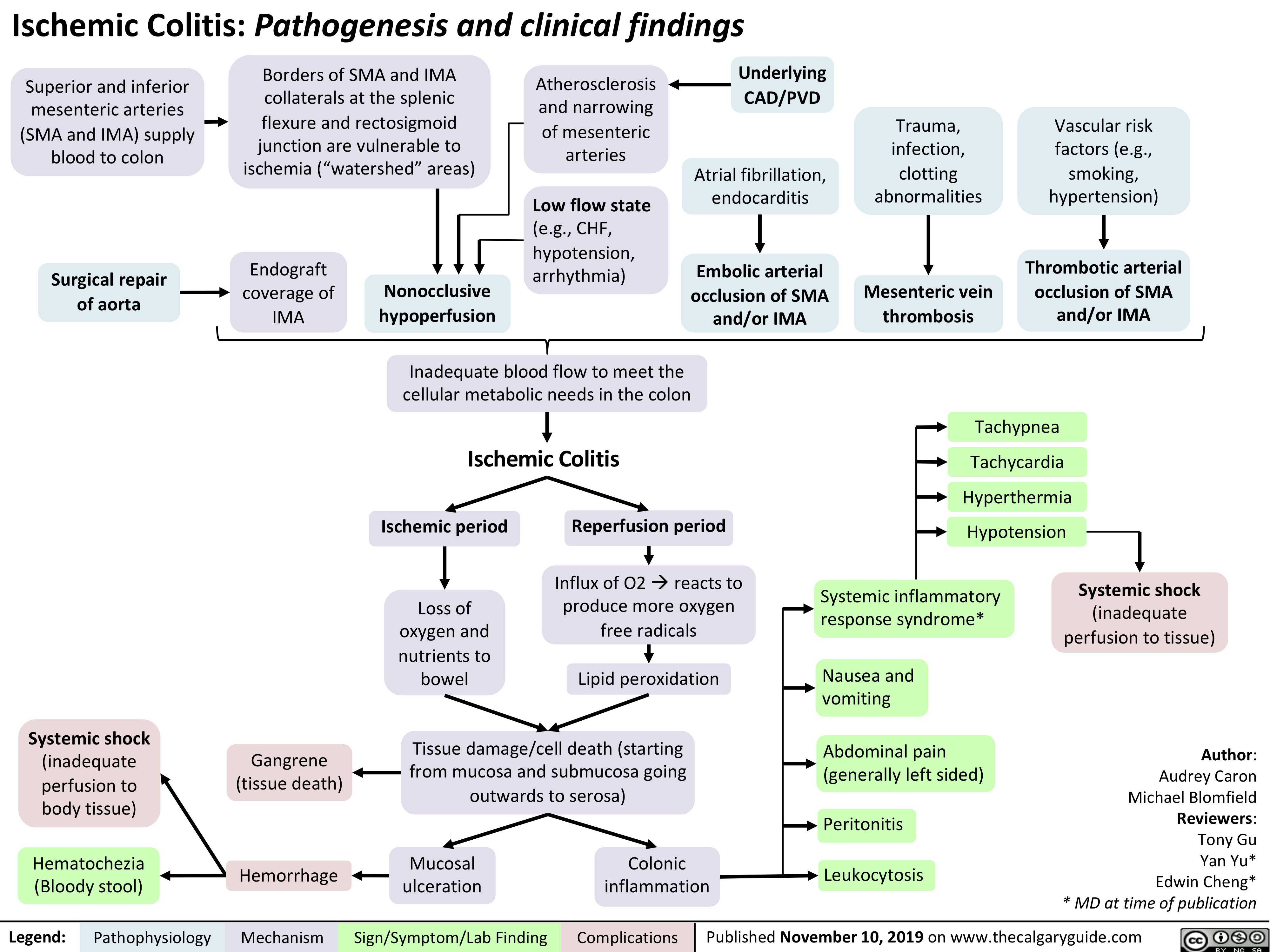
Ischemic Colitis: Pathogenesis and clinical findings
Superior and inferior mesenteric arteries (SMA and IMA) supply blood to colon
Surgical repair of aorta
Borders of SMA and IMA collaterals at the splenic flexure and rectosigmoid junction are vulnerable to ischemia (“watershed” areas)
Atherosclerosis and narrowing of mesenteric arteries
Low flow state
(e.g., CHF, hypotension, arrhythmia)
Underlying CAD/PVD
Atrial fibrillation, endocarditis
Embolic arterial occlusion of SMA and/or IMA
Trauma, infection, clotting abnormalities
Mesenteric vein thrombosis
Vascular risk factors (e.g., smoking, hypertension)
Thrombotic arterial occlusion of SMA and/or IMA
Endograft coverage of IMA
Nonocclusive hypoperfusion
Inadequate blood flow to meet the cellular metabolic needs in the colon
Ischemic Colitis
Tachypnea Tachycardia Hyperthermia Hypotension
Ischemic period
Loss of oxygen and nutrients to bowel
Reperfusion period
Influx of O2àreacts to produce more oxygen free radicals
Lipid peroxidation
Systemic inflammatory response syndrome*
Nausea and vomiting
Abdominal pain (generally left sided)
Peritonitis
Leukocytosis
Systemic shock
(inadequate perfusion to tissue)
Author: Audrey Caron Michael Blomfield Reviewers: Tony Gu Yan Yu* Edwin Cheng* * MD at time of publication
Systemic shock
(inadequate perfusion to body tissue)
Hematochezia (Bloody stool)
Gangrene (tissue death)
Hemorrhage
Tissue damage/cell death (starting from mucosa and submucosa going outwards to serosa)
Mucosal ulceration
Colonic inflammation
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 10, 2019 on www.thecalgaryguide.com