Yu, Yan – Hyperkalemia clinical findings – Published.pptx
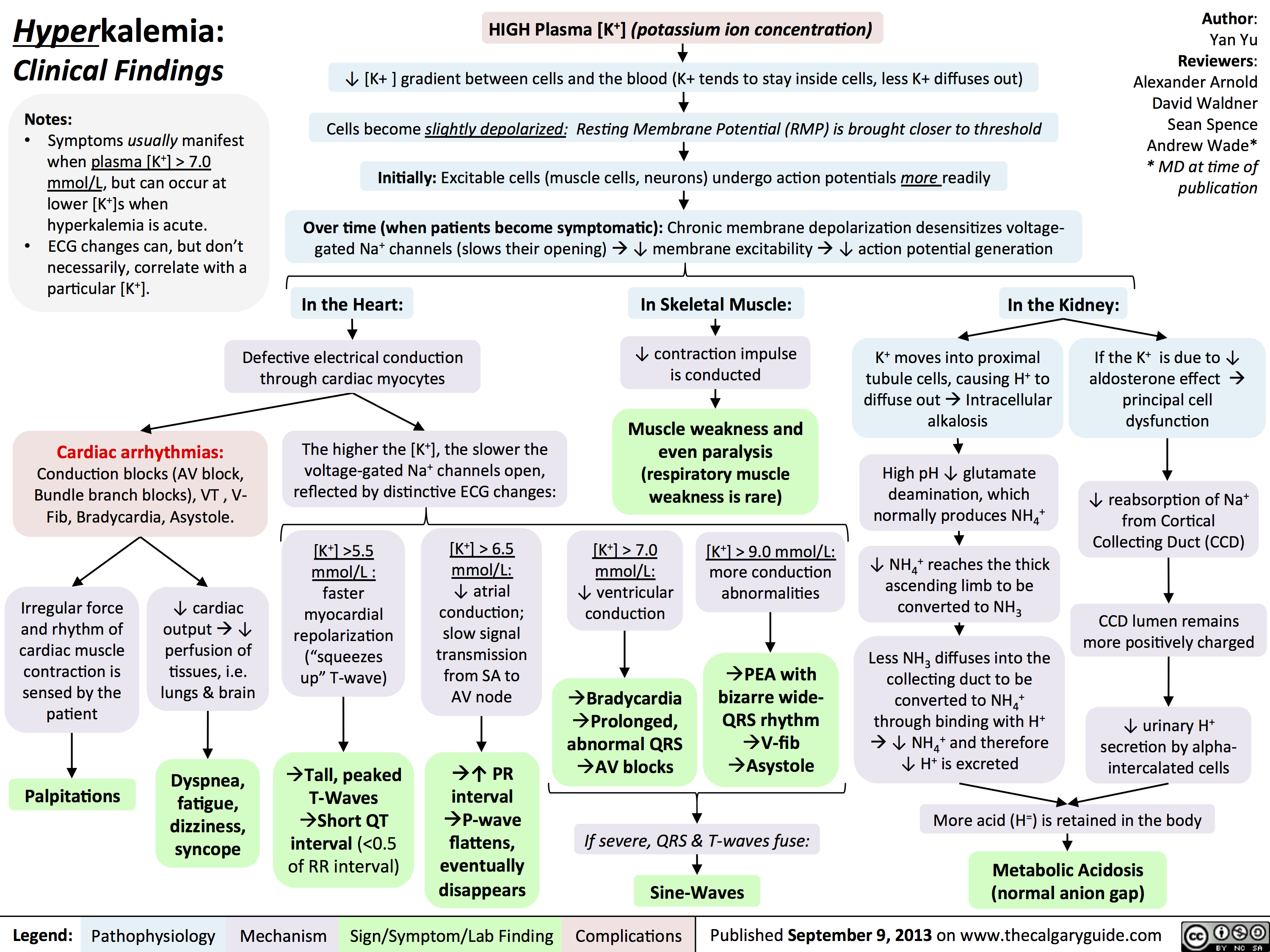
Hyperkalemia: Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published September 9, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsNotes: Symptoms usually manifest when plasma [K+] > 7.0 mmol/L, but can occur at lower [K+]s when hyperkalemia is acute.ECG changes can, but don’t necessarily, correlate with a particular [K+].Initially: Excitable cells (muscle cells, neurons) undergo action potentials more readily? [K+ ] gradient between cells and the blood (K+ tends to stay inside cells, less K+ diffuses out)In the Heart:In Skeletal Muscle:[K+] >5.5 mmol/L :faster myocardial repolarization(“squeezes up” T-wave)Tall, peaked T-Waves Short QT interval (<0.5 of RR interval)[K+] > 6.5 mmol/L:? atrial conduction; slow signal transmission from SA to AV nodeCells become slightly depolarized: Resting Membrane Potential (RMP) is brought closer to thresholdIn the Kidney:Muscle weakness and even paralysis (respiratory muscle weakness is rare)? reabsorption of Na+ from Cortical Collecting Duct (CCD)CCD lumen remains more positively chargedMetabolic Acidosis(normal anion gap)Over time (when patients become symptomatic): Chronic membrane depolarization desensitizes voltage-gated Na+ channels (slows their opening) ? ? membrane excitability ? ? action potential generation[K+] > 7.0 mmol/L:? ventricular conductionBradycardiaProlonged, abnormal QRSAV blocks[K+] > 9.0 mmol/L:more conduction abnormalitiesPEA with bizarre wide-QRS rhythmV-fibAsystole? urinary H+ secretion by alpha-intercalated cellsHIGH Plasma [K+] (potassium ion concentration)Dyspnea, fatigue, dizziness, syncope? cardiac output ? ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: Conduction blocks (AV block, Bundle branch blocks), VT , V-Fib, Bradycardia, Asystole.?? PR interval ?P-wave flattens, eventually disappearsIf severe, QRS & T-waves fuse:Sine-WavesThe higher the [K+], the slower the voltage-gated Na+ channels open, reflected by distinctive ECG changes:If the K+ is due to ? aldosterone effect ? principal cell dysfunctionHigh pH ? glutamate deamination, which normally produces NH4+? NH4+ reaches the thick ascending limb to be converted to NH3Less NH3 diffuses into the collecting duct to be converted to NH4+ through binding with H+ ? ? NH4+ and therefore ? H+ is excretedK+ moves into proximal tubule cells, causing H+ to diffuse out ? Intracellular alkalosis Irregular force and rhythm of cardiac muscle contraction is sensed by the patient? contraction impulse is conductedDefective electrical conduction through cardiac myocytesMore acid (H=) is retained in the body
118 kB / 357 words