Hypercortisolemia (Cushing’s Syndrome): Clinical Findings
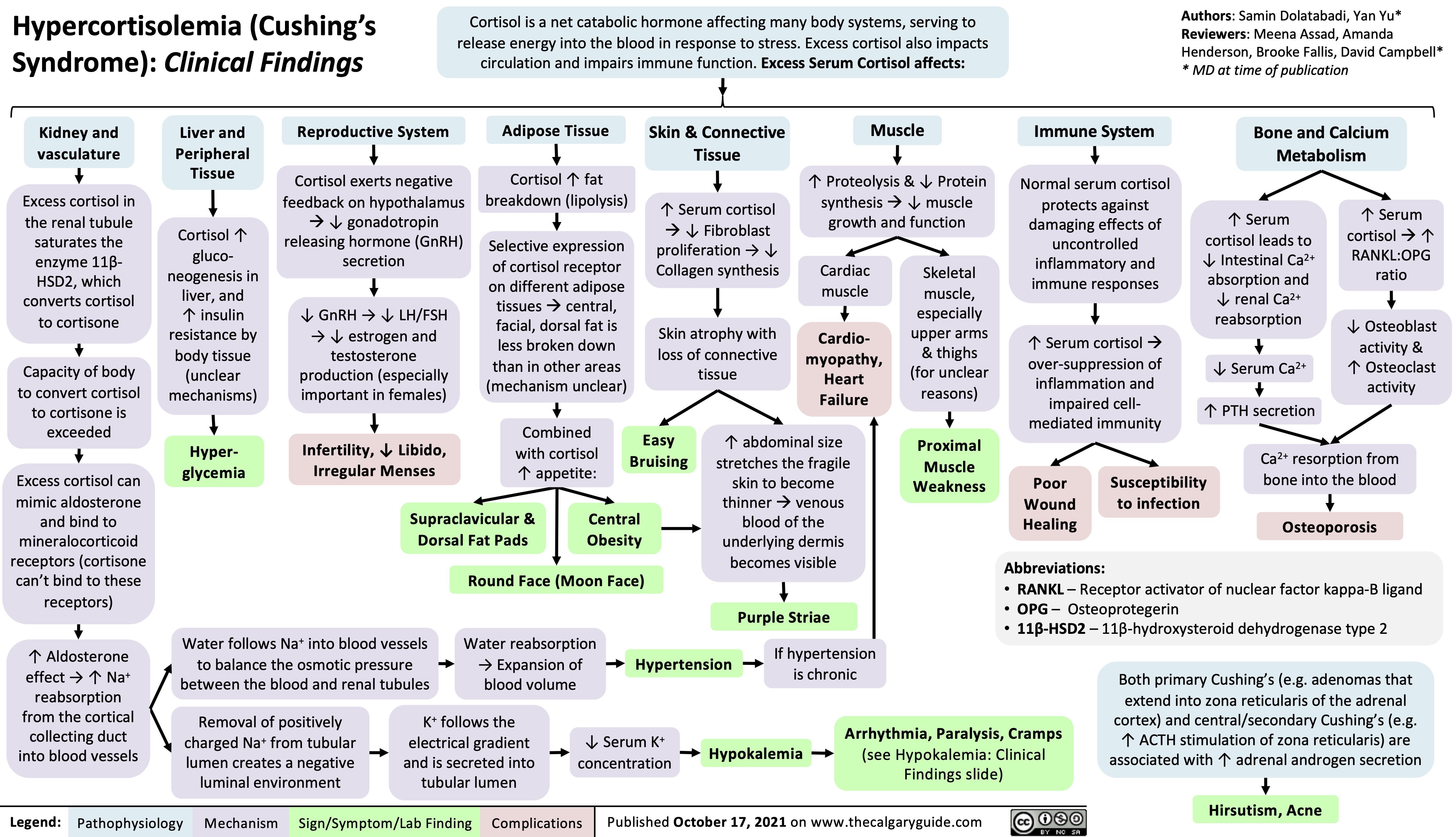
Cortisol is a net catabolic hormone affecting many body systems, serving to release energy into the blood in response to stress. Excess cortisol also impacts circulation and impairs immune function. Excess Serum Cortisol affects:
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Amanda Henderson, Brooke Fallis, David Campbell* * MD at time of publication
Bone and Calcium Metabolism
Kidney and vasculature
Excess cortisol in the renal tubule saturates the enzyme 11β- HSD2, which converts cortisol to cortisone
Capacity of body to convert cortisol to cortisone is exceeded
Excess cortisol can mimic aldosterone
and bind to mineralocorticoid receptors (cortisone can’t bind to these receptors)
↑ Aldosterone effect → ↑ Na+ reabsorption from the cortical collecting duct into blood vessels
Liver and Peripheral Tissue
Cortisol ↑ gluco- neogenesis in liver, and ↑ insulin resistance by body tissue (unclear mechanisms)
Hyper- glycemia
Reproductive System
Cortisol exerts negative feedback on hypothalamus
à↓ gonadotropin releasing hormone (GnRH) secretion
↓ GnRH → ↓ LH/FSH → ↓ estrogen and testosterone production (especially important in females)
Infertility, ↓ Libido, Irregular Menses
Adipose Tissue
Cortisol ↑ fat breakdown (lipolysis)
Selective expression of cortisol receptor on different adipose tissuesàcentral, facial, dorsal fat is less broken down than in other areas (mechanism unclear)
Combined with cortisol ↑ appetite:
Skin & Connective Tissue
↑ Serum cortisol à↓ Fibroblast proliferation → ↓ Collagen synthesis
Skin atrophy with loss of connective tissue
Muscle
↑ Proteolysis & ↓ Protein synthesisà↓ muscle growth and function
Immune System
Normal serum cortisol protects against damaging effects of uncontrolled inflammatory and immune responses
↑ Serum cortisolà over-suppression of inflammation and impaired cell- mediated immunity
↑ Serum cortisol leads to ↓ Intestinal Ca2+ absorption and ↓ renal Ca2+ reabsorption
↓ Serum Ca2+ ↑ PTH secretion
↑ Serum cortisolà↑ RANKL:OPG ratio
↓ Osteoblast activity & ↑ Osteoclast activity
Cardiac muscle
Cardio- myopathy, Heart Failure
Skeletal
muscle, especially upper arms & thighs (for unclear reasons)
Proximal Muscle Weakness
Easy Bruising
↑ abdominal size stretches the fragile skin to become thinneràvenous blood of the underlying dermis becomes visible
Purple Striae
If hypertension is chronic
Ca2+ resorption from bone into the blood
Osteoporosis
Supraclavicular & Dorsal Fat Pads
Central Obesity
Poor Wound Healing
Susceptibility to infection
Round Face (Moon Face)
Abbreviations:
• RANKL – Receptor activator of nuclear factor kappa-Β ligand • OPG – Osteoprotegerin
• 11β-HSD2 – 11β-hydroxysteroid dehydrogenase type 2
Water follows Na+ into blood vessels to balance the osmotic pressure between the blood and renal tubules
Water reabsorption → Expansion of blood volume
Hypertension
Both primary Cushing’s (e.g. adenomas that extend into zona reticularis of the adrenal cortex) and central/secondary Cushing’s (e.g. ↑ ACTH stimulation of zona reticularis) are associated with ↑ adrenal androgen secretion
Removal of positively charged Na+ from tubular lumen creates a negative luminal environment
K+ follows the electrical gradient and is secreted into tubular lumen
↓ Serum K+ concentration
Hypokalemia
Arrhythmia, Paralysis, Cramps
(see Hypokalemia: Clinical Findings slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 17, 2021 on www.thecalgaryguide.com
Hirsutism, Acne