Hemophilia:
Pathogenesis and clinical findings
Authors: Sean Spence Reviewers: Jennifer Au Yan Yu Erin Stephenson Lynn Savoie* * Indicates faculty member at time of publication
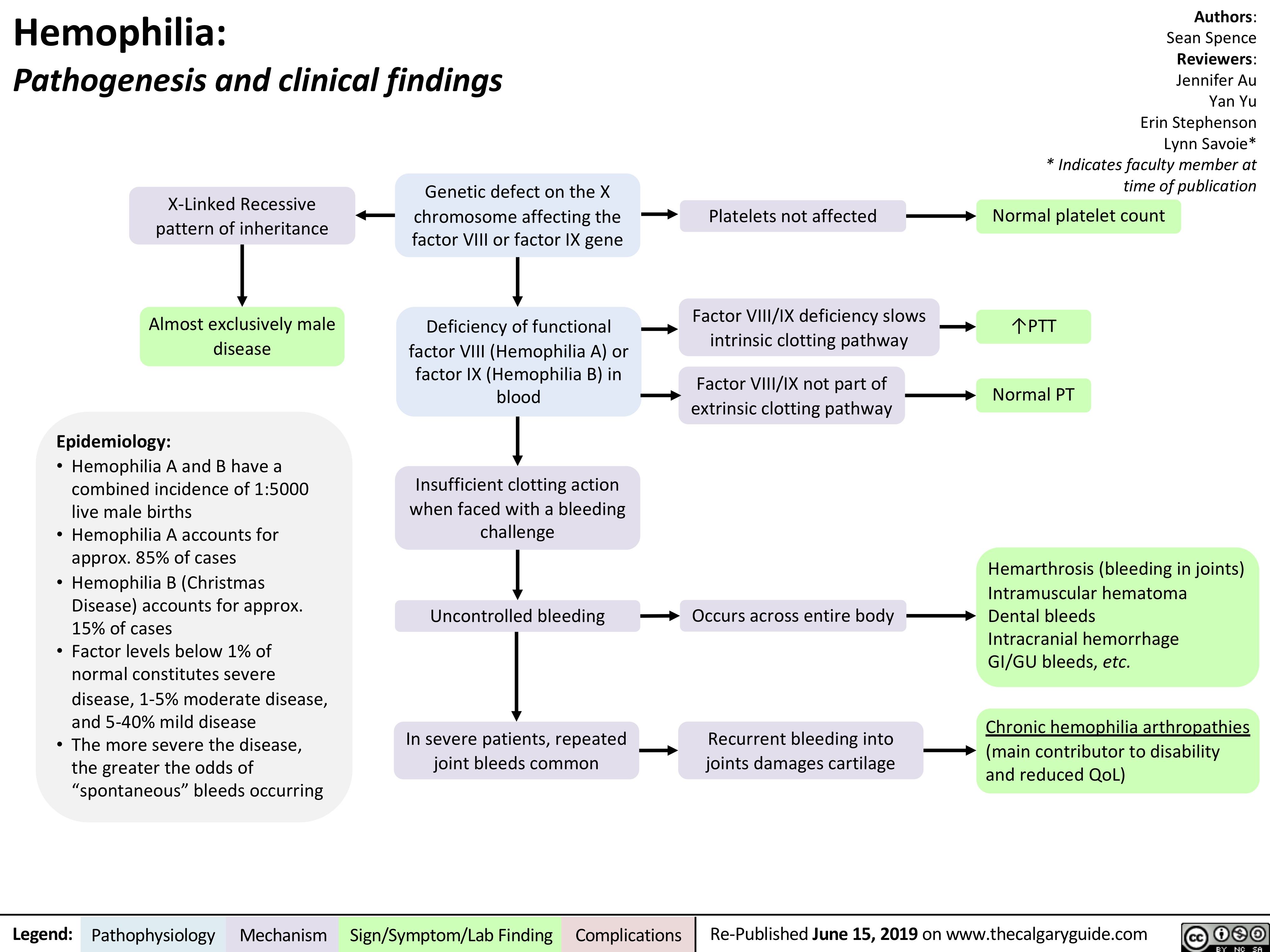
Platelets not affected Normal platelet count
X-Linked Recessive pattern of inheritance
Almost exclusively male disease
Epidemiology:
• Hemophilia A and B have a combined incidence of 1:5000 live male births
• Hemophilia A accounts for approx. 85% of cases
• Hemophilia B (Christmas Disease) accounts for approx. 15% of cases
• Factor levels below 1% of normal constitutes severe disease, 1-5% moderate disease, and 5-40% mild disease
• The more severe the disease, the greater the odds of “spontaneous” bleeds occurring
Genetic defect on the X chromosome affecting the factor VIII or factor IX gene
Deficiency of functional factor VIII (Hemophilia A) or factor IX (Hemophilia B) in blood
Insufficient clotting action when faced with a bleeding challenge
Factor VIII/IX deficiency slows intrinsic clotting pathway
Factor VIII/IX not part of extrinsic clotting pathway
↑PTT Normal PT
Uncontrolled bleeding Occurs across entire body
Hemarthrosis (bleeding in joints) Intramuscular hematoma
Dental bleeds
Intracranial hemorrhage
GI/GU bleeds, etc.
Chronic hemophilia arthropathies
(main contributor to disability and reduced QoL)
In severe patients, repeated joint bleeds common
Recurrent bleeding into joints damages cartilage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com