Guillain-Barré Syndrome: Pathogenesis and clinical findings
Author: Nissi Wei Mao Ding Reviewers: Owen Stechishin Matthew Harding Cory Toth* * MD at time of publication
↑ Protein in cerebrospinal fluid (CSF)
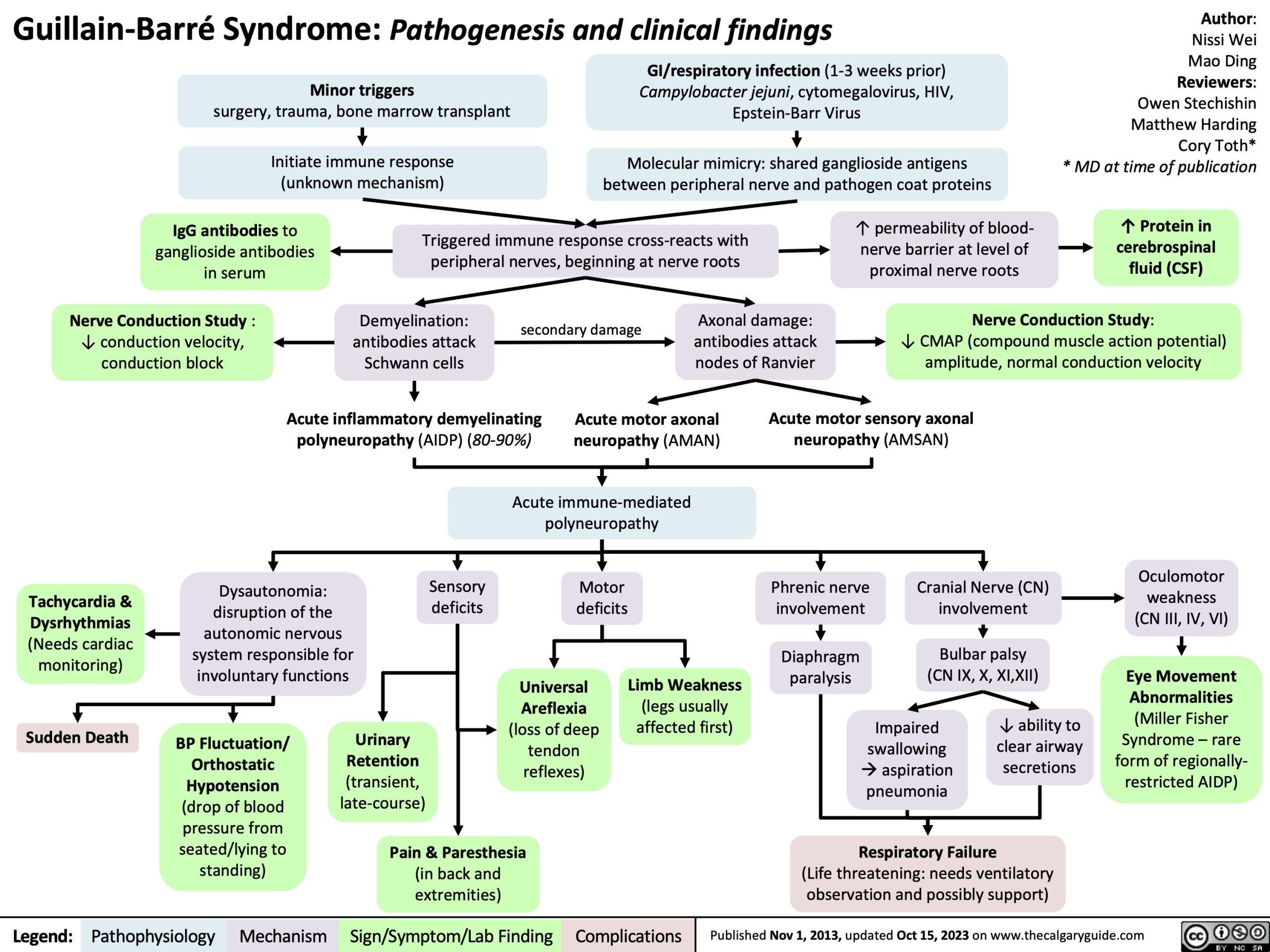
Minor triggers
surgery, trauma, bone marrow transplant
Initiate immune response (unknown mechanism)
GI/respiratory infection (1-3 weeks prior) Campylobacter jejuni, cytomegalovirus, HIV, Epstein-Barr Virus
Molecular mimicry: shared ganglioside antigens between peripheral nerve and pathogen coat proteins
IgG antibodies to ganglioside antibodies in serum
Nerve Conduction Study : ↓ conduction velocity, conduction block
Triggered immune response cross-reacts with peripheral nerves, beginning at nerve roots
↑ permeability of blood- nerve barrier at level of proximal nerve roots
Demyelination: antibodies attack Schwann cells
secondary damage
Axonal damage: antibodies attack nodes of Ranvier
Nerve Conduction Study:
↓ CMAP (compound muscle action potential) amplitude, normal conduction velocity
Acute inflammatory demyelinating polyneuropathy (AIDP) (80-90%)
Acute motor axonal neuropathy (AMAN)
Acute motor sensory axonal neuropathy (AMSAN)
Acute immune-mediated polyneuropathy
Tachycardia & Dysrhythmias (Needs cardiac monitoring)
Sudden Death
Dysautonomia: disruption of the autonomic nervous system responsible for involuntary functions
Sensory deficits
Motor deficits
Universal Areflexia (loss of deep tendon reflexes)
Phrenic nerve involvement
Diaphragm paralysis
Cranial Nerve (CN) involvement
Bulbar palsy (CN IX, X, XI,XII)
Oculomotor weakness (CN III, IV, VI)
Eye Movement Abnormalities (Miller Fisher Syndrome – rare form of regionally- restricted AIDP)
BP Fluctuation/ Orthostatic Hypotension (drop of blood pressure from seated/lying to standing)
Urinary Retention (transient, late-course)
Limb Weakness
(legs usually affected first)
Impaired swallowing àaspiration pneumonia
↓ ability to clear airway secretions
Pain & Paresthesia
(in back and extremities)
Respiratory Failure
(Life threatening: needs ventilatory observation and possibly support)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 1, 2013, updated Oct 15, 2023 on www.thecalgaryguide.com
Guillain-Barré Syndrome
Minor triggers (surgery, trauma,
GI/respiratory infection
Campylobacter jejuni, CMV, HIV , EBV
(1-3 weeks prior)
Molecular mimicry: shared ganglioside antigens between peripheral nerve and pathogen coat proteins
Author: Nissi Wei Reviewers: Owen Stechishin Matthew Harding Cory Toth* * MD at time of publication
↑ Protein in CSF
bone marrow transplant)
Initiate immune response (unknown mechanism)
IgG antibodies to ganglioside antibodies in serum
NCS: ↓ conduction velocity, conduction block
Triggered immune response cross-reacts with peripheral nerves, beginning at nerve roots
↑ permeability of blood- nerve barrier at level of proximal nerve roots
NCS: ↓ CMAP amplitude, normal conduction velocity
Demyelination: antibodies attack Schwann cells
secondary damage
Axonal damage:
antibodies attack nodes of Ranvier
Acute inflammatory demyelinating polyneuropathy (AIDP) (80-90%)
Acute motor axonal neuropathy (AMAN)
Cranial nerve involvement
Dysautonomia
Acute motor sensory axonal neuropathy (AMSAN)
Eye Movement Abnormalities
(Miller Fisher Syndrome – rare form of regionally-restricted AIDP)
Acute immune-mediated polyneuropathy
Oculomotor weakness (CN III, IV, VI)
Bulbar palsy (CN IX, X, XI,XII)
Phrenic nerve involvement
↓ ability to clear airway secretions
Impaired swallowingà aspiration pneumonia
Diaphragm paralysis
Respiratory Failure
(Life threatening: needs ventilatory observation and possibly support)
Motor deficits
Sensory deficits
Pain & Paresthesias in back and extremities
Limb Weakness
(legs usually affected first)
Universal Areflexia
Urinary Retention
(transient, late-course)
Sudden Death
BP Fluctuation, Orthostatic Hypotension
Tachycardia, Dysrhythmias (Needs cardiac monitoring)
Abbreviations:
• NCS – nerve conduction
study
• CMAP – compound muscle
action potential
• EBV – Epstein-Barr Virus
• CMV – cytomegalovirus
• CN – cranial nerve
Note: Aα, Aβ peripheral nerve fibres (large, fast-conducting, heavily myelinated axons for muscle stretch, light touch & proprioception) are more affected than Aδ and C fibres (small, less myelinated, slowly-conducting fibres for pain and temperature)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 1, 2013 on www.thecalgaryguide.com