Gout: Pathogenesis of X-Ray findings
Authors: Omer Mansoor, Nameerah Wajahat Reviewers: Reshma Sirajee, Tara Shannon *Stephanie Nguyen, *Shelley Spaner *MD at time of publication
Hyperuricemia
See hyperuricemia slide for mechanism
↑ Uric acid concentration in blood leaks into joints as monosodium urate (MSU) crystals
Uric acid crystallizes due to lower temperature, change in pH, mechanical stress and other synovial factors
Crystals found more commonly in 1st MTP joint > ankle > wrist
MSU deposits within the bone producing
intra-osseus tophi (stone-like deposits of crystals)
MSU deposits in soft tissue and bone
↑ Inflammatory marker recruitment causes granulomatous inflammation
Osteoclasts (↑ bone resorption) are activated, and osteoblasts (↑ bone formation) are inhibited at
site of inflammation Marked localized bone loss
‘Rat Bite’ erosions
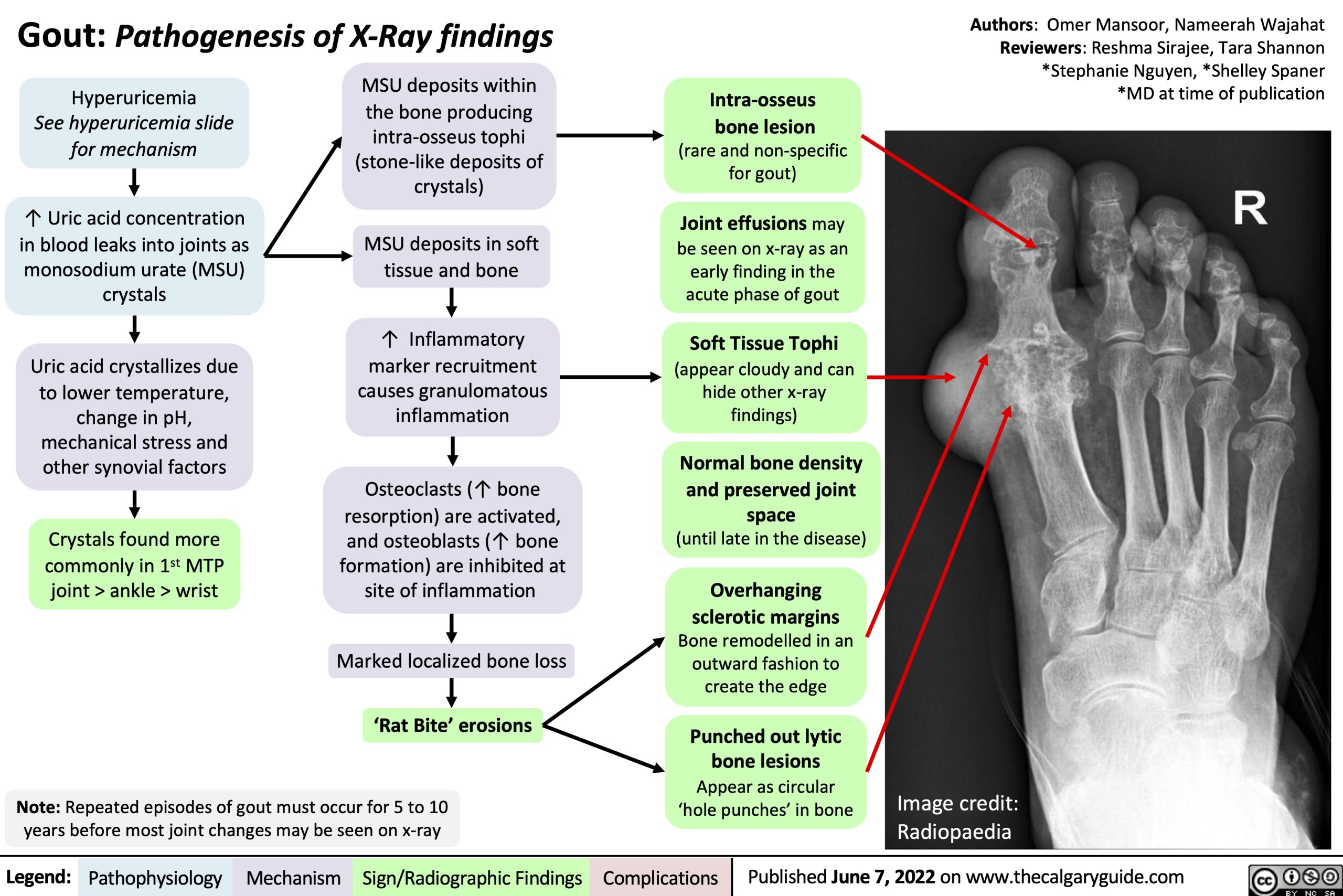
Intra-osseus bone lesion
(rare and non-specific for gout)
Joint effusions may be seen on x-ray as an early finding in the acute phase of gout
Soft Tissue Tophi
(appear cloudy and can hide other x-ray findings)
Normal bone density and preserved joint space
(until late in the disease)
Overhanging
sclerotic margins
Bone remodelled in an outward fashion to create the edge
Punched out lytic bone lesions Appear as circular ‘hole punches’ in bone
Note: Repeated episodes of gout must occur for 5 to 10 years before most joint changes may be seen on x-ray
Image credit: Radiopaedia
Legend:
Pathophysiology
Mechanism
Sign/Radiographic Findings
Complications
Published June 7, 2022 on www.thecalgaryguide.com