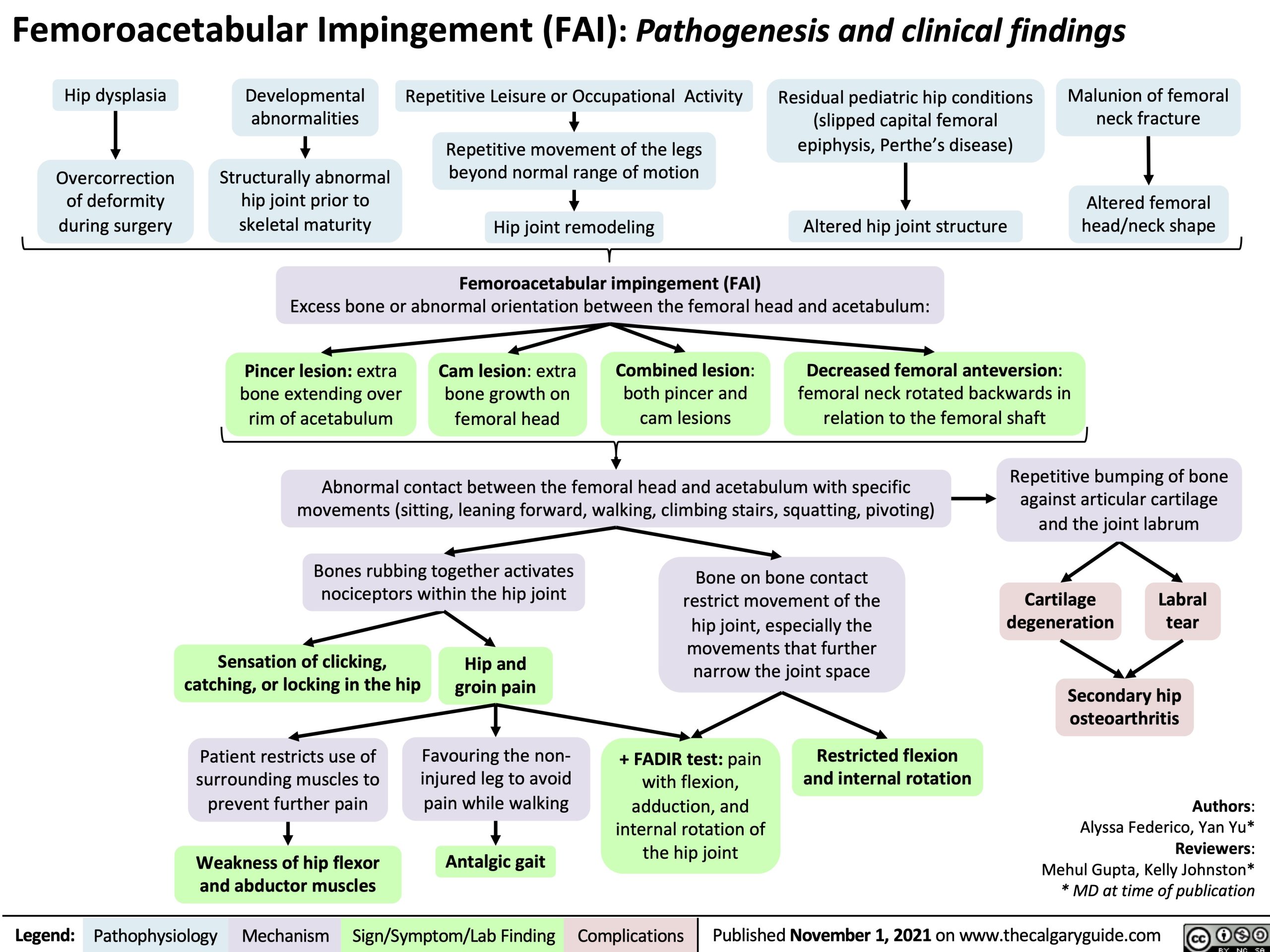
Femoroacetabular Impingement (FAI): Pathogenesis and clinical findings
Hip dysplasia
Overcorrection of deformity during surgery
Developmental abnormalities
Malunion of femoral neck fracture
Altered femoral head/neck shape
Repetitive Leisure or Occupational Activity
Repetitive movement of the legs beyond normal range of motion
Altered hip joint structure Excess bone or abnormal orientation between the femoral head and acetabulum:
Residual pediatric hip conditions (slipped capital femoral epiphysis, Perthe’s disease)
Structurally abnormal hip joint prior to skeletal maturity
Hip joint remodeling
Femoroacetabular impingement (FAI)
Pincer lesion: extra bone extending over rim of acetabulum
Cam lesion: extra bone growth on femoral head
Combined lesion: both pincer and cam lesions
Decreased femoral anteversion: femoral neck rotated backwards in relation to the femoral shaft
Abnormal contact between the femoral head and acetabulum with specific movements (sitting, leaning forward, walking, climbing stairs, squatting, pivoting)
Repetitive bumping of bone against articular cartilage and the joint labrum
Bones rubbing together activates nociceptors within the hip joint
Bone on bone contact restrict movement of the hip joint, especially the movements that further narrow the joint space
Cartilage degeneration tear
Secondary hip osteoarthritis
Authors: Alyssa Federico, Yan Yu* Reviewers: Mehul Gupta, Kelly Johnston* * MD at time of publication
Labral
Sensation of clicking, catching, or locking in the hip
Hip and groin pain
Patient restricts use of surrounding muscles to prevent further pain
Weakness of hip flexor and abductor muscles
Favouring the non- injured leg to avoid pain while walking
Antalgic gait
+ FADIR test: pain with flexion, adduction, and internal rotation of the hip joint
Restricted flexion and internal rotation
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 1, 2021 on www.thecalgaryguide.com