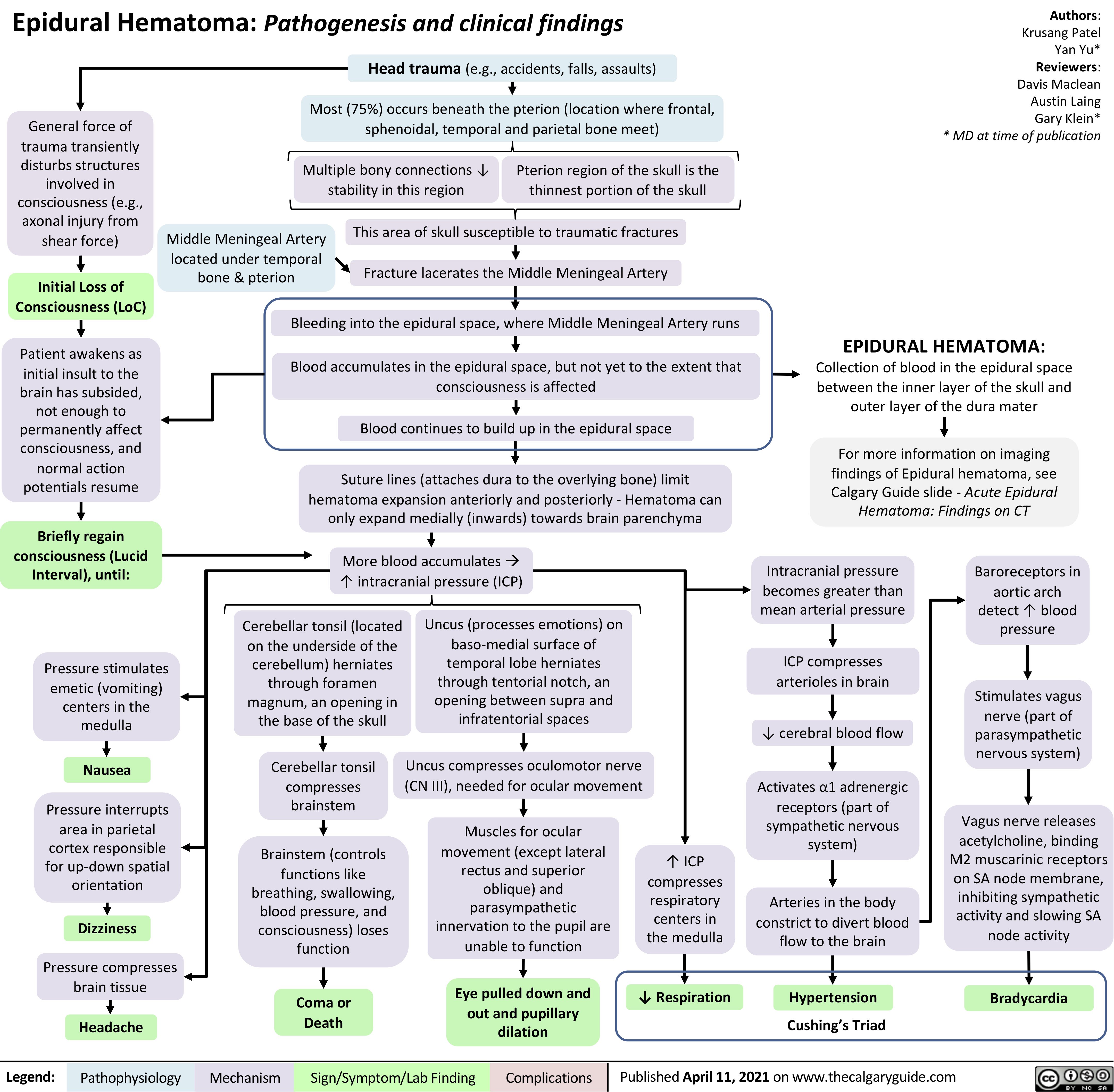
Epidural Hematoma: Pathogenesis and clinical findings Head trauma (e.g., accidents, falls, assaults)
Authors: Krusang Patel Yan Yu* Reviewers: Davis Maclean Austin Laing Gary Klein* * MD at time of publication
General force of trauma transiently disturbs structures involved in consciousness (e.g., axonal injury from shear force)
Initial Loss of Consciousness (LoC)
Patient awakens as initial insult to the
brain has subsided, not enough to permanently affect consciousness, and normal action potentials resume
Briefly regain consciousness (Lucid Interval), until:
Pressure stimulates emetic (vomiting) centers in the medulla
Nausea
Pressure interrupts area in parietal cortex responsible for up-down spatial orientation
Dizziness
Pressure compresses brain tissue
Headache
Most (75%) occurs beneath the pterion (location where frontal, sphenoidal, temporal and parietal bone meet)
Multiple bony connections ↓ stability in this region
Pterion region of the skull is the thinnest portion of the skull
Middle Meningeal Artery located under temporal bone & pterion
This area of skull susceptible to traumatic fractures Fracture lacerates the Middle Meningeal Artery
Bleeding into the epidural space, where Middle Meningeal Artery runs
Blood accumulates in the epidural space, but not yet to the extent that consciousness is affected
Blood continues to build up in the epidural space
Suture lines (attaches dura to the overlying bone) limit hematoma expansion anteriorly and posteriorly – Hematoma can only expand medially (inwards) towards brain parenchyma
More blood accumulatesà ↑ intracranial pressure (ICP)
EPIDURAL HEMATOMA:
Collection of blood in the epidural space between the inner layer of the skull and outer layer of the dura mater
For more information on imaging findings of Epidural hematoma, see Calgary Guide slide – Acute Epidural Hematoma: Findings on CT
Cerebellar tonsil (located on the underside of the cerebellum) herniates through foramen magnum, an opening in the base of the skull
Cerebellar tonsil compresses brainstem
Brainstem (controls functions like breathing, swallowing, blood pressure, and consciousness) loses function
Coma or Death
Uncus (processes emotions) on baso-medial surface of temporal lobe herniates through tentorial notch, an opening between supra and infratentorial spaces
Uncus compresses oculomotor nerve (CN III), needed for ocular movement
Muscles for ocular movement (except lateral
rectus and superior oblique) and parasympathetic innervation to the pupil are unable to function
Eye pulled down and out and pupillary dilation
Intracranial pressure becomes greater than mean arterial pressure
ICP compresses arterioles in brain
↓ cerebral blood flow
Activates α1 adrenergic receptors (part of
sympathetic nervous system)
Arteries in the body constrict to divert blood flow to the brain
Hypertension Cushing’s Triad
Baroreceptors in aortic arch
detect ↑ blood pressure
Stimulates vagus nerve (part of parasympathetic nervous system)
Vagus nerve releases acetylcholine, binding M2 muscarinic receptors on SA node membrane, inhibiting sympathetic activity and slowing SA node activity
Bradycardia
↑ ICP compresses respiratory centers in the medulla
↓ Respiration
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 11, 2021 on www.thecalgaryguide.com