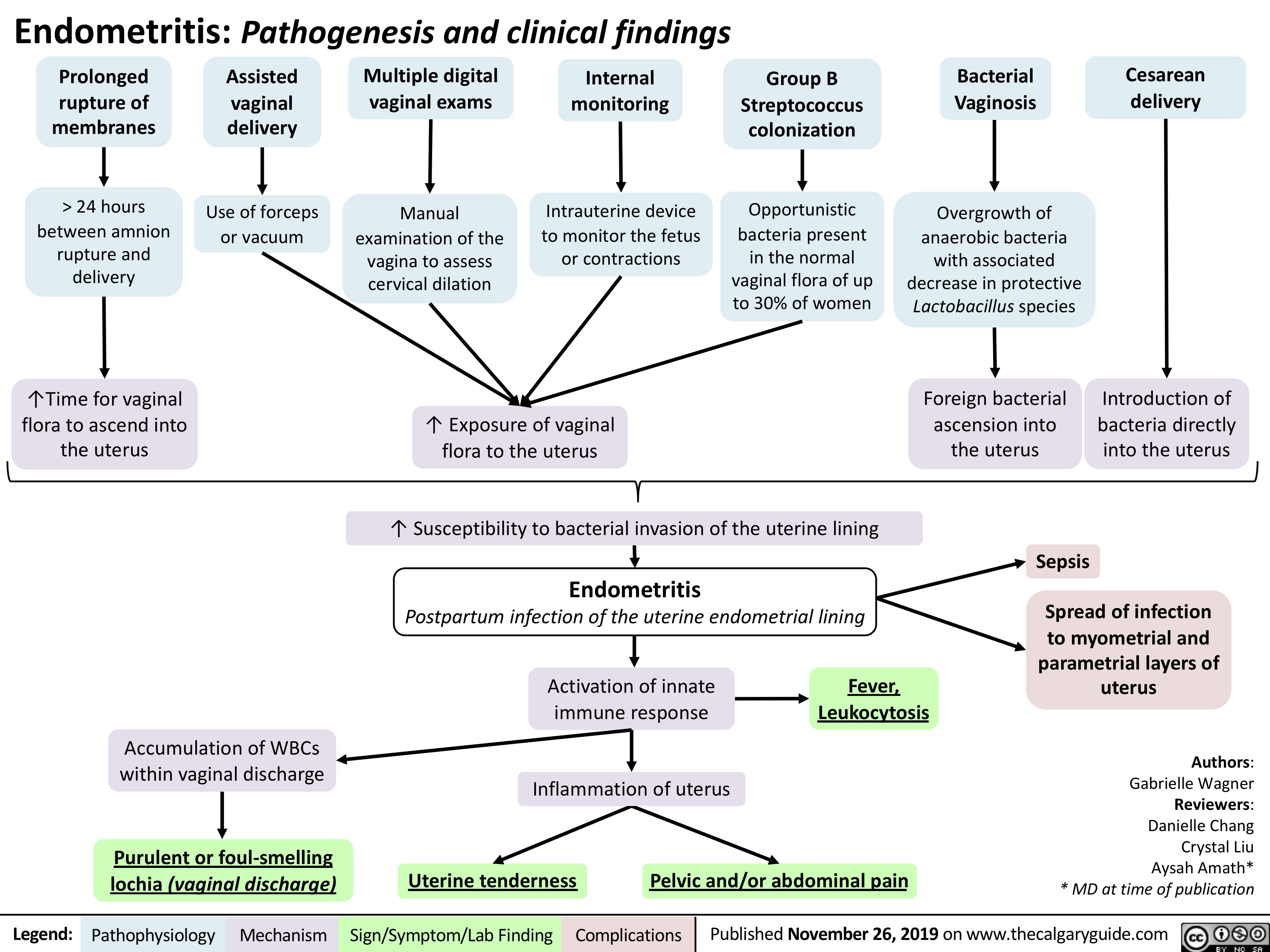
Endometritis: Pathogenesis and clinical findings
Prolonged
rupture of membranes
> 24 hours between amnion
rupture and delivery
↑Time for vaginal flora to ascend into the uterus
Assisted vaginal delivery
Use of forceps or vacuum
Multiple digital vaginal exams
Manual examination of the vagina to assess cervical dilation
Internal monitoring
Intrauterine device to monitor the fetus or contractions
Group B Streptococcus colonization
Opportunistic bacteria present
in the normal vaginal flora of up to 30% of women
Bacterial Vaginosis
Overgrowth of anaerobic bacteria with associated decrease in protective Lactobacillus species
Foreign bacterial ascension into the uterus
Sepsis
Cesarean delivery
↑ Exposure of vaginal flora to the uterus
Introduction of bacteria directly into the uterus
Spread of infection to myometrial and parametrial layers of uterus
Authors: Gabrielle Wagner Reviewers: Danielle Chang Crystal Liu Aysah Amath* * MD at time of publication
↑ Susceptibility to bacterial invasion of the uterine lining
Endometritis
Postpartum infection of the uterine endometrial lining
Activation of innate Fever,
immune response Inflammation of uterus
Leukocytosis
Accumulation of WBCs within vaginal discharge
Purulent or foul-smelling lochia (vaginal discharge)
Uterine tenderness
Pelvic and/or abdominal pain
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com