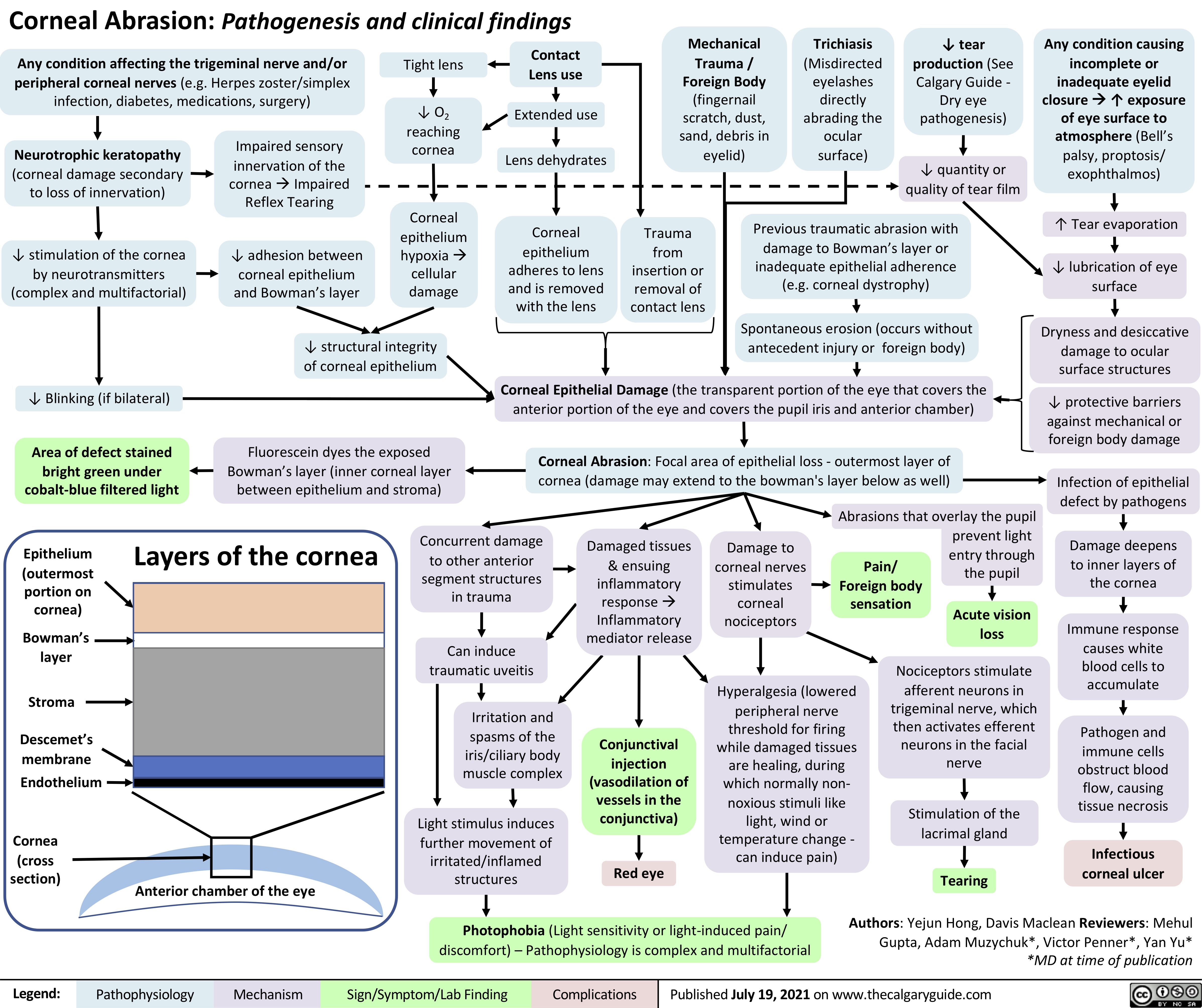
Corneal Abrasion: Pathogenesis and clinical findings
Mechanical Trauma / Foreign Body (fingernail scratch, dust, sand, debris in eyelid)
Trichiasis
(Misdirected eyelashes directly abrading the ocular surface)
↓ tear production (See Calgary Guide – Dry eye pathogenesis)
↓ quantity or quality of tear film
Any condition causing incomplete or inadequate eyelid closureà↑ exposure of eye surface to atmosphere (Bell’s palsy, proptosis/ exophthalmos)
↑ Tear evaporation
↓ lubrication of eye surface
Dryness and desiccative damage to ocular surface structures
↓ protective barriers against mechanical or foreign body damage
Infection of epithelial defect by pathogens
Damage deepens to inner layers of the cornea
Immune response causes white blood cells to accumulate
Pathogen and immune cells obstruct blood flow, causing tissue necrosis
Infectious corneal ulcer
Any condition affecting the trigeminal nerve and/or peripheral corneal nerves (e.g. Herpes zoster/simplex infection, diabetes, medications, surgery)
Tight lens
↓ O2 reaching cornea
Corneal epithelium hypoxiaà cellular damage
Contact Lens use
Extended use Lens dehydrates
Corneal epithelium adheres to lens and is removed with the lens
Neurotrophic keratopathy
(corneal damage secondary to loss of innervation)
↓ stimulation of the cornea by neurotransmitters (complex and multifactorial)
↓ Blinking (if bilateral)
Area of defect stained bright green under cobalt-blue filtered light
Impaired sensory innervation of the
corneaàImpaired Reflex Tearing
↓ adhesion between corneal epithelium and Bowman’s layer
Trauma from insertion or removal of contact lens
Previous traumatic abrasion with damage to Bowman’s layer or inadequate epithelial adherence (e.g. corneal dystrophy)
Spontaneous erosion (occurs without antecedent injury or foreign body)
↓ structural integrity of corneal epithelium
Fluorescein dyes the exposed Bowman’s layer (inner corneal layer between epithelium and stroma)
Corneal Epithelial Damage (the transparent portion of the eye that covers the anterior portion of the eye and covers the pupil iris and anterior chamber)
Corneal Abrasion: Focal area of epithelial loss – outermost layer of cornea (damage may extend to the bowman’s layer below as well)
Abrasions that overlay the pupil
Epithelium (outermost portion on cornea)
Bowman’s layer
Stroma
Descemet’s membrane
Endothelium
Cornea (cross section)
Layers of the cornea
Concurrent damage to other anterior
segment structures in trauma
Can induce traumatic uveitis
Irritation and spasms of the iris/ciliary body muscle complex
Light stimulus induces further movement of
irritated/inflamed structures
Damaged tissues & ensuing inflammatory responseà Inflammatory mediator release
Conjunctival injection (vasodilation of vessels in the conjunctiva)
Red eye
Damage to corneal nerves stimulates corneal nociceptors
Pain/ Foreign body sensation
prevent light entry through the pupil
Acute vision loss
Hyperalgesia (lowered peripheral nerve
threshold for firing while damaged tissues are healing, during which normally non- noxious stimuli like light, wind or temperature change – can induce pain)
Nociceptors stimulate afferent neurons in trigeminal nerve, which then activates efferent neurons in the facial nerve
Stimulation of the lacrimal gland
Tearing
Anterior chamber of the eye
Photophobia (Light sensitivity or light-induced pain/ discomfort) – Pathophysiology is complex and multifactorial
Authors: Yejun Hong, Davis Maclean Reviewers: Mehul Gupta, Adam Muzychuk*, Victor Penner*, Yan Yu* *MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 19, 2021 on www.thecalgaryguide.com