Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Pathogenesis
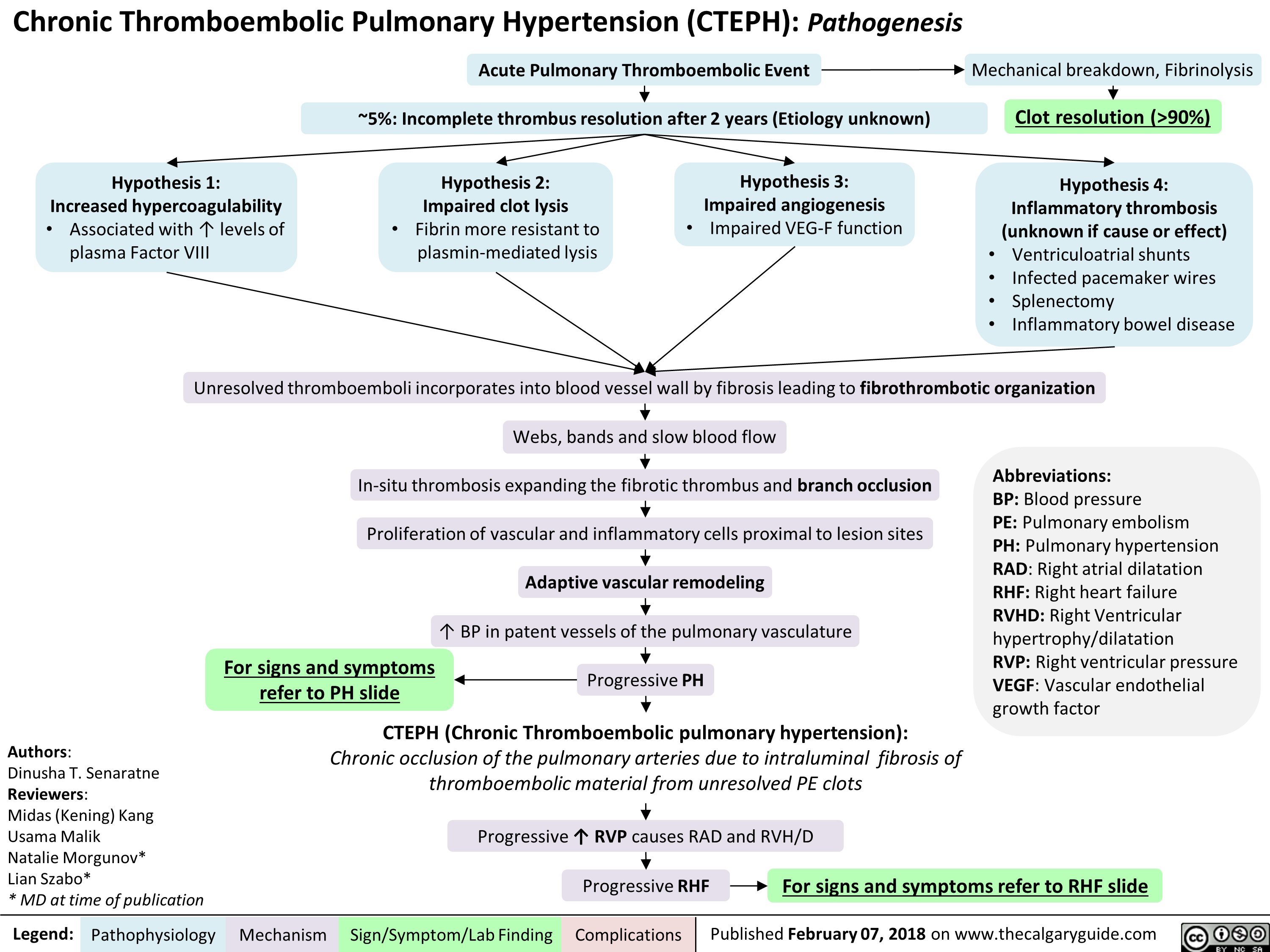
Acute Pulmonary Thromboembolic Event
Mechanical breakdown, Fibrinolysis
—5%: Incomplete thrombus resolution after 2 years (Etiology unknown)
*
Clot resolution (>90%)
Hypothesis 1: Increased hypercoagulability Hypothesis 2: Impaired clot lysis Hypothesis 3: Impaired angiogenesis Hypothesis 4: Inflammatory thrombosis • Associated with 1` levels of • Fibrin more resistant to • Impaired VEG-F function (unknown if cause or effect) plasma Factor VIII plasmin-mediated lysis • Ventriculoatrial shunts • Infected pacemaker wires • Splenectomy • Inflammatory bowel disease
Unresolved thromboemboli incorporates into blood vessel wall by fibrosis leading to fibrothrombotic organization
Authors: Dinusha T. Senaratne Reviewers: Midas (Kening) Kang Usama Malik Natalie Morgunov* Lian Szabo* * MD at time of publication
Legend:
Webs, bands and slow blood flow In-situ thrombosis expanding the fibrotic thrombus and branch occlusion Abbreviations: BP: Blood pressure PE: Pulmonary embolism PH: Pulmonary hypertension RAD: Right atrial dilatation RHF: Right heart failure RVHD: Right Ventricular hypertrophy/dilatation RVP: Right ventricular pressure VEGF: Vascular endothelial growth factor Proliferation of vascular and inflammatory cells proximal to lesion sites Adaptive vascular remodeling BP in patent vessels of the pulmonary vasculature For signs and symptoms refer to PH slide ■ Progressive PH
CTEPH (Chronic Thromboembolic pulmonary hypertension): Chronic occlusion of the pulmonary arteries due to intraluminal fibrosis of thromboembolic material from unresolved PE clots
Pathophysiology Mechanism
Progressive'(` RVP causes RAD and RVH/D
Sign/Symptom/Lab Finding
Progressive RHF
Complications
For signs and symptoms refer to RHF slide