Cholesteatoma (of middle ear): Pathogenesis and clinical findings
Authors: Emma Holmes Angela Mak Reviewers: Stephanie Cote Vaneeza Moosa Shahab Marzoughi William Kim Sunawer Aujla Kristine Anne Smith* * MD at time of publication
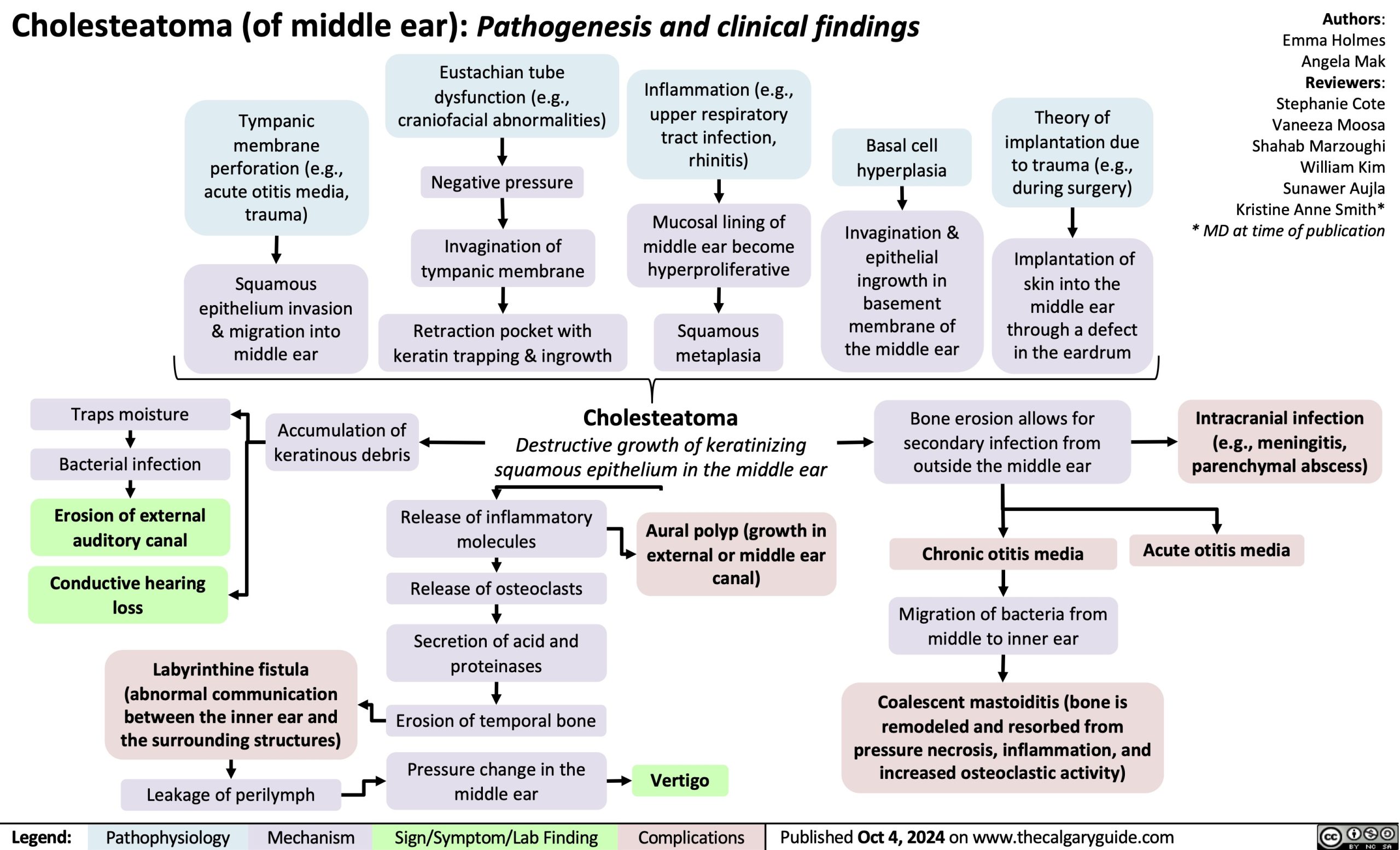
Tympanic membrane perforation (e.g., acute otitis media, trauma)
Squamous epithelium invasion & migration into middle ear
Eustachian tube dysfunction (e.g., craniofacial abnormalities)
Negative pressure
Invagination of tympanic membrane
Retraction pocket with keratin trapping & ingrowth
Inflammation (e.g., upper respiratory tract infection, rhinitis)
Mucosal lining of middle ear become hyperproliferative
Squamous metaplasia
Basal cell hyperplasia
Invagination & epithelial ingrowth in basement membrane of the middle ear
Theory of implantation due to trauma (e.g., during surgery)
Implantation of skin into the
middle ear through a defect in the eardrum
Traps moisture
Bacterial infection
Erosion of external auditory canal
Conductive hearing loss
Labyrinthine fistula (abnormal communication between the inner ear and the surrounding structures)
Leakage of perilymph
Cholesteatoma
Destructive growth of keratinizing squamous epithelium in the middle ear
Bone erosion allows for secondary infection from outside the middle ear
Chronic otitis media
Migration of bacteria from middle to inner ear
Intracranial infection (e.g., meningitis, parenchymal abscess)
Acute otitis media
Accumulation of keratinous debris
Release of inflammatory molecules
Release of osteoclasts
Secretion of acid and proteinases
Erosion of temporal bone
Pressure change in the middle ear
Aural polyp (growth in external or middle ear canal)
Vertigo
Coalescent mastoiditis (bone is remodeled and resorbed from pressure necrosis, inflammation, and increased osteoclastic activity)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com