Carbonic Anhydrase Inhibitor Diuretics: Renal mechanism and side effects
Authors:
Stephanie Happ Reviewers:
Matthew Hobart
Raafi Ali
Adam Bass*
* MD at time of publication
Carbonic Anhydrase Inhibitors (CAI)
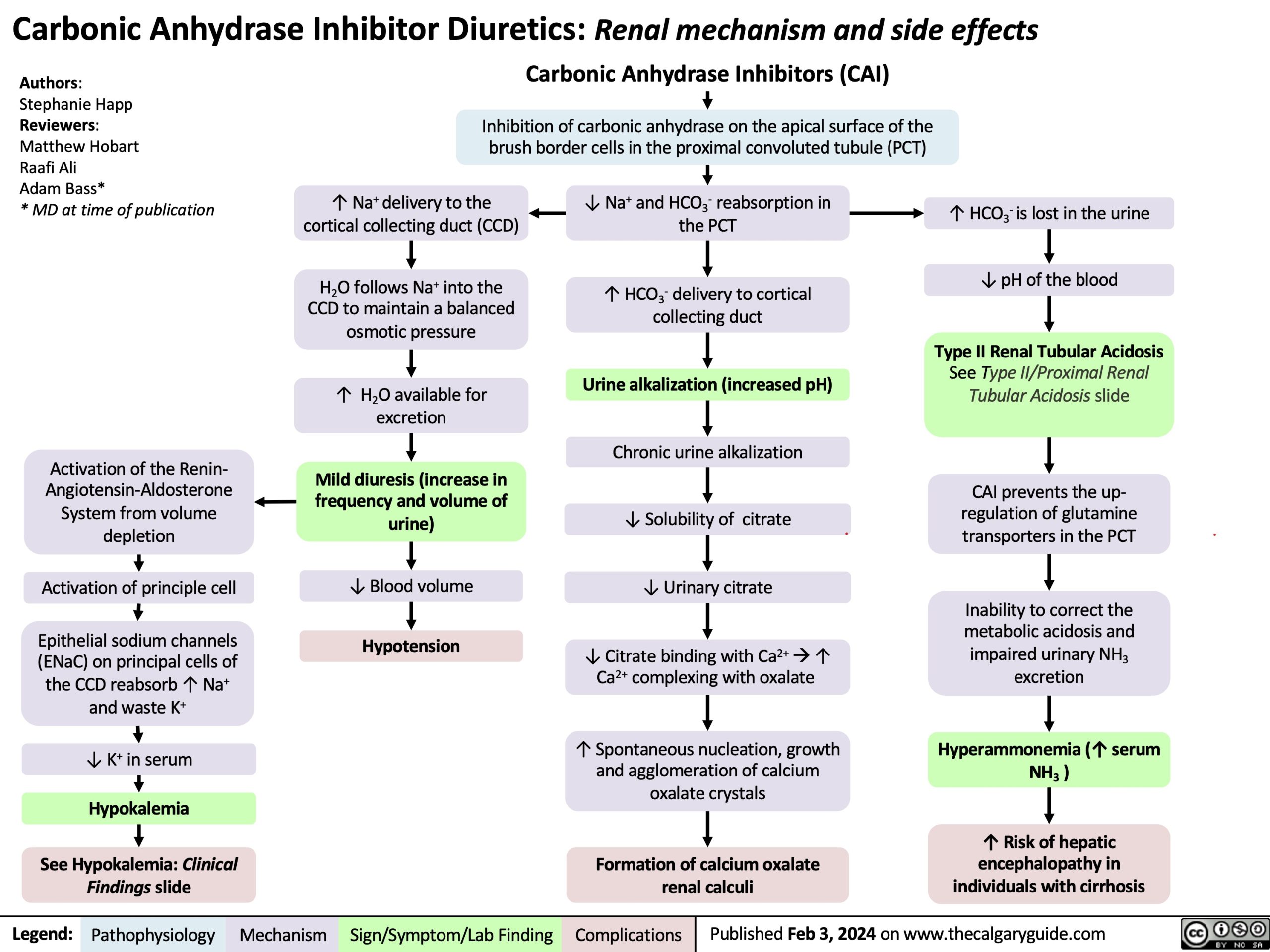
Inhibition of carbonic anhydrase on the apical surface of the brush border cells in the proximal convoluted tubule (PCT)
Activation of the Renin- Angiotensin-Aldosterone Systemfromvolume depletion
Activation of principle cell
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+ and waste K+
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical
Findings slide
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H2O available for excretion
Mild diuresis (increase in frequencyandvolumeof urine)
↓ Blood volume
Hypotension
↓ Na+ and HCO3- reabsorption in the PCT
↑ HCO3- delivery to cortical collecting duct
Urine alkalization (increased pH)
Chronic urine alkalization
↓Solubilityof citrate
↓ Urinary citrate
↓ Citrate binding with Ca2+à↑ Ca2+ complexing with oxalate
↑ Spontaneous nucleation, growth and agglomeration of calcium oxalate crystals
Formation of calcium oxalate renal calculi
↑ HCO3- is lost in the urine ↓ pH of the blood
Type II Renal Tubular Acidosis
See Type II/Proximal Renal Tubular Acidosis slide
CAI prevents the up- regulationofglutamine transporters in the PCT
Inability to correct the metabolic acidosis and impaired urinary NH3 excretion
Hyperammonemia (↑ serum NH3 )
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 3, 2024 on www.thecalgaryguide.com
Carbonic Anhydrase Inhibitor Diuretics: Renal Mechanism and Side Effects Carbonic Anhydrase Inhibitors (CAI)
Inhibition of carbonic anhydrase on the apical surface of the brush border cells of the proximal convoluted tubule (PCT)
Authors: Stephanie Happ Reviewers: Matt Hobart Name Name* * MD at time of publication
↓ Na+ and HCO3- reabsorption in the PCT
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H O available for 2
excretion
Mild diuresis
↓ Blood volume Hypotension
↑ HCO3- delivery to cortical collecting duct
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+
↑ Intracellular Na+ drives Na+/K+ ATPase activity on the principal cells (moving 2 K+ into cell and 3 Na+ out into the peritubular capillary)
↑ Intracellular K+ drives H+/K+ ATPase activity on the intercalated cells (moving 1 H+ into cell and 1 K+ out into the tubular filtrate)
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical Findings slide
Urine alkalization
↑ HCO3- is lost in the urine, leading to ↓ pH of the blood
Renal Tubular Acidosis Type II
See Type II/Proximal Renal Tubular Acidosis slide
CAI inhibit the up-regulation of glutamine transporters in the PCT
Inability to correct the metabolic acidosis and
impaired urinary NH3 excretion
Hyperammonemia
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Chronic urine alkalization leads to marked ↓ in urinary citrate
↓ Ability of citrate to bind to Ca2+ and calcium oxalate stones
↓ Inhibition of spontaneous nucleation
↓ Prevention of growth and agglomeration of crystals
Formation of calcium oxalate renal calculi
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com