Bronchiectasis: Pathogenesis and clinical findings
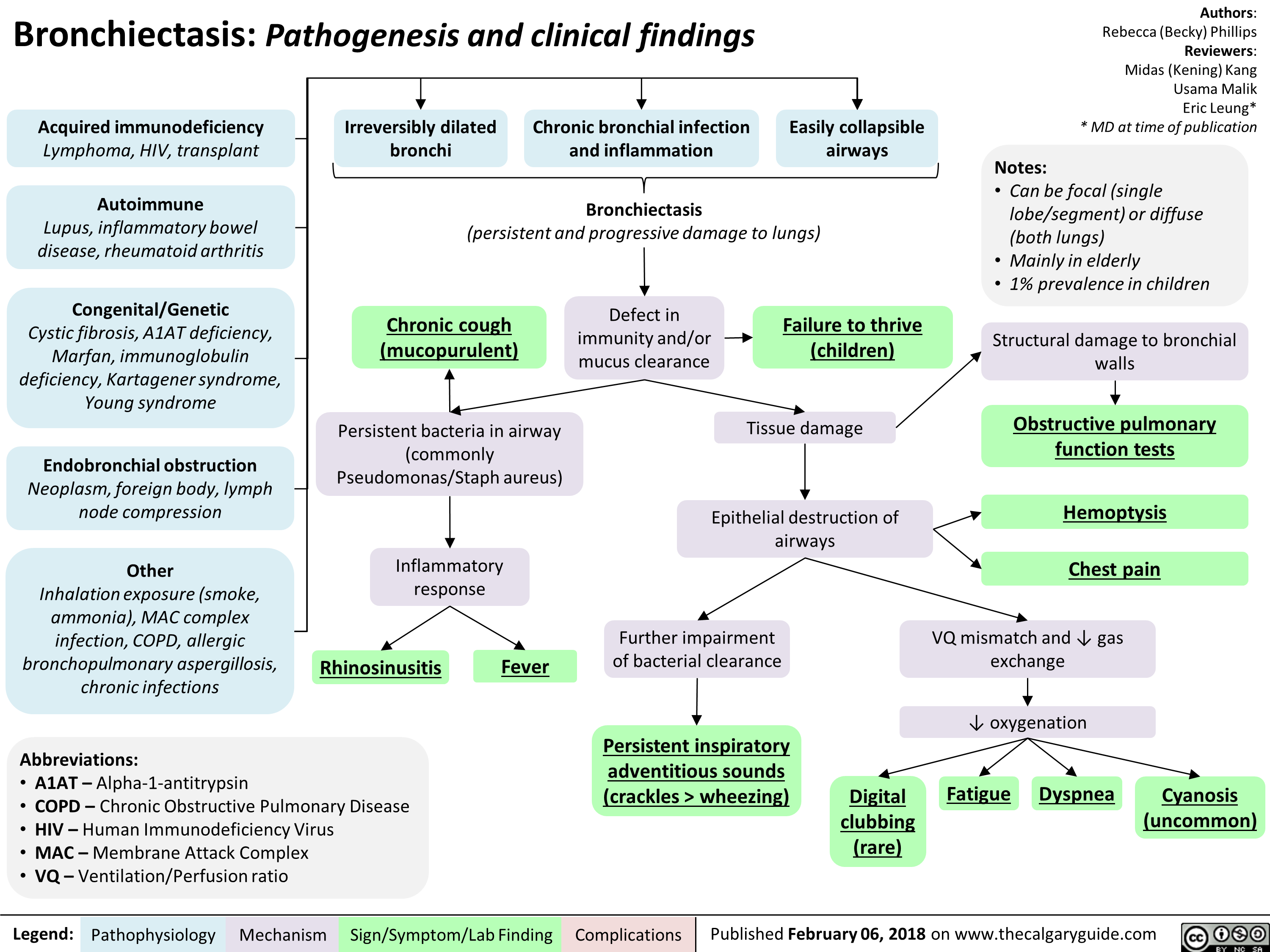
Acquired immunodeficiency Lymphoma, HIV, transplant
Autoimmune Lupus, inflammatory bowel disease, rheumatoid arthritis
Congenital/Genetic Cystic fibrosis, A1AT deficiency, Marfan, immunoglobulin deficiency, Kartagener syndrome, Young syndrome
Endobronchial obstruction Neoplasm, foreign body, lymph node compression
Other Inhalation exposure (smoke, ammonia), MAC complex infection, COPD, allergic bronchopulmonary aspergillosis, chronic infections
Irreversibly dilated bronchi
Chronic bronchial infection and inflammation
1
Easily collapsible airways
I Bronchiectasis (persistent and progressive damage to lungs)
Chronic cough (mucopurulent)
Defect in immunity and/or mucus clearance
Persistent bacteria in airway (commonly Pseudomonas/Staph aureus)
Inflammatory response
Rhinosinusitis
Abbreviations: • A1AT — Alpha-1-antitrypsin • COPD — Chronic Obstructive Pulmonary Disease • HIV — Human Immunodeficiency Virus • MAC — Membrane Attack Complex • VQ— Ventilation/Perfusion ratio
Legend:
Pathophysiology Mechanism
Fever
Sign/Symptom/Lab Finding
Failure to thrive (children)
Authors: Rebecca (Becky) Phillips Reviewers: Midas (Kening) Kang Usama Malik Eric Leung* * MD at time of publication
Notes: • Can be focal (single lobe/segment) or diffuse (both lungs) • Mainly in elderly • 1% prevalence in children
Tissue damage
Epithelial destruction of airways
Further impairment of bacterial clearance
Persistent inspiratory adventitious sounds (crackles > wheezing)
Complications
Structural damage to bronchial walls
Obstructive pulmonary function tests
Hemoptysis
Chest pain
VQ mismatch and 4, gas exchange
4, oxygenation
Digital clubbing (rare)
Fatigue Dyspnea
Cyanosis (uncommon)