Benign Paroxysmal Positional Vertigo (BPPV): Pathogenesis and Clinical Findings
Authors: Ryan Chan, Jonathan Wong, Mehul Gupta, Yan Yu* Reviewers: Davis Maclean, Saud Sunba, Euna Hwang* * MD at time of publication
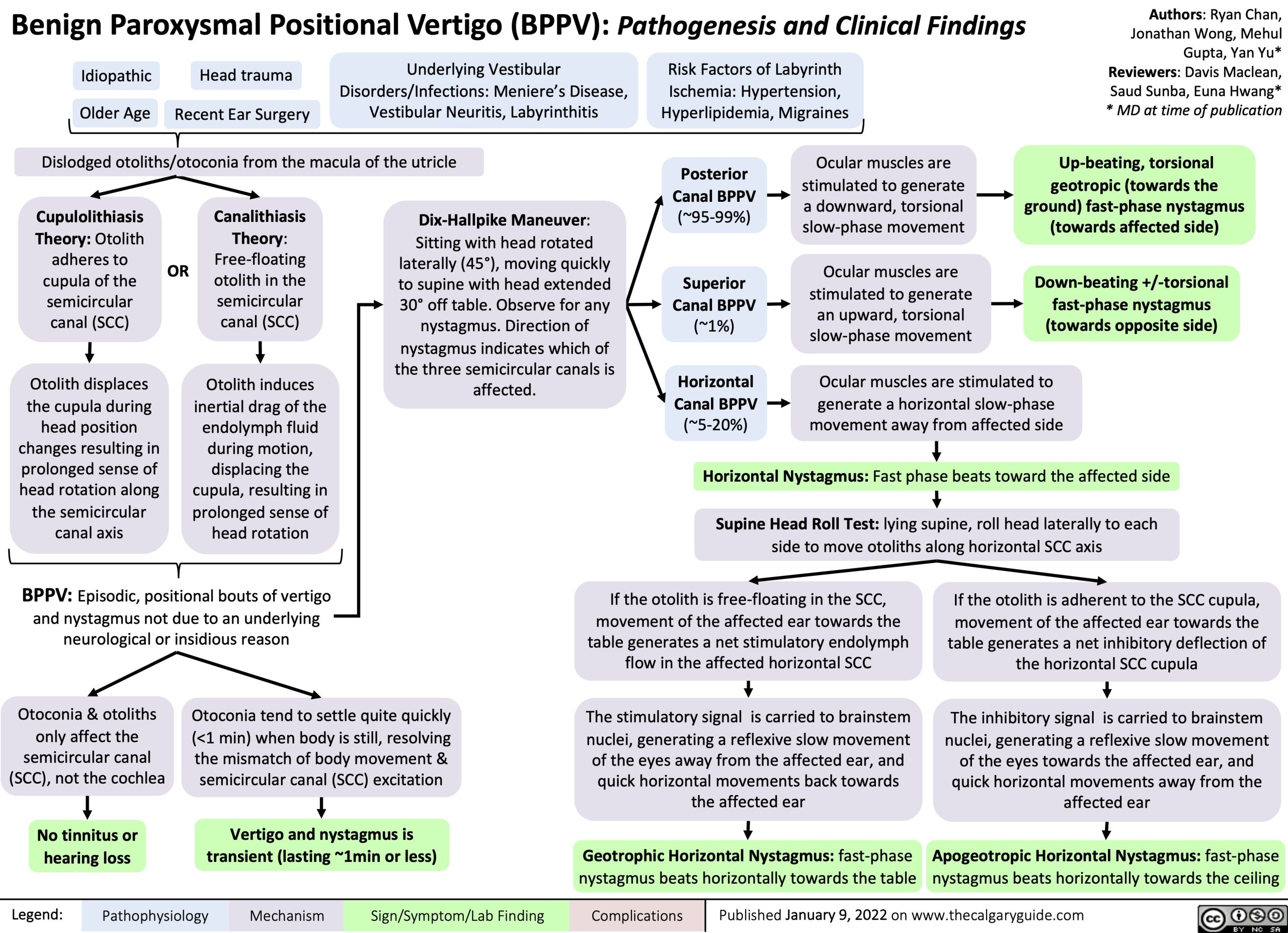
Up-beating, torsional geotropic (towards the
ground) fast-phase nystagmus (towards affected side)
Down-beating +/-torsional fast-phase nystagmus (towards opposite side)
Idiopathic Older Age
Head trauma
Recent Ear Surgery
Underlying Vestibular Disorders/Infections: Meniere’s Disease, Vestibular Neuritis, Labyrinthitis
Risk Factors of Labyrinth
Ischemia: Hypertension, Hyperlipidemia, Migraines
Dislodged otoliths/otoconia from the macula of the utricle
Posterior Canal BPPV (~95-99%)
Superior Canal BPPV (~1%)
Horizontal Canal BPPV (~5-20%)
Ocular muscles are stimulated to generate
a downward, torsional slow-phase movement
Ocular muscles are stimulated to generate
an upward, torsional slow-phase movement
Cupulolithiasis Theory: Otolith adheres to cupula of the semicircular canal (SCC)
Otolith displaces the cupula during head position changes resulting in prolonged sense of head rotation along the semicircular canal axis
OR
Canalithiasis Theory: Free-floating otolith in the semicircular canal (SCC)
Otolith induces inertial drag of the endolymph fluid during motion, displacing the cupula, resulting in prolonged sense of head rotation
Dix-Hallpike Maneuver: Sitting with head rotated laterally (45°), moving quickly to supine with head extended 30° off table. Observe for any nystagmus. Direction of nystagmus indicates which of the three semicircular canals is affected.
Ocular muscles are stimulated to generate a horizontal slow-phase movement away from affected side
Horizontal Nystagmus: Fast phase beats toward the affected side Supine Head Roll Test: lying supine, roll head laterally to each
side to move otoliths along horizontal SCC axis
BPPV: Episodic, positional bouts of vertigo and nystagmus not due to an underlying neurological or insidious reason
If the otolith is free-floating in the SCC, movement of the affected ear towards the table generates a net stimulatory endolymph flow in the affected horizontal SCC
The stimulatory signal is carried to brainstem nuclei, generating a reflexive slow movement
of the eyes away from the affected ear, and quick horizontal movements back towards the affected ear
Geotrophic Horizontal Nystagmus: fast-phase nystagmus beats horizontally towards the table
If the otolith is adherent to the SCC cupula,
movement of the affected ear towards the table generates a net inhibitory deflection of the horizontal SCC cupula
The inhibitory signal is carried to brainstem nuclei, generating a reflexive slow movement of the eyes towards the affected ear, and quick horizontal movements away from the affected ear
Apogeotropic Horizontal Nystagmus: fast-phase nystagmus beats horizontally towards the ceiling
Otoconia & otoliths only affect the
semicircular canal (SCC), not the cochlea
No tinnitus or hearing loss
Otoconia tend to settle quite quickly (<1 min) when body is still, resolving the mismatch of body movement & semicircular canal (SCC) excitation
Vertigo and nystagmus is transient (lasting ~1min or less)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 9, 2022 on www.thecalgaryguide.com