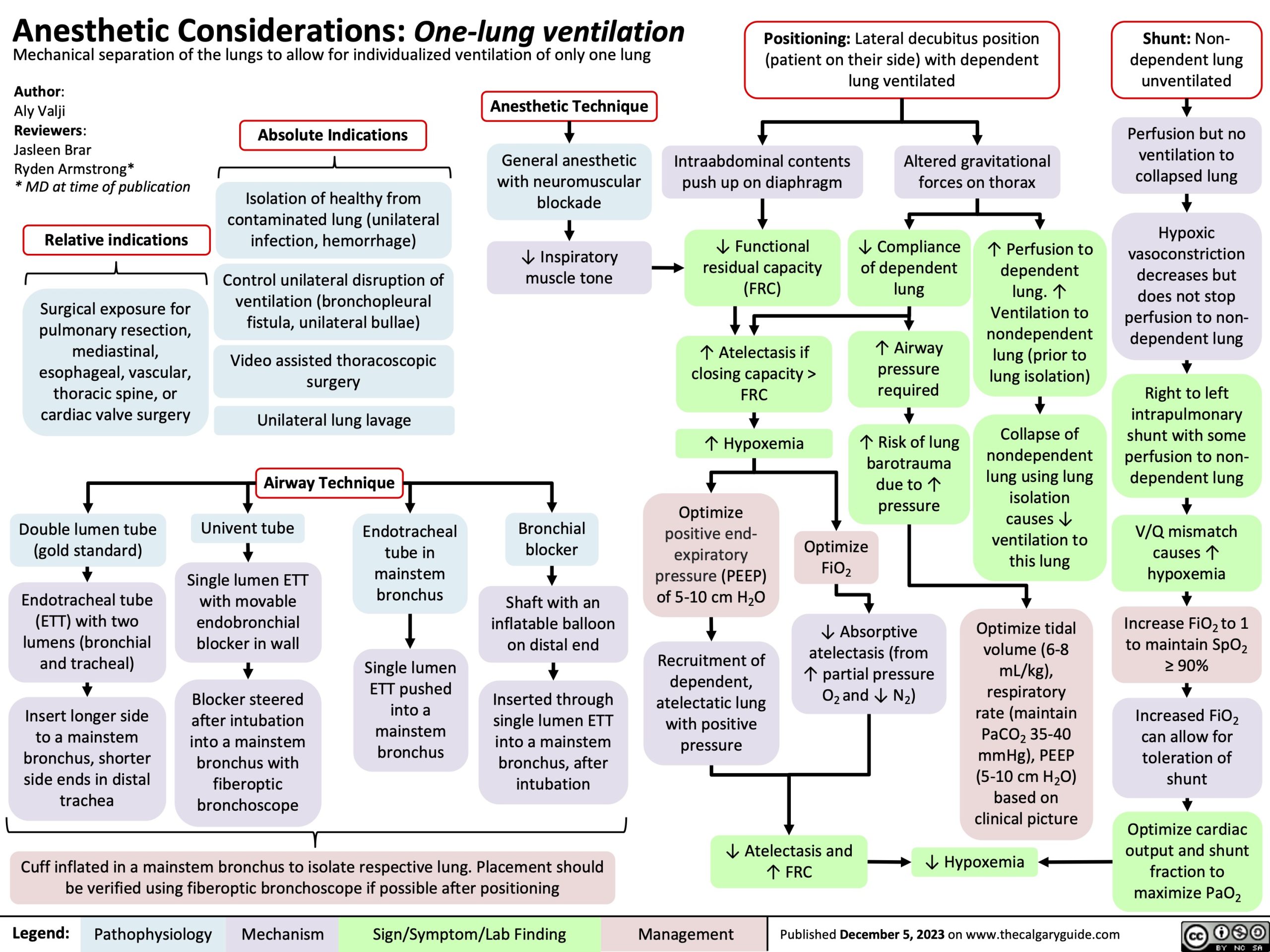
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Shunt: Non- dependent lung unventilated
Perfusion but no ventilation to collapsed lung
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch causes ↑ hypoxemia
Increase FiO2 to 1 to maintain SpO2 ≥ 90%
Increased FiO2 can allow for toleration of shunt
Optimize cardiac output and shunt fraction to maximize PaO2
Author:
Aly Valji
Reviewers:
Jasleen Brar
Ryden Armstrong*
* MD at time of publication
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Double lumen tube (gold standard)
Endotracheal tube (ETT) with two lumens (bronchial and tracheal)
Insert longer side to a mainstem bronchus, shorter side ends in distal trachea
Absolute Indications
Isolation of healthy from contaminated lung (unilateral infection, hemorrhage)
Control unilateral disruption of ventilation (bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Airway Technique
Anesthetic Technique
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Intraabdominal contents push up on diaphragm
↓ Functional residual capacity (FRC)
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize
Altered gravitational forces on thorax
↓ Compliance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent lung. ↑ Ventilation to nondependent lung (prior to lung isolation)
Collapse of nondependent lung using lung isolation causes ↓ ventilation to this lung
Optimize tidal volume (6-8 mL/kg), respiratory rate (maintain PaCO2 35-40 mmHg), PEEP (5-10 cm H2O) based on clinical picture
Univent tube
Single lumen ETT with movable endobronchial blocker in wall
Blocker steered after intubation into a mainstem bronchus with fiberoptic bronchoscope
Endotracheal tube in mainstem bronchus
Single lumen ETT pushed into a mainstem bronchus
Bronchial blocker
Shaft with an inflatable balloon on distal end
Inserted through single lumen ETT into a mainstem bronchus, after intubation
positive end- expiratory pressure (PEEP) of 5-10 cm H2O
Recruitment of dependent, atelectatic lung with positive pressure
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Cuff inflated in a mainstem bronchus to isolate respective lung. Placement should be verified using fiberoptic bronchoscope if possible after positioning
↓ Atelectasis and ↑ FRC
↓ Hypoxemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Management
Published December 5, 2023 on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Shunt: Non- dependent lung unventilated
Perfusion but no ventilation to collapsed lung
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to 1 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Author:
Aly Valji
Reviewers:
Jasleen Brar
Dr. Armstrong*
* MD at time of publication
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Double lumen tube (DLT)
Two endotracheal tubes (ETT) bonded together
Insert longer side to a mainstem bronchus, shorter side ends in distal trachea
Absolute Indications
Isolation of healthy from contaminated lung (unilateral infection, hemorrhage)
Control unilateral disruption of ventilation (bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Airway Technique
Anesthetic Technique
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Intraabdominal contents push up on diaphragm
↓ Functional residual capacity (FRC)
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize
Altered gravitational forces on thorax
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume (6-8 mL/kg), respiratory rate (maintain PaCO2 35-40 mmHg), PEEP (5-10 cm H2O) based on clinical picture
Univent tube
Single lumen ETT with movable endobronchial blocker in wall
Blocker steered after intubation into a mainstem bronchus with fiberoptic bronchoscope
Endotracheal tube in mainstem bronchus
Single lumen ETT pushed into a mainstem bronchus
Bronchial blocker
Shaft with an inflatable balloon on distal end
Inserted through single lumen ETT into a mainstem bronchus, after intubation
positive end- expiratory pressure (PEEP) of 5-10 cm H2O
Recruitment of dependent, atelectatic lung with positive pressure
Optimize
FiO
2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Cuff inflated in a mainstem bronchus to isolate respective lung. Placement should be verified using fiberoptic bronchoscope if possible after positioning
↓ Atelectasis and ↑ FRC
↓ Hypoxemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Management
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine surgery
Absolute Indications
Isolation of healthy from contaminated lung (Unilateral infection or hemorrhage)
Control unilateral disruption of ventilation (Bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia
Altered gravitational forces on thorax
Shaft with an inflatable balloon on distal end. Inserted through a single lumen ETT after intubation into a mainstem bronchi
Single lumen ETT pushed into a mainstem bronchus
Optimize positive end-expiratory pressure (PEEP))
Recruitment of dependent, atelectatic lung with positive pressure
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
Bronchial blocker
Endotracheal tube in mainstem bronchus
Technique
Univent tube
Double lumen tube (DLT)
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Single lumen ETT with movable endobronchial blocker housed in wall of ETT. Blocker maneuvered after intubation into a mainstem bronchus
Two endotracheal tubes (ETT) bonded together. Longer side goes into a mainstem bronchus, shorter side ends in distal trachea
↓ Atelectasis and ↑ FRC
↓ V/Q mismatch
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO to 2
maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Comorbidity: Likely underlying pulmonary disease
Pre-operative evaluation
Pulmonary function testing
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Multidisciplinary determination of fitness for surgery
Pulmonary hemorrhage Whole lung lavage Unilateral infection Bronchopleural fistula
Isolation of affected lung from unaffected lung
Pulmonary resection
Mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Operative lung deflated to expose surgical site
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize positive
Altered gravitational forces on thorax
Contraindications
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
Bilateral lung ventilation dependency
Hemodynamic instability
Severe hypoxia Severe COPD
Severe pulmonary hypertension
Potentially unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass
Known difficult airway
Risk of dislodging mass and inability to secure airway
Pursue more advanced airway techniques
end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O and ↓ N )
2
2
↓ Atelectasis and ↑ FRC
Post-operative pain management
Thoracotomy or VATS procedure causing ↑ pain along thoracic dermatomes
Epidural
Paravertebral block
Anesthetic injected into epidural space
Anesthetic injected into paravertebral spaces
Bilateral spinal nerve blockade below desired spinal level
Ipsilateral spinal nerve and sympathetic chain blockade in thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Comorbidity: Likely underlying pulmonary disease
Pre-operative evaluation
Pulmonary function testing
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Multidisciplinary determination of fitness for surgery
Anesthetic injected into epidural space
Anesthetic injected into paravertebral spaces
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Pulmonary hemorrhage Whole lung lavage Unilateral infection Bronchopleural fistula
Isolation of affected lung and unaffected lung
Pulmonary resection
Mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Operative lung deflated to expose surgical site
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis ↑ Hypoxemia
Optimize
positive end- expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
↓ Atelectasis and ↑ FRC
Altered gravitational forces on thorax
Contraindications
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Bilateral lung ventilation dependency
Hemodynamically unstable
Severe hypoxia Severe COPD
Severe pulmonary hypertension
Unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass
Known difficult airway
Risk of dislodging mass and inability to secure airway
Pursue more advanced airway techniques
Post-operative pain management
Thoracotomy or VATS procedure causing ↑ pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired spinal level
Ipsilateral spinal nerve and sympathetic chain blockade in thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Name* * MD at time of publication
Indication
Contraindications
Comorbidity: Likely underlying pulmonary disease
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
General anesthetic with neuromuscular blockade
Post-operative pain management
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Operative lung deflated to expose surgical site
Isolation of affected lung and unaffected lung
Dependency on bilateral lung ventilation, hemodynamically unstable, severe hypoxia, severe COPD, or severe pulmonary hypertension
Unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass or known difficult Pursue more advanced
Risk of dislodging mass and inability to secure airway
Multidisciplinary determination of fitness for surgery
airway
Pulmonary function testing
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
airway techniques
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Pre-operative evaluation
Non- dependent lung not ventilated
Altered gravitational forces on thorax
Intraabdominal contents push up on diaphragm
↓ Inspiratory muscle tone
Likely procedure is thoracotomy or VATS causing ↑ pain along thoracic dermatomes
Right to left intrapulmonary shunt with some perfusion to non- dependent lung still present
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
↓ Atelectasis and ↑ FRC
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
↓ Functional residual capacity (FRC)
↓ Ventilation-perfusion (V/Q) mismatch
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma due to ↑ pressure
Intervention:
Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
Epidural
Paravertebral block
Anesthetic injected into epidural space
Bilateral spinal nerve blockade below desired spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in thoracic paravertebral spaces dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation
Author:
Aly Valji Reviewers: Name* * MD at time of publication
One lung ventilation: mechanical separation of the lungs to allow for individualized ventilation of only one lung
Indication
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Exposure of surgical site by deflation of operative lung
Isolation of affected lung and unaffected lung
Dependency on bilateral lung ventilation, Contraindications hemodynamically unstable, severe hypoxia, severe
COPD, or severe pulmonary hypertension
Intraluminal airway obstruction/mass or known difficult airway
Pursue more advanced airway techniques
Unable to tolerate one lung ventilation
Risk of dislodging mass and inability to secure airway
Likely underlying Pre-operative Pulmonary pulmonary disease evaluation function testing
Overall clinical picture, forced expiratory Determination of volume (FEV1), and diffusion capacity (DLCO) fitness for surgery
Right to left intrapulmonary shunt as some perfusion to non- dependent lung is still present
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
Non- dependent lung not ventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
V/Q mismatch from shunt increases hypoxemia
Intervention:
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for non-dependent lung
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP
↓ Atelectasis and ↑ FRC
Positioning: Lateral position with dependent lung ventilated
Altered gravitational forces on thorax
↓ Ventilation-perfusion (V/Q) mismatch
General anesthetic with neuromuscular blockade
Intraabdominal contents push up on diaphragm
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma
Intervention: Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung from PEEP
↓ Inspiratory muscle tone
↓ Functional residual capacity (FRC)
Post- operative pain management
Thoracotomy or VATS causes pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired Anesthetic injected into epidural space spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in paravertebral spaces thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic considerations: one-lung ventilation
Author:
Aly Valji Reviewers: Name* * MD at time of publication
One lung ventilation: mechanical separation of the lungs to allow for individualized ventilation of only one lung
Indication
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Exposure of surgical site by deflation of one lung
Isolation of one lung from other
Dependency on bilateral lung ventilation, Contraindications hemodynamically unstable, severe hypoxia, severe
COPD, or severe pulmonary hypertension
Intraluminal airway obstruction/mass or known difficult airway
Pursue more advanced airway techniques
Unable to tolerate one lung ventilation
Risk of dislodging mass and inability to secure airway
Pre-operative evaluation given likely Pulmonary Forced expiratory volume (FEV1) Determination of underlying pulmonary disease function testing Diffusion capacity (DLCO) fitness for surgery
Non- dependent lung not ventilated
Hypoxic vasoconstriction decreases but does not stop perfusion of non- dependent lung
Vasodilation of dependent lung pulmonary vasculature
Right to left intrapulmonary shunt causes V/Q mismatch
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
↑ Hypoxemia
Intervention:
Increase FiO2 to maintain SpO2 ≥ 90%
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP
↓ Atelectasis and ↑ FRC
Positioning: Lateral decubitus with dependent lung ventilated
Altered gravitational forces on thorax
↓ Ventilation-perfusion (V/Q) mismatch
General anesthetic with neuromuscular blockade
Intraabdominal contents push up on diaphragm
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma
Intervention: Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent lung
↓ Inspiratory muscle tone
↓ Functional residual capacity (FRC)
Post- operative pain management
Thoracotomy or VATS causes pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired Anesthetic injected into epidural space spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in paravertebral spaces thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com