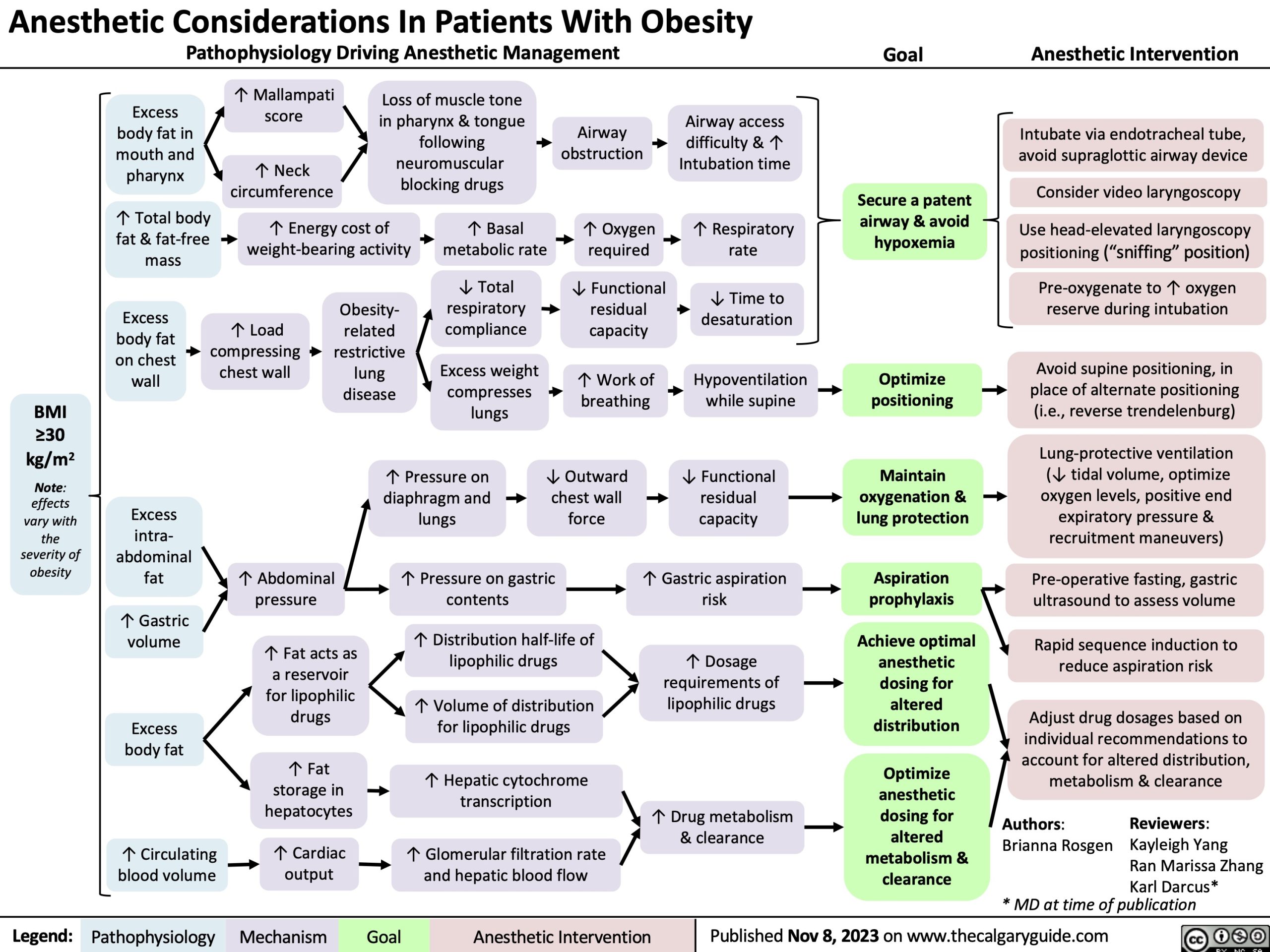
Anesthetic Considerations In Patients With Obesity
Pathophysiology Driving Anesthetic Management Goal Anesthetic Intervention
Excess body fat in mouth and pharynx
↑ Total body fat & fat-free mass
↑ Mallampati score
↑ Neck circumference
Loss of muscle tone in pharynx & tongue following
neuromuscular blocking drugs
Airway access
difficulty & ↑ Intubation time
↑ Respiratory rate
↓ Time to desaturation
Hypoventilation while supine
↓ Functional residual capacity
↑ Gastric aspiration risk
↑ Dosage requirements of lipophilic drugs
↑ Drug metabolism & clearance
↑ Energy cost of weight-bearing activity
↑ Basal metabolic rate
↓ Total respiratory compliance
Excess weight compresses lungs
Airway obstruction
↑ Oxygen required
↓ Functional residual capacity
↑ Work of breathing
Secure a patent airway & avoid hypoxemia
Optimize positioning
Maintain oxygenation & lung protection
Aspiration prophylaxis
Achieve optimal anesthetic dosing for altered distribution
Optimize anesthetic dosing for altered metabolism & clearance
Intubate via endotracheal tube, avoid supraglottic airway device
Consider video laryngoscopy
Use head-elevated laryngoscopy positioning (“sniffing” position)
Pre-oxygenate to ↑ oxygen reserve during intubation
Avoid supine positioning, in place of alternate positioning (i.e., reverse trendelenburg)
Lung-protective ventilation (↓ tidal volume, optimize oxygen levels, positive end
expiratory pressure & recruitment maneuvers)
Pre-operative fasting, gastric ultrasound to assess volume
Rapid sequence induction to reduce aspiration risk
Adjust drug dosages based on individual recommendations to account for altered distribution, metabolism & clearance
Excess body fat on chest wall
Excess intra- abdominal fat
↑ Gastric volume
Excess body fat
↑ Circulating blood volume
Obesity- related restrictive lung disease
↑ Load compressing chest wall
BMI
≥30
kg/m2
Note: effects vary with the severity of obesity
↑ Pressure on diaphragm and lungs
↓ Outward chest wall force
↑ Abdominal pressure
↑ Fat acts as a reservoir for lipophilic drugs
↑ Fat storage in hepatocytes
↑ Cardiac output
↑ Pressure on gastric contents
↑ Distribution half-life of lipophilic drugs
↑ Volume of distribution for lipophilic drugs
↑ Hepatic cytochrome transcription
↑ Glomerular filtration rate and hepatic blood flow
Authors: Brianna Rosgen
Reviewers: Kayleigh Yang
Ran Marissa Zhang
Karl Darcus*
* MD at time of publication
Legend:
Pathophysiology
Mechanism
Goal
Anesthetic Intervention
Published Nov 8, 2023 on www.thecalgaryguide.com