Anesthetic Considerations: Hemodynamic Goals (“CRRAP Goals”) for Patients with Aortic Stenosis Undergoing Non-Cardiac Surgery
CRRAP Goals:
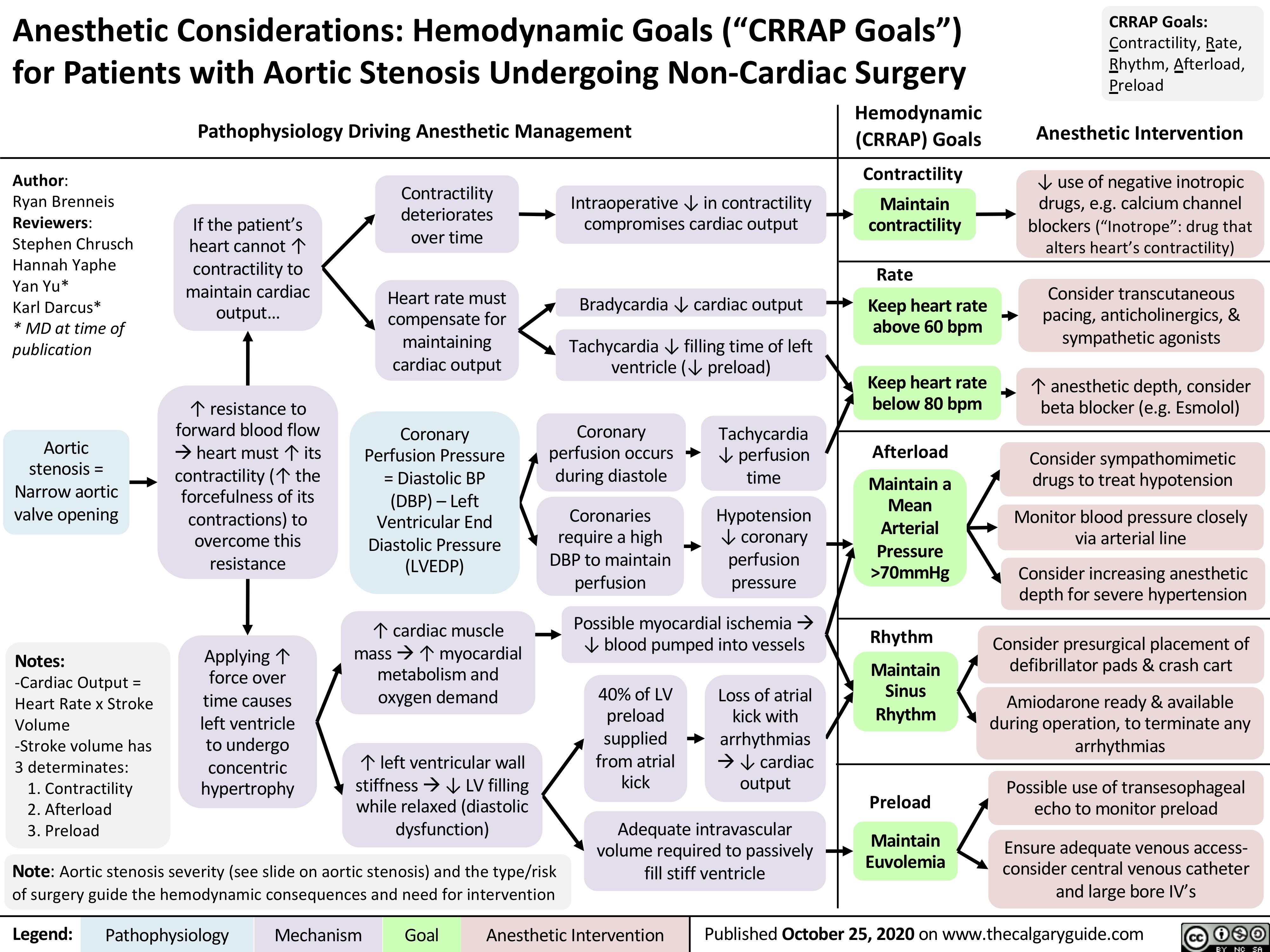
Contractility, Rate, Rhythm, Afterload, Preload
Pathophysiology Driving Anesthetic Management Hemodynamic Anesthetic Intervention (CRRAP) Goals
Author:
Ryan Brenneis Reviewers: Stephen Chrusch Hannah Yaphe Yan Yu*
Karl Darcus*
* MD at time of publication
Aortic stenosis = Narrow aortic valve opening
Notes:
-Cardiac Output = Heart Rate x Stroke Volume
-Stroke volume has 3 determinates:
1. Contractility 2. Afterload
3. Preload
If the patient’s heart cannot ↑ contractility to maintain cardiac output…
↑ resistance to forward blood flow àheart must ↑ its contractility (↑ the forcefulness of its contractions) to overcome this resistance
Applying ↑ force over time causes left ventricle to undergo concentric hypertrophy
Contractility deteriorates over time
Heart rate must compensate for maintaining cardiac output
Coronary Perfusion Pressure = Diastolic BP (DBP) – Left Ventricular End Diastolic Pressure (LVEDP)
↑ cardiac muscle massà↑ myocardial metabolism and oxygen demand
↑ left ventricular wall stiffnessà↓ LV filling while relaxed (diastolic dysfunction)
Intraoperative ↓ in contractility compromises cardiac output
Bradycardia ↓ cardiac output
Tachycardia ↓ filling time of left ventricle (↓ preload)
Coronary perfusion occurs during diastole
Coronaries require a high DBP to maintain perfusion
Tachycardia ↓ perfusion time
Hypotension ↓ coronary perfusion pressure
Possible myocardial ischemiaà ↓ blood pumped into vessels
40% of LV preload supplied from atrial kick
Loss of atrial kick with arrhythmias à↓ cardiac output
Note: Aortic stenosis severity (see slide on aortic stenosis) and the type/risk of surgery guide the hemodynamic consequences and need for intervention
Adequate intravascular volume required to passively fill stiff ventricle
Contractility
↓ use of negative inotropic Maintain drugs, e.g. calcium channel
contractility blockers (“Inotrope”: drug that alters heart’s contractility)
Rate
Keep heart rate above 60 bpm
Keep heart rate below 80 bpm
Consider transcutaneous pacing, anticholinergics, & sympathetic agonists
↑ anesthetic depth, consider beta blocker (e.g. Esmolol)
Afterload
Maintain a Mean Arterial Pressure >70mmHg
Consider sympathomimetic drugs to treat hypotension
Monitor blood pressure closely via arterial line
Consider increasing anesthetic depth for severe hypertension
Rhythm
Maintain Sinus Rhythm
Consider presurgical placement of defibrillator pads & crash cart
Amiodarone ready & available during operation, to terminate any arrhythmias
Preload
Maintain Euvolemia
Possible use of transesophageal echo to monitor preload
Ensure adequate venous access- consider central venous catheter and large bore IV’s
Legend:
Pathophysiology
Mechanism
Goal
Anesthetic Intervention
Published October 25, 2020 on www.thecalgaryguide.com