Adult Pneumonia: Pathogenesis and clinical findings
Author: Laura Byford-Richardson Reviewers: Tara Shannon, *Yan Yu, Sadie Kutz , Natalie Morgunov, *Kerri Johannson, *Julie Carson *MD at time of publication
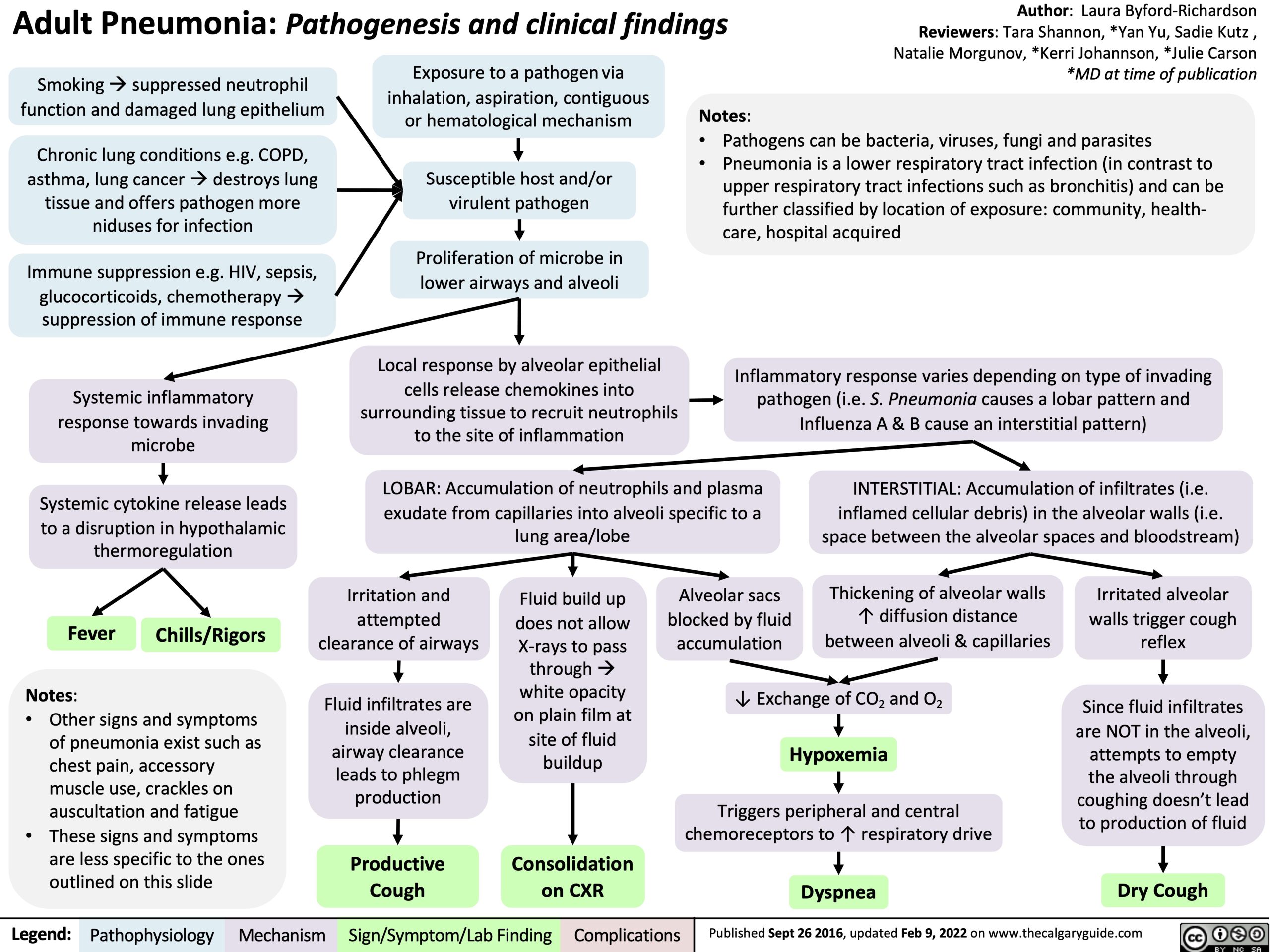
Smoking à suppressed neutrophil function and damaged lung epithelium
Chronic lung conditions e.g. COPD, asthma, lung canceràdestroys lung tissue and offers pathogen more niduses for infection
Immune suppression e.g. HIV, sepsis, glucocorticoids, chemotherapyà suppression of immune response
Systemic inflammatory response towards invading microbe
Systemic cytokine release leads to a disruption in hypothalamic thermoregulation
Exposure to a pathogen via
inhalation, aspiration, contiguous Notes:
or hematological mechanism
Susceptible host and/or virulent pathogen
Proliferation of microbe in lower airways and alveoli
Local response by alveolar epithelial cells release chemokines into surrounding tissue to recruit neutrophils to the site of inflammation
• Pathogens can be bacteria, viruses, fungi and parasites
• Pneumonia is a lower respiratory tract infection (in contrast to
upper respiratory tract infections such as bronchitis) and can be further classified by location of exposure: community, health- care, hospital acquired
Inflammatory response varies depending on type of invading pathogen (i.e. S. Pneumonia causes a lobar pattern and Influenza A & B cause an interstitial pattern)
LOBAR: Accumulation of neutrophils and plasma exudate from capillaries into alveoli specific to a lung area/lobe
INTERSTITIAL: Accumulation of infiltrates (i.e. inflamed cellular debris) in the alveolar walls (i.e. space between the alveolar spaces and bloodstream)
Fever
Notes:
• Other signs and symptoms
of pneumonia exist such as chest pain, accessory muscle use, crackles on auscultation and fatigue
• These signs and symptoms are less specific to the ones outlined on this slide
Irritation and attempted clearance of airways
Fluid infiltrates are inside alveoli, airway clearance leads to phlegm production
Productive Cough
Fluid build up does not allow X-rays to pass through à white opacity on plain film at site of fluid buildup
Consolidation on CXR
Alveolar sacs blocked by fluid accumulation
Thickening of alveolar walls ↑ diffusion distance between alveoli & capillaries
Irritated alveolar walls trigger cough reflex
Since fluid infiltrates are NOT in the alveoli, attempts to empty the alveoli through coughing doesn’t lead to production of fluid
Dry Cough
Chills/Rigors
↓ Exchange of CO2 and O2
Hypoxemia
Triggers peripheral and central chemoreceptors to ↑ respiratory drive
Dyspnea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 26 2016, updated Feb 9, 2022 on www.thecalgaryguide.com