Acute Pulmonary Embolism: Computed Tomography Pulmonary Angiogram (CTPA/CTPE)
Virchow’s Triad:
Hypercoagulability, venous stasis, vascular endothelial injury
Image Source: European Society of Radiology
Image: Polo mint sign on axial CTPA.
Image Source: Journal of The Indian Academy of Echocardiography
Image: Railway sign on axial CTPA. Image Source: Moore et al. 2018
Image: Pleural effusion and pulmonary infarction on axial CTPA.
Authors: Aly Valji, Nameerah Wajahat, Omer Mansoor Reviewers: Reshma Sirajee, Sravya Kakumanu, Victória Silva, Mao Ding Vincent Dinculescu* *MD at time of publication
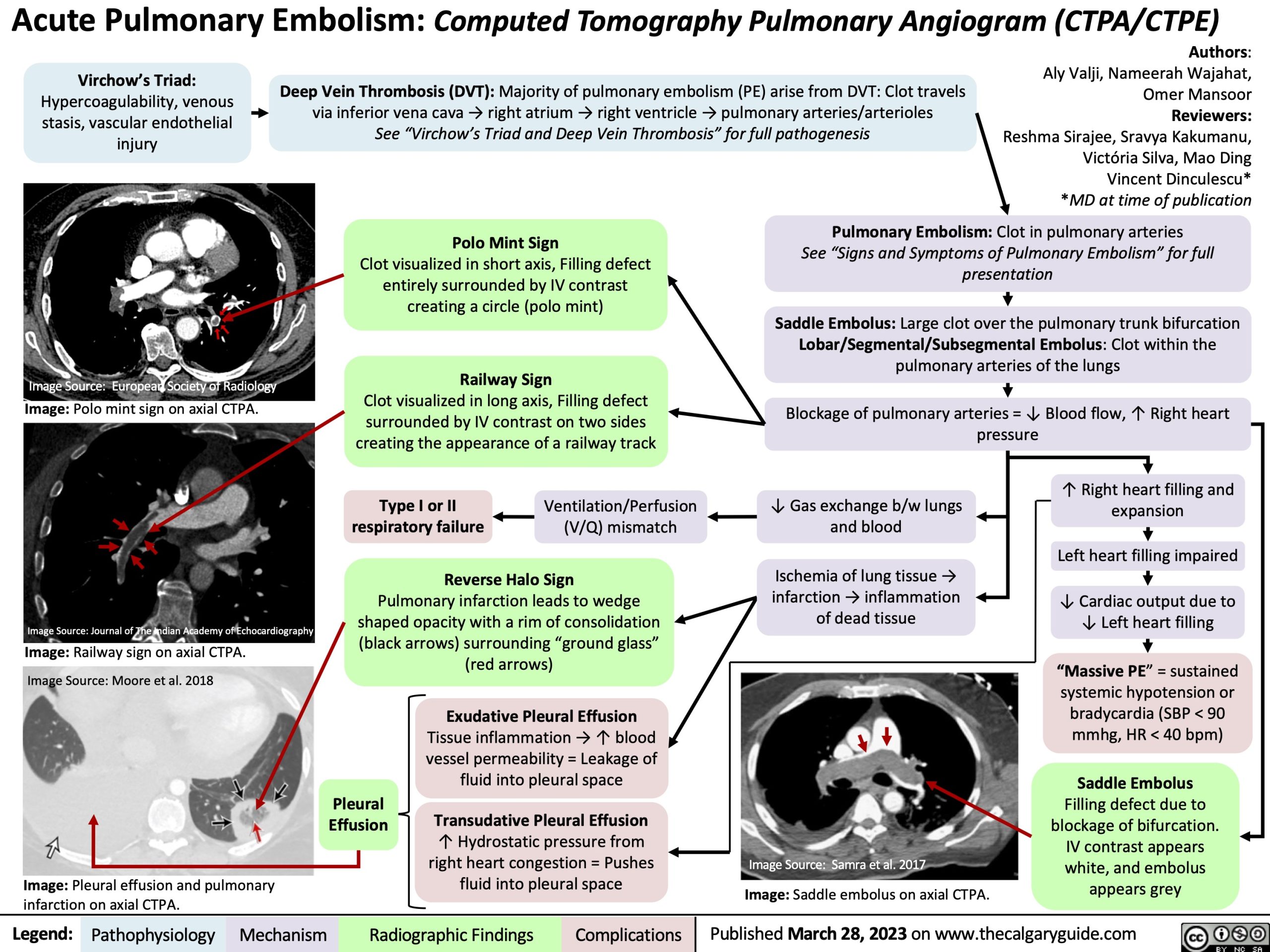
Deep Vein Thrombosis (DVT): Majority of pulmonary embolism (PE) arise from DVT: Clot travels via inferior vena cava → right atrium → right ventricle → pulmonary arteries/arterioles
See “Virchow’s Triad and Deep Vein Thrombosis” for full pathogenesis
Polo Mint Sign
Clot visualized in short axis, Filling defect entirely surrounded by IV contrast creating a circle (polo mint)
Railway Sign
Clot visualized in long axis, Filling defect surrounded by IV contrast on two sides creating the appearance of a railway track
Type I or II Ventilation/Perfusion respiratory failure (V/Q) mismatch
Reverse Halo Sign
Pulmonary infarction leads to wedge shaped opacity with a rim of consolidation (black arrows) surrounding “ground glass” (red arrows)
Pulmonary Embolism: Clot in pulmonary arteries
See “Signs and Symptoms of Pulmonary Embolism” for full presentation
Saddle Embolus: Large clot over the pulmonary trunk bifurcation Lobar/Segmental/Subsegmental Embolus: Clot within the pulmonary arteries of the lungs
Blockage of pulmonary arteries = ↓ Blood flow, ↑ Right heart pressure
↓ Gas exchange b/w lungs and blood
Ischemia of lung tissue → infarction → inflammation of dead tissue
↑ Right heart filling and expansion
Left heart filling impaired
↓ Cardiac output due to ↓ Left heart filling
“Massive PE” = sustained systemic hypotension or bradycardia (SBP < 90 mmhg, HR < 40 bpm)
Saddle Embolus
Filling defect due to blockage of bifurcation. IV contrast appears white, and embolus appears grey
Pleural Effusion
Exudative Pleural Effusion
Tissue inflammation → ↑ blood vessel permeability = Leakage of fluid into pleural space
Transudative Pleural Effusion
↑ Hydrostatic pressure from right heart congestion = Pushes fluid into pleural space
Image Source: Samra et al. 2017
Image: Saddle embolus on axial CTPA.
Legend:
Pathophysiology
Mechanism
Radiographic Findings
Complications
Published March 28, 2023 on www.thecalgaryguide.com