SEARCH RESULTS FOR: Menopause
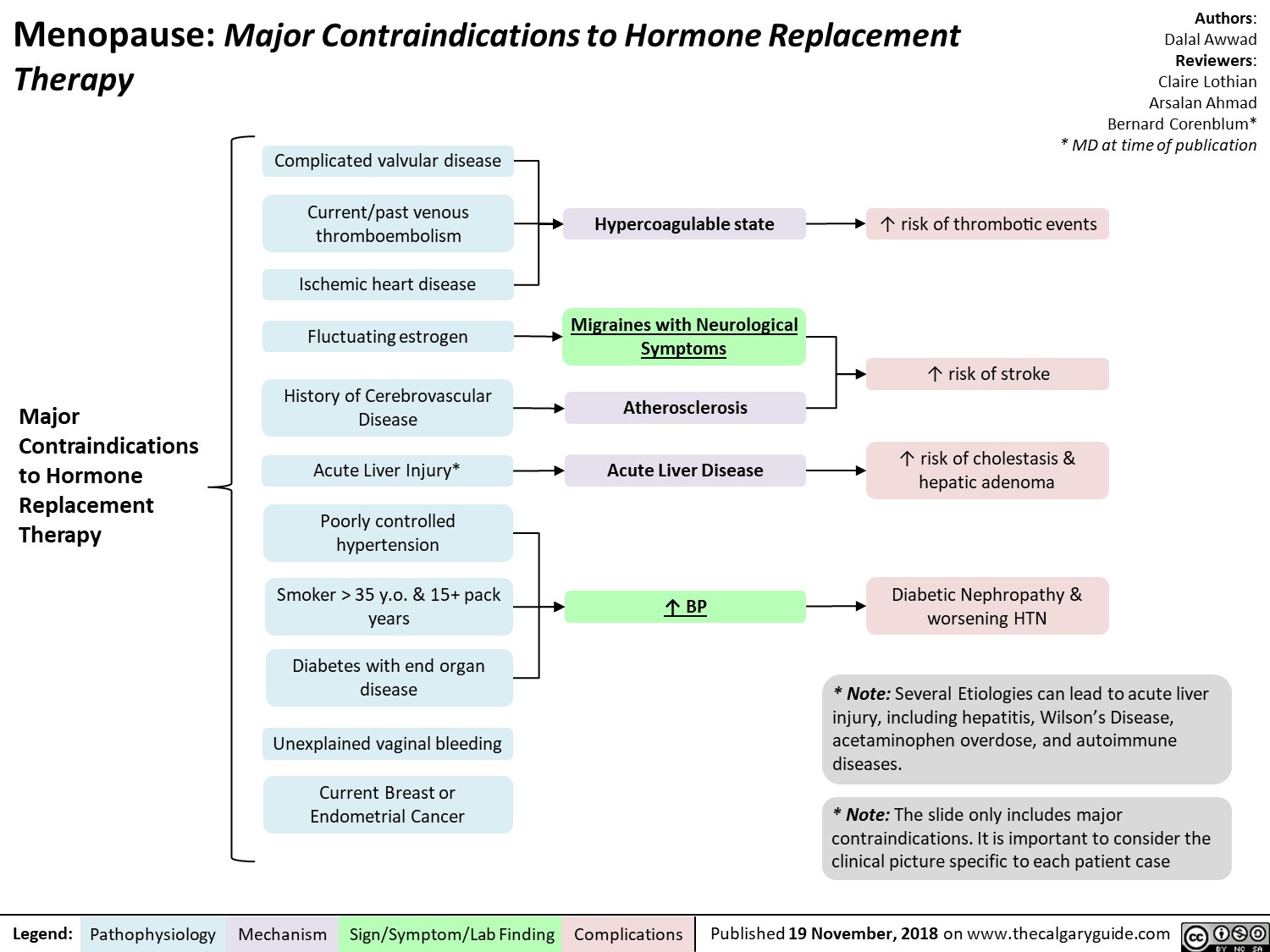
Menopause contraindications to hormone replacement therapy
Uterine-Fibroids
: Pathogenesis and clinical findings
Early Menarche (onset of period)
↑ estrogen exposure in
Obesity
↑ adipose tissue
↑ conversion of androgens into estrogen
Ethnicity (African)
↑ amount of aromatase enzymes
Family History
Complex chromosomal rearrangements
Myometrial Injury
Hypoxia of myometrial cells
Low Parity
Lack of protective pregnancy-induced remodeling to myometrium
Note:
Approximately three-quarters of women have fibroids. Of these, only about one-quarter become symptomatic. Fibroids generally decrease in size after menopause and symptoms improve.
Intracavitary
Fibroid projects into uterine cavity
↑ Endometrial Surface Area ↑ endometrium to proliferate and
lose during menstruation
Age 40-50
lifetime Estrogen stimulates proliferation of uterine smooth muscle cells
Benign proliferation of monoclonal myometrial (uterine wall/muscle) cells into discrete masses
Uterine Fibroids (Leiomyomas)
Benign tumours originating in and consisting of uterine muscle tissue
Fibroids can be located in different areas of the uterus, including the following locations
Authors: Emilee Anderson Reviewers: Danielle Chang Crystal Liu Yan Yu* Aysah Amath* * MD at time of publication
Subserosal
Fibroid grows adjacent to perimetrium into uterine muscle
Enlarged uterus or pelvic mass on bimanual exam
Irregularities in uterine cavity
Transformation of normal myocytes into abnormal myocytes
Submucosal
Fibroid grows adjacent to endometrium into uterine muscle
Intramural
Fibroid is within the thickness of the myometrium
Pedunculated
Fibroid extends into pelvic cavity or uterine cavity on a stalk
Spherical mass on ultrasound
Fibroid ↑ intra-abdominal pressure and puts pressure on adjacent organs
Enlarged Uterine/Pelvic Mass
Repeat shedding over time
Iron Deficiency Anemia
Pelvic Pain
Compression of stomach
Fibroid takes up space
Enlarged Abdomen
Fibroid puts pressure on the cervix
Dyspareunia
Fibroid compress the bladder
Urinary incontinence
Fibroid compress the bladder outlet
Difficulty with voiding
Fibroid compress rectum
Constipation
Embryo cannot implant
Infertility and/or recurrent pregnancy loss
Menorrhagia Dysmenorrhea
Sensation of abdominal fullness
Early Satiety
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2020 on www.thecalgaryguide.com")
abnormal-uterine-bleeding-aub-pathogenesis-and-clinical-findings
 release from hypothalamus
↑Prolactin (see Feedback Loop: Prolactin)
Exogenous estrogen (e.g. estrogen-only birth control)
↑ Peripheral adipose tissue
↑ Aromatase (enzyme present in adipose tissue)
↑ Conversion of androgens to estrogens (aromatization)
Excessive stress, exercise, low body mass (mechanism unclear)
↓ Hypothalamic gonadotropin releasing hormone secretion
↓Luteinizing hormone and follicle stimulating hormone release from pituitary
↑ Estrogen
Heavier bleeding
Angiogenesis in tumour tissue
Polycystic ovarian syndrome (see slide)
Pelvic inflammatory disease
Immature hypothalamic- pituitary-ovarian axis
(an immature axis is transient in most females)
↓ Positive feedback of estrogen in late follicular stage
No LH surge
Adenomyosis (endometrial tissue grows into uterus muscular wall)
Endometrial polyps
Retained products of contraception
Infection
Inflammation of endometrium
Endometrium is more fragile
Anovulatory Bleeding
Leiomyoma (benign tumour in myometrium)
Tara Shannon, Hannah Yaphe, Dr. Sarah Glaze* * MD at time of publication
Ovarian Scarring
Foreign bodies
Intrauterine device perforation
Physical trauma
Impaired follicle maturation
Anovulation
Corpus luteum does not form
No ovarian progesterone production
↑ Estrogen to progesterone ratio
Proliferative effect of estrogen unopposed
Endometrial proliferation
No progesterone to organize growing endometrium
Disorganized endometrium overgrows and sloughs off
Irregular bleeding
Menopause
Premature ovarian insufficiency
Intermittent congestion of polyp blood supply
Transient ischemia and slight polyp necrosis
Altered growth factor production
Vascular dysregulation and leakier vessels
Coagulopathies (e.g. von Willebrand disease)
Impaired hemostasis
Invasion of normal tissue
↓ Estrogen (hypoestrogenism)
Atrophy of endometrium and vulvovaginal tissue
Dry endometrial surfaces (↓ fluid to prevent friction)
Endometrial carcinoma
Micro- erosions of epithelium
Inflammation
Evidence unclear
Heavier and more irregular bleeding
Spotting
Heavier and more irregular bleeding
Light bleeding and spotting
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 2, 2022 on www.thecalgaryguide.com")
epithelial-ovarian-cancer-subtypes-molecular-alterations-risk-factors
 Mucinous carcinoma
Ovarian endometriosis (implantation of endometrial tissue on the ovaries)
↑ Chance of endometrioma (cyst comprised of endometrial tissue) formation in ovaries
See Endometriosis Slide
Familial BRCA1 or BRCA2 mutation
Impaired double strand DNA repair mechanism results in accumulation of DNA damage
5) High grade serous carcinoma
Lynch syndrome (autosomal dominant mutations in DNA repair genes)
Impaired DNA mismatch repair
mechanismà accumulation of DNA damage
1) Low grade serous carcinoma
3) Clear cell carcinoma
4) Endometrioid carcinoma
Either clear cell, endometrioid carcinomas, or a mix of both subtypes
General risk factors for developing all epithelial ovarian cancer (unknown pathogenesis)
1. Old age
2. Family history of breast or ovarian cancer
3. Post-menopausal hormone replacement therapy
4. Irregular age of menarche & menopause 5. High number of lifetime ovulation events /
nulliparity
Alteration in genes like KRAS, NRAS, BRAF, ERBB2 & CDKN2A
Alteration in genes like ARID1A, PIK3CA & ERBB2
Alteration in genes like POLE & TP53
Molecular alterations in genes like TP53 and/or CCNE1
Molecular alterations commonly associated with specific epithelial ovarian cancer subtypes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Findings
Complications
Published August 30, 2022 on www.thecalgaryguide.com")
Menopause
 See relevant slide: Menstrual Cycle Physiology: Ovarian Cycle – Brief Overview
Each cycle involves ovulation, during which an oocyte is released from the ovary’s dominant follicle into the Fallopian tube
Some non-dominant follicles degenerate in a process known as atresia
Menstrual cycle stops
Menopause marks 1 year since last menstrual cycle
↓ Fluid transudatio
n from blood vessels of vaginal wall
↓ Vaginal lubrication
Vaginal tissue becomes thinner and more easily irritated
Over time, fewer
follicles remain in the ovary
Some cycles become anovulatory (no oocyte is released from ovary)
↓ Ovulation causes prevents thickening of the endometrial lining
↓ regularity and frequency of periods
Ovaries eventually stop releasing oocytes
↑ Oxidative stress- induced apoptosis of dermal fibroblasts
Remaining non-dominant follicles become less sensitive to LH and FSH
Since follicular cells are responsible for estrogen production, less follicles result in reduced estrogen production
↓ Expression of serotonin receptors in the CNS
↓ LDL receptor expression and ↑HMG- CoA reductase activity
↓ Regulation of the production and clearance of LDL
↑ LDL Cholesterol levels
Author: Sunawer Aujla Reviewers: Ashar Memon Yan Yu* * MD at time of publication
↓ Serotonin activity
↓ Density of
↓ Healthy vaginal flora
↑ pH of vaginal fluid
↑ Spread of bacteria otherwise unable to survive in low pH environment
Recurrent urinary tract infections
↓ Calcitonin
↑ Sensitivity of bone mass to Parathyroid Hormone
↑ Activation of osteoclasts
Mechanism is likely
multifactorial and the subjective symptoms of menopause may contribute
Depression
5HT receptors in
thermoregulatory region of hypothalamus
↑ Inhibition of sexual responses initiated in prefrontal cortex
↓ Libido
2A
↓ Collagen, elastin, and hyaluronic acid
↓ Proliferation of smooth muscle fibers
↓ Inhibition of osteoclasts
Narrower thermoregulatory zone
Injury to epithelial tissue in multiple areas of the body
Atrophy of bladder and urethra epithelium
Urinary incontinence
More bone resorption than formation
Osteoporosis
See relevant slide: Osteoporosis: Pathogenesis and risk factors
Sometimes, for unknown reasons, core body temperature increases above upper threshold of narrowed thermoregulatory zone
Hot Flashes
Sudden, temporary onset of body warmth, flushing, and sweating
Sometimes, for unknown reasons, core body temperature decreases below lower threshold of narrowed thermoregulatory zone
Chills
Sudden, temporary onset of shivering, tingling, cold feeling
Atrophy of vaginal epithelium
Dyspareunia
Pain during sexual intercourse
↓ Integrity of of blood vessels
Atherosclerosis
↑ Risk for cardiovascular disease
Genitourinary Syndrome of Menopause
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 7, 2023 on www.thecalgaryguide.com")
Cystocele

Connective tissue disorders (e.g. Marfans, Ehlers- Danlos Syndrome)
Genetic susceptibility (e.g. Type III collagen gene abnormality
Menopause
Visceral fat places pressure on pelvic floor structures
Growing fetus places pressure on pelvic floor structures
Straining and bearing down on pelvic floor
Muscle tearing and damage
Disruption of nerves, loss of bladder structural support, and disruption of fascia and muscles
Collagen impairment
Depletion of ovarian follicles leading to ↓ in estrogen production
↑ Intra-abdominal pressure
Transfer of intra- abdominal pressure to pelvic floor
Pelvic floor muscles and pelvic floor fascia become weakened
Pelvic tissue and muscular atrophy
Loss of tissue function and structure support that collagen provided
↓ Stimulation of collagen production
↓ Estrogen levels
Pelvic Organ Prolapse Quantification (POP-Q) System: Grade 1: Bladder descends 1 cm above the hymen Grade 2: Bladder descends to ≤ 1 cm above or below hymen
Grade 3: Bladder descends past the hymen but 2 cm less than total vaginal length
Grade 4: Complete vaginal prolapse
Mechanical obstruction of bladder and urethra
Urinary retention
Descended bladder creates pressure in vagina
Pressure/bulging sensation
Symptoms of voiding dysfunction (e.g. incomplete emptying/frequency/ urgency/nocturia)
Vaginal intercourse puts pressure on descended bladder
Activates pain receptors
Dyspareunia (painful sex) for some patients
Cystocele
Descent of bladder through anterior vaginal wall
Hydronephrosis/ hydroureter
Recurrent UTI
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 5, 2024 on www.thecalgaryguide.com")
Ankle Fracture

Crushing force (e.g. limb Loading force entrapment beneath heavy object) (e.g. fall)
Force exceeds mechanical strength of bone
Ankle eversion or inversion
Osteoporosis
Compromised bone scaffolding & repair impairs the structural integrity of bone. Force required for fracture is lowered
Ankle Fracture
(Fracture of the talus and/or the distal 6 cm of the tibia and/or fibula)
Fractured bone is displaced through the dermal layers
Open Fracture
Compromised dermal layers create an opportunity for pathogens to enter the wound site
Infection
Multiple malleoli are fractured within the ring of the ankle
Lack of ligamentous & bone support makes ankle joint unstable
Displacement of bone from fracture site
Misalignment of bone segments prevents regeneration & union
Malunion of unreduced fracture
Ligamentous injury occurs concurrently from excessive tensile force
Fractured bone disrupts surrounding vasculature
Hyaline cartilage of the articulating surface is damaged
Trauma induces synovitis, chondrocyte apoptosis, & necrosis
Fractured bone disrupts surrounding peripheral nerves
Numbness Localized Pain
Pain is induced when the patient attempts to weight bear
Inability to weight bear
Authors: Ethan Smith Reviewers: Nojan Mannani Michelle J. Chen Dr. Gerhard Kiefer* * MD at time of publication
Platelets are exposed to the extravascular environment, thereby releasing platelet derived factors & complement factors
Plasma coagulation cascade is activated
Chondrocyte dysfunction in proliferation
Reduced synovial functioning
↑Vascular permeability from inflammatory cytokines
Protective hematoma forms in the joint space
Hyaline cartilage loss
Lost cartilage over time degrades proper articulation & causes joint narrowing, osteophytes, subchondral sclerosis
Post traumatic osteoarthritis
Edema
Fluid in the joint space changes position of bony articulations
Bruising
Restricted range of movement
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 30, 2024 on www.thecalgaryguide.com")
Genital Prolapse

↑ risk of levator
muscle avulsion
Pelvis widens during
Valsalva maneuver
(straining downwards
to ↑ intra-abdominal
pressure)
↑ Support needed
to hold pelvic
organs, which may
eventually fail
Genital Prolapse: Pathogenesis, clinical findings, & complications
Pregnancy
Levator ani muscle is injured or
denervated due to overstretching
& or compression during labour
Levator ani muscle loses tone
Genital hiatus opening enlarges
Pelvic diaphragm descends
& forms a funnel shape
Ligamentous & connective tissue (e.g., arcus tendineus
fascia pelvis, arcus tendineus levator ani, uterosacral
ligaments) bear the ↑ abdominal pressure load
Ligamentous & connective
tissue stretch & may
eventually fail with time
↑ Internal pressure from pelvic organ
tissues pushes against pelvic muscles Hysterectomy
Disruption to pelvic
structural supports
(particularly uterosacral
ligament), pelvic blood
supply, & or innervation
during operation
↓ Pelvic organ support,
which may fail with time
Authors:
Sara Cho
Reviewers:
Michelle J. Chen
Jessica Revington
Rachel Wang*
* MD at time of publication
Unclear mechanism
Pelvic & or low back pain Dyspareunia (pain during intercourse)
Legend: Pathophysiology Mechanism
Conditions with impaired
collagen quality (e.g.
Ehlers-Danlos syndrome,
Marfan syndrome)
Alterations in collagen
& elastin synthesis
Dysfunction of pelvic
connective tissue
Aging/menopause
↓ Systemic
estrogen
concentrations
↓ Smooth muscle cell
proliferation & collagen
synthesis in tissues
with estrogen
receptors (e.g.,
endopelvic fascia, arcus
tendineus, levator ani,
uterosacral ligament)
Chronic cough
Frequent
contraction of
abdominal &
pelvic muscles
Chronic
constipation
Patient constantly
bears down,
contracting
abdominal &
pelvic muscles
Genetic factors
(e.g., family
history of
prolapse, urinary
incontinence,
abdominal or
inguinal hernia)
Obesity
Surrounding
adipose tissue ↑
intra-abdominal
pressure
↑ Stress on pelvic
supporting structures
Repeated ↑ in intra-
abdominal pressure
Combination of risk factors that contribute to,
predispose, promote, or worsen prolapse
Sign/Symptom/Lab Finding ↓ Pelvic organ support,
which may fail with time
Genital Prolapse
Vaginal or uterine descent through the introitus (genital opening)
Rectum pushes against the vaginal wall & widens the
anorectal angle (angle between anal canal & rectum)
Fecal incontinence
Published Aug 25, 2025 on www.thecalgaryguide.com
Weakened pelvic floor muscles provide
↓ structural support & ↑ hypermobility
of the urethra & bladder neck
Urinary incontinence
Complications")
Endometriosis

Transfer of endometrial tissue away
from the uterus during pelvic surgery,
vaginal delivery, or cesarean section
Sampson’s theory: Retrograde
flow of endometrial tissue
through fallopian tubes
Long menstrual flows
(↑ retrograde menstruation)
Coelomic metaplasia theory:
Undifferentiated mesothelial cells
from the peritoneal cavity
differentiate into endometrial cells
during fetal development. May also
occur in patients with testes
Implantation theory: Menstrual endometrium
implants onto pelvic structures
↓ Cellular antioxidant
capacity (↑ cell damage)
Alcohol use
(mechanism unclear)
Early menarche (↑
estrogen exposure)
Stem cell theory: Endometrial stem/
Embryonic rest theory: Residual
progenitor cells from menstrual
embryonic cells from Müllerian
Dissemination theory: Endometrial
blood or neonatal uterine bleeding
or Wolffian ducts are misplaced
tissue transported through bloodstream
implant in the pelvic cavity
during organogenesis
or lymphatics to extrauterine structures
(e.g., brain, pericardium)
Cells differentiate into endometrial-like tissue
Ovary releases estrogen
& progesterone
Endometriosis
Endometrial glands & stroma (structural support tissue) found outside the uterus
Ectopic endometrial-like
tissue on bladder
Ectopic endometrial-like tissue in posterior cul-de-sac
Monthly proliferation
(by estrogen) and
stabilization (by
progesterone) of
endometrial tissue
Chronic inflammation of surrounding tissues & fibrosis/adhesion formation
Tissue inflammation & fibrosis/adhesions push on & displace pelvic organs
Ectopic tissue
abnormally
activates
nerve signaling
pathways
responsible for
bladder
contraction
Bladder wall
contractions
activate
nociceptors
(pain
sensors)
Penetrative intercourse involving the
posterior vagina applies ↑ pressure to
tethered & immobile pelvic structures
Feces moves down colon into
rectum & applies pressure to
the tethered rectum
Monthly
progesterone
withdrawal
Dyspareunia (pain with
deep intercourse)
Dyschezia (pain with
bowel movements)
↑ Urinary
frequency &
urgency
Pain with
micturition
(urination)
Endometrial tissue sloughs
off from a basal tissue layer
(menstruation**)
Extra-uterine endometrial-
like tissue cannot evacuate
the implantation site
Retrograde menstruation in ovary ↑ the
presence of ectopic endometrial-like tissue
& blood (mechanism poorly understood)
Old blood fills
endometrial-like
tissue on ovary
Endometrioma
(chocolate cyst)
Chronic cyclical local
inflammation (release of
pro-inflammatory chemicals)
Nociceptors near ectopic
endometrial-like tissue activate
Pain signals & release of inflammatory
mediators subsides over time
Cyclic dysmenorrhea
(menstrual pain)
Repair of inflammation
Ectopic endometrial-like tissue
becomes fibrotic (scarred)
Significant ↑ scar tissue
Nodule formation
↓ Hormone levels
post-menopause
Accumulation of
inflammatory fluid
within scar tissue
↑ Risk of scar tissue obstructing
or kinking fallopian tubes
Endometrial tissue
stops proliferating
Hormone-dependent symptoms
(e.g., dysmenorrhea) cease
Cyst formation
Embryos unable to pass through
fallopian tube to uterus
Author:
Joshua Seto
Kayla Nelson
Reviewers:
Yan Yu
Sean Spence
Jessica Revington
Infertility
Colin Birch*, Rachel Wang*
* MD at time of publication
**See corresponding Calgary Guide slide
Legend: Published December 20, 2013, revised September 24,
2025 on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications")