SEARCH RESULTS FOR: asthma
Asthma: Findings on Investigations
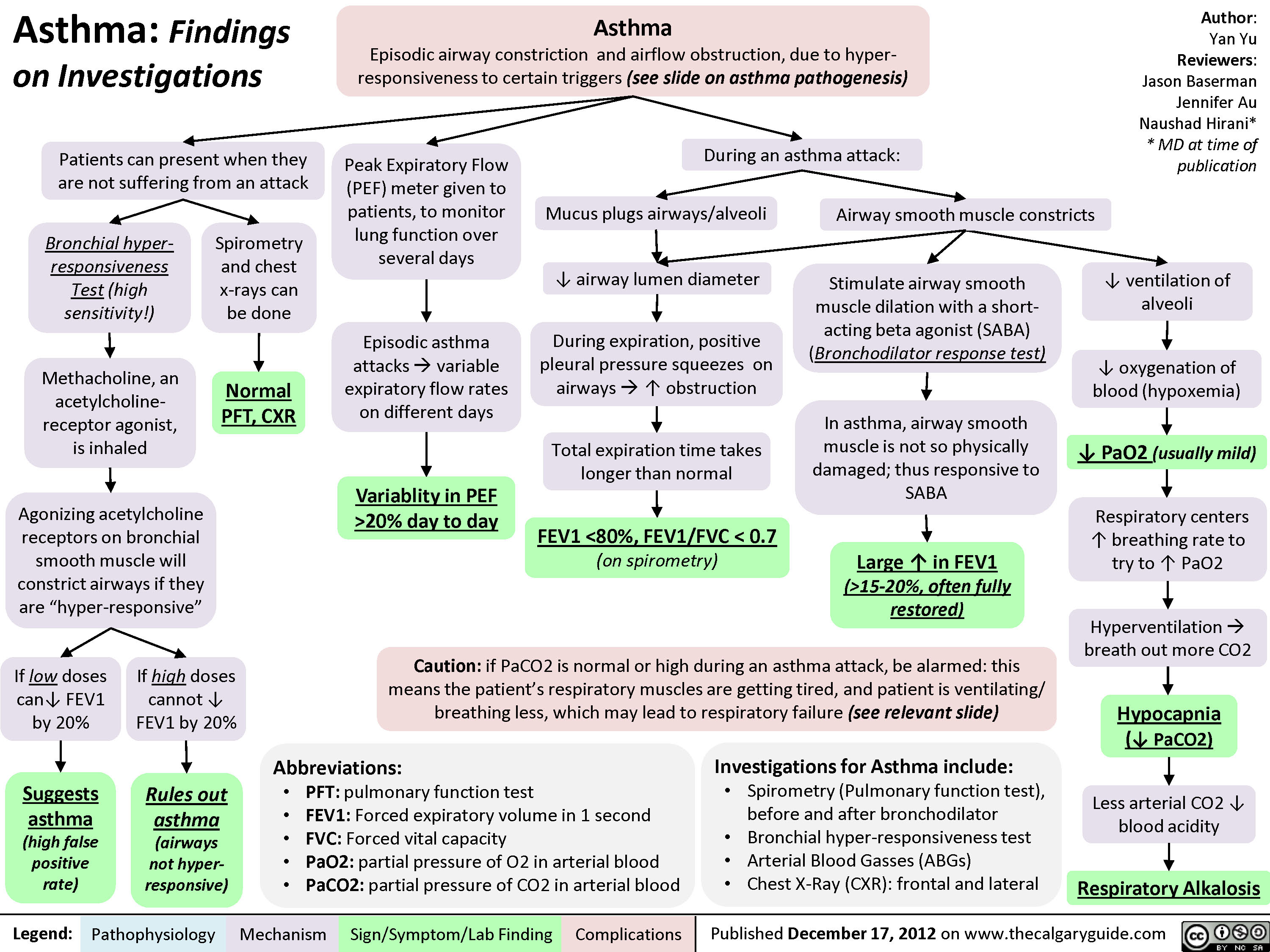
Asthma Acute Exacerbation: Pathogenesis and Treatment
: An episode of increased symptoms due to decreases in airflow
Abbreviations • PCO2: Partial pressure of CO, in arterial blood • PEF: Peak expiratory flow • SABA: Short-acting beta-2 agonists • Sp02 : Blood oxygen saturation level
Mild to moderate exacerbation: PEF 50% of predicted
Titrate O2 toSpO2, 92%, give SABA & steroids ■
Good response: symptoms resolved, PEF > 80%
[Treat at home with SABA as needed and steroids
Dyspnea
Bronchoconstriction
1` Residual volume and 1` PCO2
Respiratory failure
1` Air trapping causes '1' intra-alveolar pressure
Severe exacerbation: PEF 50% of predicted Educate patient regarding medications, Loss of Pulsus inhaler technique & [consciousness paradoxus follow up with primary care provider I
Legend: Pathophysiology Mechanism
Titrate O2 to402 93%, give SABA, steroids & magnesium sulfate
Sign/Symptom/Lab Finding
{Worsening symptoms and/or respiratory failure: Do not delay intubation, send to ICU, give SABA, steroids & magnesium sulfate
Authors: Luke Gagnon Reviewers: Midas (Kening) Kang Usama Malik Lian Szabo* * MD at time of publication
4, Delivery of oxygen rich air to alveoli 4, Oxygenation of blood
Drowsy and confused
Central cyanosis
• Tachycardia
Pneumothorax
[Depending on 1 severity: Observation or place chest tube")
Benzodiazepine (BZD) withdrawal: clinical findings and complications
 withdrawal: clinical findings and complications
Abrupt cessation of chronic ingestion of BZDs
Administration of BZD antagonist (flumazenil) on patients who have developed -* tolerance/dependence to BZD
Withdrawal Seizure
Negative physiological reactions BZD intake inhibition a mygd to f, • of a la Withdrawal symptoms Benzodiazepine Withdrawal GABA receptor activity (less inhibition alleviated by ingesting BZD Tolerance GABA BZD intake Conformational changes in the GABA receptor 1, receptor's Withdrawal Insomnia Pro-excitatory 4— state of excitatory neurotransmitters) 4— to the agent activity affinity for the agent
A
Activation of ACC and OFC
Feelings of fear
Activation of PAG
Behavioural response of fight or flight
Legend: Pathophysiology Mechanism
Activation of hypothalamus '1` Cortisol CAD, T2DM, Stroke
Sign/Symptom/Lab Finding
Activation of PBN
V
t RR, SOB, Asthma, or a sense of being smothered
Activation of LC
t Sympathetic Activity
t BP, t HR variability, tremor, and diaphoresis
Authors: Usama Malik Reviewers: Sina Marzoughi Aaron Mackie* * MD at time of publication
Notes: • The onset of withdrawal can vary according to the half-life of the BZD involved. Symptoms may be delayed up to three weeks in BZDs with long half-lives, but may appear as early as 24 to 48 hours after cessation of BZDs with short half-lives.
Abbreviations: • ACC: Anterior Cingulate Cortex • BP: Blood Pressure • CAD: Coronary Artery Disease • HR: Heart Rate • LC: Locus Coeruleus • MI: Myocardial Infarction • OFC: Orbitofrontal Cortex • PAG: Periaqueductal Gray • PBN: Parabrachial Nucleus • RR: Respiratory Rate • SOB: Shortness of Breath • T2DM: Type 2 Diabetes
I` atherosclerosis, cardiac ischemia, MI, or sudden death")
gastroesophageal-reflux-disease-gerd-complications
: Complications
Esophageal stricture
disease
Esophagitis
Esophageal
adenocarcinoma
Barrett’s esophagus
GERD
Reflux of gastric content into distal esophagus
Damage to squamous
esophageal epithelium
Legend: Published March 30, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Authors:
Wendy Wang
Reviewers:
Yoyo Chan
Sean Doherty
Dr. Sylvain Coderre*
* MD at time of publication
Squamous esophageal
epithelium undergoes
metaplasia to become
columnar epithelium
This predisposes cells to
premalignant changes
(dysplasia)
Collagen is deposited
where ulcers heal
Asthma/Chronic Cough
Chronic Laryngitis
Laryngeal and
Tracheal Stenosis
Extra-esophageal Complications Esophageal Complications
Airway becomes
irritated
Fibroblasts proliferate
and deposit granulation
tissue in airway
Tissue deposition
leads to narrowing of
laryngeal and
tracheal space
Damage to pharyngeal
lining and airway
Esophageal tissue repeatedly
exposed to stomach acid
Pro-inflammatory cells and cytokines
are recruited to the area
Definitions:
• Metaplasia: abnormal change in the
nature of a tissue
• Pro-inflammatory cells and cytokines:
Mediators of inflammation. Examples
of cells include macrophages and T
cells, cytokines include IL-17, IL-2, IL-4
Over time, collagen fibers
contract
Bronchoconstriction
↑ vagal
tone
↑ bronchial
reactivity
Cough sensory
nerve endings are
stimulated
Vagal reflex
is activated
Activation of
cough center in
brainstem
↑ inflammation of
squamous epithelium
Ulcers form in esophagus")
Beta-Blockers-Mechanism-of-Action-and-Side-Effects
 to these receptors, ↓ their normal adrenergic tone
Beta-2 receptor antagonism Beta-1 receptor antagonism
Lungs Eyes Central nervous system Heart Kidneys ↓ cAMP (intracellular messenger) productionàcomplex, tissue-specific intracellular mechanisms resulting in a variety of effects in different tissues:
Throughout body tissue
Epinephrine (via cAMP) indirectly ↑ the activity of the Na+/K+ pump on cell membranes (a pump that moves 3 Na+ out of cells per 2 K+ moved into cells)
Blocking epinephrine from binding
the beta-2 receptor and producing cAMPà↓ activity of Na+/K+ pump à↓K+ moved into cells
↑ proportion of K+ now resides in extracellular fluid, detectable in serum (total body K+ remains the same)
Hyperkalemia (see Calgary Guide: Hyperkalemia – Clinical findings)
Blocking sympathetic hormonesà↓ relaxation of smooth muscle circumferentially wrapped around airways
↑ resting airway muscle toneà bronchoconstriction
↑ resistance to airflow
Wheezing, dyspnea, chest tightness
Exacerbation of underlying airway disease (e.g. asthma)
↓ ciliary epithelium’s production of aqueous humor (fluid that fills anterior chamber of the eye)
Reduced intraocular pressure
Blocking adrenergic response mediated by epinephrine and norepinephrine (e.g. the physiologic “fight- or-flight” response to stress)
↓ tremor, irritability, anxiety
↓ ability to produce adrenergic symptoms in response to hypoglycemia
Hypoglycemia unawareness
Coronary perfusion pressure = diastolic blood pressure in aorta – LV end diastolic pressure
↓ inotropy (contractility of cardiac muscle)
↓ chronotropy (heart rate and conduction velocity)
↓ renin releaseà↓ creation of angiotensin II & aldosterone
+ ↓ reabsorption of Na
and H2O in nephron
↑ urinary Na+ & H2O loss
↓ total blood volume
Decompensation of acute heart failure
Dizziness and fatigue Hypotension (Blood pressure = cardiac
output x systemic vascular resistance)
↓ O2 demand of myocardial tissue
Bradycardia
Inability to ↑ heart rate in response to stress (e.g. shock, sepsis)
↓ stroke volume
↓ cardiac output
Beta blockers ↓ diastolic blood pressure, & thus may ↓ coronary perfusion pressure
Before giving beta blockers, ensure blood pressure isn’t too low
Otherwise, may worsen acute myocardial ischemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 14, 2021, updated Feb 7, 2021 on www.thecalgaryguide.com")
asthma-pathogenesis
 Naushad Hirani* * MD at time of publication
Genetic factors
(i.e. HLA gene mutations, defects in bronchial airway epithelium)
Environmental factors
(i.e. excess hygiene, fewer siblings, antibiotics within the first two years)
Asthma:
Defined as airway hyper-responsiveness causing variable and reversible airflow obstruction
Atopy:
predisposition to allergic hyper-sensitivity in airways
First exposure to triggers*
sensitizes helper T cells
Stimulation of B-cells to produce IgE, which binds to mast cell surfaces
Activated Helper-T cells & IgE-sensitized mast cells now line the airways
Triggers of airway hyper- responsiveness include:
Upper respiratory tract infections (URTIs)
Allergens (pollen, animal dander, dust, mold, etc)
Air pollution, cigarette smoke, other chemicals
Drugs (aspirin, NSAIDs, Beta- blockers)
Cold air
Exercise
Early response (0-2 hrs)
Delayed response (3-4 hrs)
Allergens cross-link IgEs on mast cells
Activated mast cells & helper T cells release cytokines
Mast cells release histamines, leukotrienes, and other inflammatory mediators
Induce maturation of granular WBCs like eosinophils
Eosinophils migrate into:
Vascular permeabilityà edema of airway mucosa
Goblet cell hyperplasia à mucus secretion
Bronchial smooth muscle contraction
Airway obstruction
Second exposure to triggers
Asthma Airways Bronchiole constriction
Eyes Conjunctivitis Nose Rhinitis
Note: Delayed response presents within 3-4 hrs, peaks within 6-8 hrs, and resolves within 24 hrs
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 17, 2012, updated Aug 19, 2021 on www.thecalgaryguide.com")
copd-overview-and-definitions
”
Author: Yan Yu Reviewers: Jason Baserman, Jennifer Au, Ciara Hanly, Zesheng Ye (叶泽生), Yonglin Mai (麦泳琳)*, Naushad Hirani*, Juri Janovcik* * MD at time of publication
Cystic Fibrosis
Multisystem disease due to CFTR gene mutation, that presents in the lungs as bronchiectasis
Bronchiectasis, Cystic Fibrosis, etc
COPD
Systemic disease, largely manifesting as an airflow-obstructing respiratory disorder; can manifest in the form of any of the following disorders:
Emphysema
Lung tissue destruction & abnormal, permanent enlargement of lung acini: airspaces distal to terminal bronchioles
Chronic Bronchitis
Chronic, productive cough for a total duration of 3 months per year, over 2 continuous years
Asthma
Asthma that does not
remit completely with treatment (thus, chronic airflow obstruction) is defined as asthma-COPD overlap syndrome (ACOS)
Emphysema
Bronchiectasis
Destruction and widening of large airways, resulting in mucus hyper-secretion and recurrent infections
Chronic Bronchitis
Most common COPD manifestations
(most patients suffer from a combination of emphysema and chronic bronchitis)
Clinically, COPD is seen as:
• Progressive, partially reversible airflow obstruction and lung hyperinflation (causing respiratory symptoms like cough, sputum production, and dyspnea)
• Post-bronchodilator spirometry results: FEV1/FVC ratio <0.7 (FEV1 is not a defining feature of COPD, but a marker of severity)
• ↑ frequency & severity of acute exacerbations
• Systemic manifestations such as
deconditioning and muscle weakness
Chronic Obstructive Pulmonary Disease (COPD)
Asthma
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013, updated October 5, 2021 on www.thecalgaryguide.com")
Pneumonie: Pathogenese und klinische Befunde
 und kann unterteilt werden in: Ambulant erworbene, nosokomial (im Krankenhaus) erworbene Pneumonie
Die Immunantwort variiert je nach eingedrungenem Erreger (z.B. Pneumokokken verursachen ein lobär betontes,
H. influenzae ein interstitiell betontes Entzündungsbild)
Rauchen unterdrückt die Funktionsfähigkeit der neutrophilen Granulozyten und schädigt das Lungenepithel
Chronische Lungenerkrankungen z.B. COPD, Asthma oder Lungenkrebs zerstören das Lungengewebe und bieten Krankheitserregern mehr Angriffsfläche für Infektionen
Durch Immunsuppression z.B. bei HIV, Sepsis, Glucocorticoid- oder Chemotherapie wird die Immunantwort eingeschränkt
Systemisch kommt es zu einer inflammatorischen Immunantwort
Durch systemische Zytokinfreisetzung wird die
hypothalamische Thermoregulation beeinträchtigt
Erregersexposition durch Inhalation, Aspiration, Kontakt- oder hämatologische Übertragung
Anfällige Person und/oder virulenter Erreger
Proliferation des Erregers in unteren Atemwegen und Alveolen
Lokal reagiert das Alveolarepithel mit einer Chemokinausschüttung um neutrophile Granulozyten an den Entzündungsort zu mobilisieren
LOBÄR betont: Lokal begrenzte Akkumulation von neutrophilen Granulozyten und Plasmaexudat in Alveolen
INTERSTITIELL betont: Zelluläre Infiltrate (Immunzellen und Immunzellfragmente) in den Alveolarwänden (zwischen Alveolen und Kapillaren)
Fieber
Anmerkungen:
Schüttelfrost
Irritation der Atemwege mit Hustenreiz
Flüssige Infiltrate in Alveolen führen zur Schleimbildung
Produktiver Husten
Das Exudat vermindert die
Röntgenstrahlendur chlässigkeit, entzündete Areale erscheinen im Röntgenbild heller/weiß.
Verschattung im Röntgen
Alveolen sind durch Flüssigkeitsansamml ungen blockiert
Verdickung der Alveolarwände, Diffusionsstrecke ↑
Irritation der Alveolarwände mit Hustenreiz
Bei ausschließlich interstitieller Infiltration -> Husten ohne Schleimproduktion
Trockener Husten
• Andere Symptome der Pneumonie sind: Brustschmerzen, Nutzung der Atemhilfsmuskulatur, auskultatorisch Rasselgeräusche, Müdigkeit
• Diese Symptome sind jedoch unspezifisch
O2 und CO2- Austausch vermindert
Hypoxie
Periphere & zentrale Chemorezeptoren werden aktiviert, Atemfrequenz ↑
Luftnot
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Veröffentlicht: 26. September 2016 auf www.thecalgaryguide.com")
Asthma: Pathogenese
 Naushad Hirani* Übersetzung: Sarah Schwarz Übersetzungsprüfung: Dr. Gesche Tallen * MD zum Zeitpunkt der Veröffentlichung
Genetische Faktoren
(z.B. Mutationen im HLA- Gen, Defekte im bronchialen Endothel)
Umwelteinflüsse
(z.B. übermäßige Hygiene, wenige Geschwister, Antibiotikaeinnahme in den ersten 2 Lj.)
Asthma:
Eine chronisch-entzündliche Erkrankung welche durch hyperreagible Atemwege zu variablen, reversiblen Obstruktionen führt
Trigger für Hyperreagibilität der Atemwege:
Atopie:
Neigung zu allergischen Überempfindlichkeitsreaktionen der Atemwege
Erstexposition gegenüber des Triggers
Sensibilisierung der T-Helferzellen
Stimulation der B-Zellen zur IgE Produktion, welche an Mastzellen binden und diese aktivieren
Aktivierte T-Helferzellen und Mastzellen säumen die Atemwege
Infektionen des oberen Respirationstrakts
Allergene (Pollen, Haus- staub, Tierhaar etc.)
Luftverschmutzung, Zigarettenrauch, Chemikalien
Medikamente (ASS, NSAR, Beta-Blocker)
kalte Luft
Bewegung
Mastzellen setzen Histamine, Leukotriene
und andere Entzündungsmediatoren frei
Induzieren Zellreifung eosinophiler Granulozyten
Eosinophile migrieren in:
Gefäßpermeabilität ↑, Schleimhautödem in Bronchien
Becherzellhyperplasie, Schleimsekretion ↑
Kontraktion der Bronchialmuskulatur
Zweitkontak t mit dem Trigger
Frühe Reaktion (0-2 h)
Verspätet e Reaktion (3-4 h)
Allergene binden an IgEs auf Mastzellen
Aktivierte T- Helferzellen & Mastzellen setzen Zytokine frei
Obstruktion der Atemwege
Asthma
Bronchokonstriktion Konjunktivitis
Beachte: Verspätete Reaktionen beginnen nach 3-4h, erreichen ihren Höhepunkt nach 6-8h und klingen nach 24h ab
Atemwege Augen
Nase
Rhinitis
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Veröffentlicht: 17. Dez. 2012, aktualisiert: 19. Aug. 2021 auf www.thecalgaryguide.com")
哮喘急性发作-发病机制和治疗
 Kang,Usama Malik,Lian Szabo*
译者:Yonglin Mai (麦泳琳) 翻译审核人:Zesheng Ye (叶泽生) * 发表时担任临床医生
下呼吸道炎症
免疫系统激活:气道上皮趋化因子、淋巴细胞和巨噬细胞激活, 白三烯产生↑ 炎症介质释放
哮喘轻中度急性发作: PEF ≥ 预计值50%
疗效良好: 症状缓 解, PEF ≥ 80%
患者日常在家 服用糖皮质激 素及必要时使 用SABA
支气管狭窄
残气量↑ 及PaCO2↑
气体潴留↑,肺 泡内压力 ↑
奇脉
气体通过 发炎的呼 吸道产生 的刺激↑
咳嗽和喘息
Notes
呼吸 困难
黏膜水肿会导 致气流湍急
喘息
吸O2使SpO2 ≥ 92%, 给予SABA & 糖皮质激素 治疗
重度急性发作: PEF ≤预计值 50%
呼吸困难
呼吸急促 呼吸衰竭
意识丧失
↓ 向肺泡传送 空气氧含量
血氧饱和度↓
•
•
Asthma哮喘: Airway hyper- responsiveness causing airflow obstructions气道高反应性引起气流受 限
Acute Exacerbation (Asthma)哮喘急性 发作: An episode of increased symptoms due to decreases in airflow气流减少而 引起一系列症状加重
Abbreviations
• PaCO2动脉二氧化碳分压:Partial
pressure of CO2 in arterial blood
• PEF最大呼气流量/呼气流量峰值: Peak
expiratory flow
• SABA短效beta-2受体激动剂: Short-
acting beta-2 agonists
• SpO2血氧饱和度: Blood oxygen
saturation level
昏睡
气胸
中枢性紫绀 心动过速
患者宣教: 正确服用药物,使用 药物吸入装置 &全科医生密切医学随 访
吸 O 使 SpO ≥ 2 2
症状恶化和/或呼吸衰竭 :及时气 管插管, 送往ICU, 给予SABA, 糖皮 质激素 & 硫酸镁
取决于气胸严 重程度: 密切观 察或者置入胸 腔引流管
93%, 给予 SABA, 糖皮质激素 & 硫 酸镁
图注:
病理生理
机制
体征/症状/实验室检查
并发症
2018年 2月6日发布于 www.thecalgaryguide.com")
Asthma clinical findings

Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Yonoglin Mai (麦泳琳) Naushad Hirani* * MD at time of publication
Variable, sporadic airway obstruction in response to triggers
Associated allergic eosinophil response
Eosinophils infiltrate: Skin
If severe:
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
During expiration, positive pleural pressure squeezes on airwaysà↑↑ airway obstruction
Heart rate to improve
perfusion of tissue
Tachycardia
Respiratory centers rate of breathing to
compensate
Tachypnea
Gas is trapped within alveolià hyperinflates lungs
Ventilating larger lungs needs more effort
Patients need to voluntarily contract
their expiratory muscles faster and more forcefully to effectively expire
Narrower airways àturbulent
airflow, heard on auscultation
Expiratory Wheeze (high-pitched expiratory sound)
Nose
Rhinitis/ sinusitis
Runny nose, sneezing, etc
Atopic dermatitis
Skin rash, hives
Eyes
Conjunctivitis
Red itchy eyes, visual blurring
Episodic
dyspnea
(shortness of breath)
Chest tightness
During severe attacks:
Note: Asthma attacks often have two phases:
• An immediate attack (within 0-2 hours of the trigger, due to acute release of histamine from mast cells)
• A delayed attack (due to eosinophil infiltration of airways, presents within 3-4 hours after exposure to the trigger, peaks within 6-8 hours, and resolves within 24 hours).
Keep the possibility of a delayed attack in mind when treating patients in Emergency!
Note: Symptoms often worse at night or early in the morning.
Note: Asthma should be suspected in children experiencing dyspnea with multiple episodes of Upper Respiratory Tract Infections or Croup.
Patient compensates by activating accessory respiratory muscles to ↑ thoracic volume
Visible contraction of
neck muscles (Scalene, sternocleidomastoids)
↑↑↑ airway obstruction on
expiration, lungs take more time to empty
Prolonged expiratory phase of breathing
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 17, 2012 and updated Dec 4, 2021 on www.thecalgaryguide.com")
Chronic Cough Pathogenesis_2021

Infection
IP; likely chronic ↑ cough receptors commonly pertussis- related or post-viral
Asthma
↑ EDN
↑ MBP levels in RT
Neoplasm
Bronchiectasis
COPD
GERD
Allergic Rhinitis
↑ sputum production
and accumulation
Damage from chronic inflammation causes poor mucus clearance
Inhalants trigger ↑ cytokines ↑ mucus
Aspiration of refluxed microdroplets
Irritation by post- nasal drip
↑ inflammatory mediators in RT
Mechanical obstructions (i.e. mediastinal masses, neoplasms)
Foreign body Presence irritation of irritants
Stimulation of sensory nerve receptors expressed on nerve endings penetrating the epithelia of the upper RT
Abbreviations:
• RT: respiratory tract
• IP: indefinite
pathophysiology
• GERD: Gastro-esophageal
reflux disease
• EDN: Eosinophil-derived
neurotoxin
• MBP: Major basic protein
• COPD: Chronic
Obstructive Pulmonary Disease
Complications: Syncope, insomnia, hemoptysis, rib fractures
Slowly adapting receptors
Respond to mechanical forces during breathing
Stimulation of the vagus nerve
Activation of nucleus tractus solitarius in central respiratory generator (brainstem)
Generation of efferent cough signal
Chronic cough: Cough of over 8 weeks duration with no dyspnea or fever
C-fibre receptors
Respond to chemical stimuli (bradykinin, capsaicin, acid/alkaline solutions, mannitol, hypertonic saline, and other inhaled irritants)
Authors: Arsalan Ahmad Lance Bartel Reviewers: Midas (Kening) Kang Usama Malik Ciara Hanly Yonglin Mai (麦泳琳) Yan Yu*, Eric Leung* * MD at time of publication
Rapidly adapting receptors
Responds to mechanical stimuli, such as physical obstruction of the airways
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 06, 2018, updated Dec 4, 2021 on www.thecalgaryguide.com")
哮喘-发病机制

哮喘-临床表现

哮喘-检查结果

adult-pneumonia-pathogenesis-and-clinical-findings
 and can be further classified by location of exposure: community, health- care, hospital acquired
Inflammatory response varies depending on type of invading pathogen (i.e. S. Pneumonia causes a lobar pattern and Influenza A & B cause an interstitial pattern)
LOBAR: Accumulation of neutrophils and plasma exudate from capillaries into alveoli specific to a lung area/lobe
INTERSTITIAL: Accumulation of infiltrates (i.e. inflamed cellular debris) in the alveolar walls (i.e. space between the alveolar spaces and bloodstream)
Fever
Notes:
• Other signs and symptoms
of pneumonia exist such as chest pain, accessory muscle use, crackles on auscultation and fatigue
• These signs and symptoms are less specific to the ones outlined on this slide
Irritation and attempted clearance of airways
Fluid infiltrates are inside alveoli, airway clearance leads to phlegm production
Productive Cough
Fluid build up does not allow X-rays to pass through à white opacity on plain film at site of fluid buildup
Consolidation on CXR
Alveolar sacs blocked by fluid accumulation
Thickening of alveolar walls ↑ diffusion distance between alveoli & capillaries
Irritated alveolar walls trigger cough reflex
Since fluid infiltrates are NOT in the alveoli, attempts to empty the alveoli through coughing doesn’t lead to production of fluid
Dry Cough
Chills/Rigors
↓ Exchange of CO2 and O2
Hypoxemia
Triggers peripheral and central chemoreceptors to ↑ respiratory drive
Dyspnea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 26 2016, updated Feb 9, 2022 on www.thecalgaryguide.com")
asthma-how-treatments-work-and-common-side-effects

Long-acting Beta Agonists (Controller)
Short-acting Muscarinic Antagonists (Exacerbation)
Long-acting Muscarinic Antagonists (Controller)
Magnesium Sulfate (Exacerbation)
Monoclonal Antibodies (Controller)
Leukotriene Receptor Antagonists (Controller)
Inhaled Corticosteroids (ICS) (Controller)
Systemic Corticosteroids (Exacerbation)
Binding to beta-2 adrenergic receptors and subsequent intracellular signal cascade in bronchial smooth muscle
Off-target binding occurs in other systemic cells
Inhibition of muscarinic acetylcholine receptors in airway muscle cells
↓ Activation of the inositol triphosphate (IP3)
intracellular pathway
(IP3 pathway normally functions to mobilize intracellular Ca2+ stores)
Inhibition of Ca2+ channels on airway smooth muscle surface
↓ Influx of Ca2+
Binding and inactivation of inflammatory signal molecules (IgE, IL-5)
Inhibition of leukotriene receptors in lung and immune cells
Steroid binds to nuclear receptors within cells
↓ Gene expression/synthesis of immune mediators (ex. cytokines)
Stimulation of
Na/K ATPase (which transports K into cells)
Hypokalemia Palpitations Tachycardia Muscle cramps Tremor
Authors: Chunpeng Nie Reviewers: Sravya Kakumanu, Ben Campbell, *Tara Lohmann
* MD at time of publication
↓ Activation of mast cells (by ↓ IgE) and eosinophils (by ↓ IL-5/leukotrienes)
↓ Release of inflammatory cytokines by these cells (↓ Type 2 inflammatory response in airways)
↓ Permeability of airway vasculature
↓ Microvascular leakage into airway
Inadvertent sympathetic nervous system activation
Bronchial smooth muscle cells have ↓ Ca2+ release from intracellular stores (i.e. from sarcoplasmic reticulum)
↓↓ Cytoplasmic Ca2+
Myosin (muscle protein) unable to be activated for muscle contraction
↓ Smooth muscle contraction in bronchioles
Bronchodilation
ICS cause ↓
immune cell activity in the oropharynx
Susceptibility to infection and irritation of the oropharynx from inhaled particles and pathogens
Hoarseness Thrush
Systemic corticosteroids cause ↓ immune cell activity in whole body
↑ Susceptibility to any infection
Many other side effects
Similar effects on other muscles in the body outside bronchi
Dry mouth
Urinary retention
Constipation
↓ Mucosal edema
↓ Airway Mucus
Airflow improvement
↑ Peak flow, ↑ Oxygenation, ↓ Dyspnea
Legend:
Pathophysiology
Mechanism
Treatment Effect
Complications
Published October 9, 2022 on www.thecalgaryguide.com")
Acute Laryngitis

Malaise Fever
Fungal
Atopy (asthma, allergy)
Non-infectious
Gastroesophageal Reflux
Trauma or damage to larynx
Smoking
Yan Yu*
* MD at time of publication
Environmental Pollution/Inhalants
Bacterial (S. pneumoniae,
H. influenzae, M. catarrhalis)
Systemic immune response
Spread of infection to larynx through upper respiratory tract
Infection of the vocal folds and surrounding tissue
Mechanical
(vocal misuse/ trauma)
(Area in the neck that contains the structures for voice production, anatomically anterior to the esophagus, inferior to the pharynx and superior to the trachea)
Irritation of the vocal folds and surrounding tissue
Inflammatory cascade triggered
Acute Laryngitis
Symptoms for <3 weeks
Acute injury to vocal folds
Vocal fold
lesions (i.e., vocal polyps)
Laryngeal inflammation
Neutrophils and macrophages release inflammatory cytokines
Local laryngeal inflammationà↑ vascular permeability ↑ Secretion of mucous leading to airway congestion Cough reflex initiated to clear airway congestion Cough
Edema of vocal folds and surrounding tissue
Dysphagia (difficulty swallowing)
Dysphonia (difficulty speaking)
Odynophagia (painful swallowing)
Swelling impairs vocal cord vibration
Frank aphonia (loss of voice)
Progressive worsening of edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 24, 2023 on www.thecalgaryguide.com")
Kindliche Asthma Exazerbation: Pathogenese und klinische Befunde bei Kindern

Asma Eksaserbasi Patogenesis dan temuan klinis pada anak

تشدید آسم حاد بیماریزایی و درمان

آسم بیماریزایی

آسم یافتھ ھای بالینی

آسم یافتھ ھای تحقیقاتی

Death Cardiovascular Respiratory and Neurologic Mechanisms

Hypoxemia (Type I Respiratory Failure): low dissolved oxygen in blood (PaO2)
Lungs can’t oxygenate blood fast enough
Lungs can’t rid blood of CO2 fast enough
Hypercapnia / hypercarbia (Type II Respiratory Failure): elevated dissolved CO2 in blood (PaCO2)
Cerebral vasodilation
Toxins: e.g. cyanide, pesticides, arsenic Severe anemia
Distributive problems:
Systemic inflammation (sepsis, anaphylaxis, pancreatitis), adrenal insufficiency, vasodilatory drugs
Obstructive problems: Cardiac tamponade*, tension pneumothorax* or massive pulmonary embolism*
Hypovolemic* problems (low blood volume): Hemorrhage, dehydration, widespread skin disruption or burns
Cardiac valve dysfunction
Myocardial infarction* or cardiomyopathy
Cardiac arrhythmia or heart block
Disturbed electrical activity in cardiomyocytes
Peripheral metabolic disturbances
Hypokalemia*, Hyperkalemia* Acidosis* (including renal failure) Hypothermia*
Toxins* (e.g. cocaine, beta blockers, tricyclics) Severe thyroid derangement
Inappropriate systemic vasodilation
Adjacent forces impair heart filling
Low cardiac preload
Low stroke volume (SV; depends on valves, contractility, preload)
Decreased systemic vascular resistance (SVR)
Low blood pressure (BP = CO x SVR)
Decreased cardiac output (CO = SV x HR)
Disseminated intravascular coagulationàwidespread thrombi that occlude blood flow (also causes hemorrhage, see relevant box at left)
Methemoglobinemia: some hemoglobin gets stuck in a state that can’t carry O2
Hemoglobin has reduced capacity to carry or release O2
Drugs: e.g. dapsone, nitrates
Carbon monoxide poisoning
Circulatory collapse / shock: inadequate perfusion of tissue with blood
Respiratory collapse: blood has insufficient useable O2 content
Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)
Hypoxia*: inadequate O2 delivery or utilization in tissues
Hypoxia creates metabolic disturbances that impair cardiac cells. Alternatively, any of the preceding conditions marked with (*) can directly trigger cardiac arrest first
Pulseless Electrical Activity (PEA): organized activity on ECG with no cardiac output (can be preceded or mimicked by pseudo-PEA, in which there is still some output on ultrasound)
Low atmospheric pressure or oxygen content Severe lung disease
Asthma, COPD, interstitial lung disease, congestive heart failure, pulmonary hypertension, pulmonary embolism, lung collapse / atelectasis
Acute respiratory distress syndrome
Pneumonia, aspiration pneumonitis, inhalational injury, systemic inflammation, drowning
Severe hypoventilation
Respiratory fatigue, advanced COPD, chest wall disorders, neuromuscular disorders, upper airway obstruction, toxins (e.g. opioids, botulism)
Can degenerate at any time
Asystole: no cardiac electrical activity or output
Death
Respiratory arrest: cessation of breathing
Inability to protect airway
Decreased level of consciousness
Note
This is a broad overview of the many scenarios that can result in death. For detailed explanations of the various disease mechanisms, refer to the corresponding slides.
* = reversible causes of cardiac arrest (Hs and Ts)
Author:
Ben Campbell
Reviewers:
Yan Yu*
Huma Ali*
* MD at time of publication
Bradycardia
(low heart rate, HR)
Unopposed parasympathetic stimulation of heart (can also cause vasodilation, see Distributive problems)
Disruption of spinal cord sympathetic control
Injury to cervical or upper thoracic spinal cord
Irreversible cessation of cardiac, respiratory, and brain function
Prolonged seizure initially causes increased cardiovascular activity, until the system fatigues
Disruption of respiratory control center in medulla
Expanding skull contents squeeze brainstem (herniation)
Increased intracranial pressure
Edema from intracranial hemorrhage, trauma, brain mass
Edema, inflammation, hypoxia and/or metabolic derangements cause diffuse neuron dysfunction
Central nervous system infection
Dementia, particularly with delirium
Massive ischemic stroke
Seizure
activity prevents or alters breathing
Metabolic disturbances that affect the central nervous system Hypoglycemia Hypocalcemia, hypercalcemia Hyponatremia, hypernatremia Uremia
Acute liver failure (hyperNH4) Many drugs / toxins Withdrawal (e.g. EtOH)
Status epilepticus
Brainstem lesion (e.g. stroke, neoplasm, inflammatory)
Nervous System Insult
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 11, 2023 on www.thecalgaryguide.com
Respiratory System Insult
Cardiovascular System Insult Cardiogenic problems")
آسم-چگونگی-اثر-درمان-ھا-و-عوارض-جانبی-ر

Pediatric Pneumonia Pathogenesis and Clinical Findings
 Kang Usama Malik Annie Pham Eric Leung* Jean Mah* * MD at time of publication
Immunological: unvaccinated, primary immunocompromise, pre-existing illness (e.g. HIV, measles), malnutrition
Environmental: smoke, air pollution, mold, crowded housing
Recent hospitalization or antibiotic-use
Physiological: neonates, low-birth weight, underlying lung disease
These factors make the host more susceptible to infection
Infection and proliferation of pathogen in lower respiratory tract/parenchyma
Pediatric pneumonia:
Inflammatory response to infection/proliferation of microbial pathogens at the alveolar level
Exposure to pathogen via inhalation, hematogenous, direct exposure, or aspiration
Epithelial cells in respiratory tract release cytokines that recruit neutrophils & plasma proteins to infection site, initiating a local inflammatory response
Cytokines released into the bloodstream (e.g. TNF, IL-1) initiate a systemic inflammatory response
↑ Vascular permeability
Accumulation of exudate, cellular debris, serous fluid, fibrin, or bacteria in the airway spaces
↑ Respiratory drive
Tachypnea
↑ Excitability of the peripheral somatosensory system
Circulating cytokines induce prostaglandin synthesis
Airway irritation as cilia are unable to efficiently clear fluid buildup
Crackles, ↓ breath sounds
Fluid, protein, or inflammatory cells leak into pleural space
Pleural effusion
Pulmonary edema
Fluid buildup in interstitial spaces ↑ gas diffusion distance
Bacteria enter the bloodstream (if bacterial pneumonia)
Sepsis
Fluid buildup in the alveoli ↓ available surface area for gas diffusion
↓ Efficiency of gas exchange
Intra- and extracranial arteries dilate
Headache
↑ Thermo-regulatory set-point of the hypothalamus
Fever
Myalgia
Hypoxemia
Malaise
Cough
Fluid accumulation in the pleural space prevents full lung expansion
↑ Work of breathing (tracheal tug, paradoxical abdominal breathing, subcostal/suprasternal indrawing)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 28, 2018; updated Aug 25, 2024 on www.thecalgaryguide.com
Pediatric Pneumonia: Pathogenesis and clinical findings
Authors: Jasmine Nguyen Nicola Adderley Reviewers: Midas (Kening) Kang Usama Malik Annie Pham Eric Leung* * MD at time of publication
Immunological: unvaccinated, primary immunocompromise, pre-existing illness (e.g. HIV, measles), malnutrition
Environmental: smoke, air pollution, mold, crowded housing
Recent Hospitalization: length of stay, recent antibiotics, mechanical ventilation
Physiological: neonates, low-birth weight, underlying lung disease (ciliary dysfunction, asthma, cystic fibrosis, bronchiectasis)
Host is more susceptible to infection
Exposure to pathogen:
inhalation, hematogenous, direct, aspiration
Infection and proliferation of pathogen in lower respiratory tract/parenchyma
Pediatric pneumonia:
Inflammatory response to infection/proliferation of microbial pathogens at the alveolar level
Notes:
• Additional findings in pediatric pneumonia may include increased
irritability, nausea/vomiting, diarrhea,
otitis, and headache
• Viral pathogens most common in
children <2yrs; bacterial pathogens most common in children >2yrs
Local inflammatory response: epithelial cells release cytokines in response to infection, which recruit neutrophils and plasma proteins to site of infection
↑ Vascular permeability causes accumulation of plasma exudate, cellular debris, serous fluid, fibrin, or bacteria in the airway spaces
Systemic inflammatory response:
Cytokine release (eg. TNF, IL-1)
↑ respiratory drive
Airway irritation as cilia are unable to efficiently clear fluid buildup
Crackles, ↓ breath sounds
Fluid, protein, or inflammatory
cells leak into pleural space
Pleural effusion
Pulmonary edema
Fluid buildup in interstitial spaces increases gas diffusion distance
Fluid buildup in the alveoli decreases
available surface area for gas diffusion
↓ efficiency of gas exchange
Bacteria invade into the bloodstream (if bacterial pneumonia)
Sepsis
Hypoxemia
Circulating cytokines induce prostaglandin synthesis, which raise the thermoregulatory set-point of the hypothalamus
paradoxical abdominal breathing, subcostal/suprasternal indrawing)
Fever
Cough
Fluid accumulation in the pleural space prevents full
lung expansion, resulting in ↓ lung volumes
Tachypnea
↑ Work of breathing (tracheal tug,
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Month Day, Year on www.thecalgaryguide.com
Pediatric Pneumonia: Pathogenesis and clinical findings
Immunological: immunization status, immune compromise
Environmental: second-hand smoke, air pollution
Hospitalization: length of stay, recent antibiotics, mechanical ventilation
Neonates, immunocompromise, underlying lung disease (ciliary dysfunction, Cystic Fibrosis, bronchiectasis)
Authors: Nicola Adderley Reviewers: Midas (Kening) Kang Usama Malik Eric Leung* * MD at time of publication
Additional findings in pediatric pneumonia may include nausea, otitis, headache
Viral pathogens most common in children <2yrs; bacterial pathogens most common in children >2yrs
Interstitial pattern: suspect Mycoplasma pneumoniae, Influenza A + B, Parainfluenza Lobar pattern: suspect S. pneumonia, H. influenzae, Moraxella, S. aureus
Systemic inflammatory response:
Cytokine release (eg. TNF, IL-1)
Exposure to pathogen: inhalation, hematogenous, direct, aspiration
Susceptible host and/or virulent pathogen
Infection and proliferation of pathogen in lower respiratory tract/parenchyma
Pediatric pneumonia:
Inflammatory response to proliferation of microbial pathogens at the alveolar level
Notes:
• •
• •
Local inflammatory response: neutrophils recruited to site of infection (LOBAR or INTERSTITIAL PATTERN, depending on pathogen) by epithelial cytokine release
Irritation of contiguous structures and/or referred pain (mechanism unclear)
Acute abdominal pain
Cough
Accumulation of plasma exudate (from capillary leakage at sites of inflammation), cell-debris, serous fluid, bacteria, fibrin
↑ respiratory drive
Disruption of hypothalamic thermoregulation
Fever/chills
Irritation of airways and failure of ciliary clearance to keep up with fluid buildup
Crackles, ↓ breath sounds
Fluid buildup in spaces between
alveoli (INTERSTITIAL PATTERN)
Interstitial opacity on CXR
Fluid buildup in alveoli (LOBAR PATTERN)
↓ efficiency of gas exchange (↑ diffusion distance in INTERSTITIAL, ↓ surface area in LOBAR)
Hypoxemia
Tachypnea
Lobar consolidation on CXR
Respiratory accessory muscle use (chest indrawing, paradoxical breathing, muscle retractions)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 28, 2018 on www.thecalgaryguide.com
gin")
Transient Tachypnea of the Newborn

↑ Work of breathing
Maternal factors leading to impaired fetal lung development
Lack of labour-induced hormone changes (i.e. cortisol, catecholamines)
↓ Alveolar fluid reabsorption through epithelial aquaporin channels
↑ Alveolar fluid in lungs Disruption of laminar flow in airways
↑ Resistance to airflow
↑ Lung expansion to compensate
Limited surface area for gas exchange in the alveoli
↓ Ventilation
Fluid buildup in the major bronchi in the perihilar region
Prominent perihilar streaking on chest x-ray
↑ Intrathoracic pressure pushes the diaphragm down
Blunting of costophrenic angle on chest x-ray
Hyperinflation of lungs
Expanded lung fields on chest x-ray
↑ Deoxygenated hemoglobin in the bloodstream
Blue/purple discoloration of the skin particularly around the lips & fingers (cyanosis)
↓ Oxygenated hemoglobin in the bloodstream
↑ Nasal passage size allows for more air to enter the lungs with each breath
Nasal flaring
Scalene/intercostal/ sternocleidomastoid /abdominal muscle activation to assist with breathing
Accessory muscle use
↓Oxygen saturation (SpO2)
Neonate takes more breaths to compensate for limited oxygenation
Respiratory rate > 60 breaths/minute (tachypnea)
Transient Tachypnea of the Newborn
Temporary respiratory condition in newborns characterized by impaired lung function and rapid breathing
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")
Pulsus Paradoxus

Thoracic cavity expands
Lungs expand and intrathoracic pressure ↓
Physiologic:
↑ Venous return to right (R) heart
↑ R heart preload (volume of blood inside the ventricle right before it contracts)
↑ Blood pools in the right side of the heart
Obstructive lung diseases (e.g., COPD**, asthma**)
Hyperinflated lungs
↑ Stretching of pulmonary vessels at rest
On inspiration, ↑↑ stretching of pulmonary vessels
↑↑ Blood pools within pulmonary vasculature
↓↓ Flow to L heart
Pathologic: Constrictive pathologies (e.g., cardiac
tamponade**, constrictive pericarditis**) Decreased pericardial compliance
Constriction of ventricles
On inspiration, ↑ venous return to R heart (normal)
R ventricle unable to fully expand due to ↓ compliance
Septum bows into L ventricle
L ventricle unable to fully expand ↓↓ Filling of L heart
↓↓ L ventricular end diastolic volume
↓↓ L heart stroke volume ↓↓ Cardiac output Pulsus Paradoxus
Exaggerated ↓in systolic BP on inspiration (>10mmHg)
Air flows into the lungs
Pulmonary vessels are physically stretched/pulled
↑ Blood pools in pulmonary vessels
↓ Return of blood to left (L) heart
↓ L heart preload
↓ L heart stroke volume
↓ Cardiac output
Obstruction of superior or inferior vena cava (e.g., clot)
↓↓ Venous return to R heart at rest
↓↓ Right heart filling
↓↓ Blood flow to pulmonary arteries
Pulmonary embolism**
Clot occludes pulmonary arteries/ arterioles
↓↓ Flow to pulmonary veins
At rest, ↓↓ flow to L heart
On inspiration, ↓↓↓ flow to L heart
↓ Systolic blood pressure (BP) of < 10mmHg on inspiration
BP = cardiac output x systemic vascular resistance
**See corresponding Calgary Guide slides
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 21, 2013; updated Dec 3, 2024 on www.thecalgaryguide.com")
Pediatric Asthma Exacerbations

Allergic asthma (triggered by allergens)
(e.g., pollen, animal dander, dust mites)
Viral respiratory
tract infections
Extreme weather Physical exertion Pollutants (e.g.
cigarette smoke)
Allergen inhalation
activates IgE on mast cells
Virus invades epithelial
cells in airway
Inhalation of cold
↑ Minute ventilation
or dry air dries
↑ Air flow irritates & dries airway mucosa
airway mucosa Inhaled irritants
damage airway
Epithelial barrier breakdown
releases inflammatory mediators
epithelium & activate
immune cells
Immune system releases inflammatory mediators (e.g., histamine, leukotrienes, prostaglandins, cytokines) into airway
Histamine & leukotrienes stimulate smooth
muscle cells in the airway to constrict
Cytokines attract white blood cells (e.g.,
eosinophils, neutrophils, monocytes)
Inflammatory mediators
stimulate epithelial goblet cells
Inflammatory mediators ↑ vascular
permeability in airway mucosa
Bronchoconstriction
(bronchioles narrow)
Airway inflammation
persists & intensifies
Goblet cells produce excess mucus
plugs & obstruct small airways
Airway wall swells
(mucosal edema)
Asthma Exacerbation
Acute or sub-acute episode marked by a progressive ↑ in asthma symptoms & a measurable ↓ in lung function compared to patient’s baseline
Bronchial hyperresponsiveness (an exaggerated & easily
triggered constricting response of the airways to various stimuli)
Narrowed bronchioles mechanically
obstructs air flow & ↓ ventilation
↓ Ventilation impairs
elimination of carbon
dioxide (CO₂) from blood
More force is
required to
expel air
Turbulent airflow through
narrowed bronchioles
during expiration
Severe airflow obstruction
prevents airflow into distal
lung regions
↓ Ventilation
traps air in
alveoli
Prolonged
expiratory phase
Inflammatory
mediators & mucous
hypersecretion
sensitize afferent
nerves in airway
↑ Arterial partial
pressure of CO2 (PaCO2))
triggers hyperventilation
↑ Work of
breathing
Expiratory
wheeze
↓ Breath
sounds
Afferents activate
cough reflex via
Trapped air ↑ intra-
Air trapping
alveolar pressure
overinflates
vagus nerve
above pleural pressure
lungs
Cough
↓ PaCO2
↑ blood
pH
Tachypnea
(↑ respiratory
rate)
Exhaustion of
respiratory muscles
↓ strength &
respiratory rate
Air trapping limits oxygen
(O2) exchange in alveoli
↑ Pressure
ruptures alveoli
↓ Diaphragmatic
excursion
Hyperinflation
on chest X-ray
Pneumothorax (air collects in pleural space)
↓ Oxygenation of
blood (hypoxemia)
Respiratory
alkalosis
Normocapnia,
can progress
to hypercapnia
(↑ PaCO2)
Engagement
of accessory
respiratory
muscles
Respiratory
failure
↓ O2 delivery to
peripheral tissues
Legend: Authors:
Fares Senjar, Jody Platt
Hypoxemic hypoxia (SpO2 < 90% on room air)
Reviewers:
Merry Faye Graff, Emily J. Doucette,
Central cyanosis (bluish discoloration
of skin & mucous membranes)
Elizabeth De Klerk, Yan Yu,
Alexander Arnold, Naminder Sandhu*,
Jonathan Liu*
Tachycardia (↑ heart rate)
*MD at time of publication
Complications
Published Dec 2, 2013; updated Nov 15 2025 on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding")