SEARCH RESULTS FOR: cirrhosis
Clinical Findings of Androgen Deficiency
![Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Clinical-Findings-of-Androgen-Deficiency.jpg "Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words")
cirrhosis
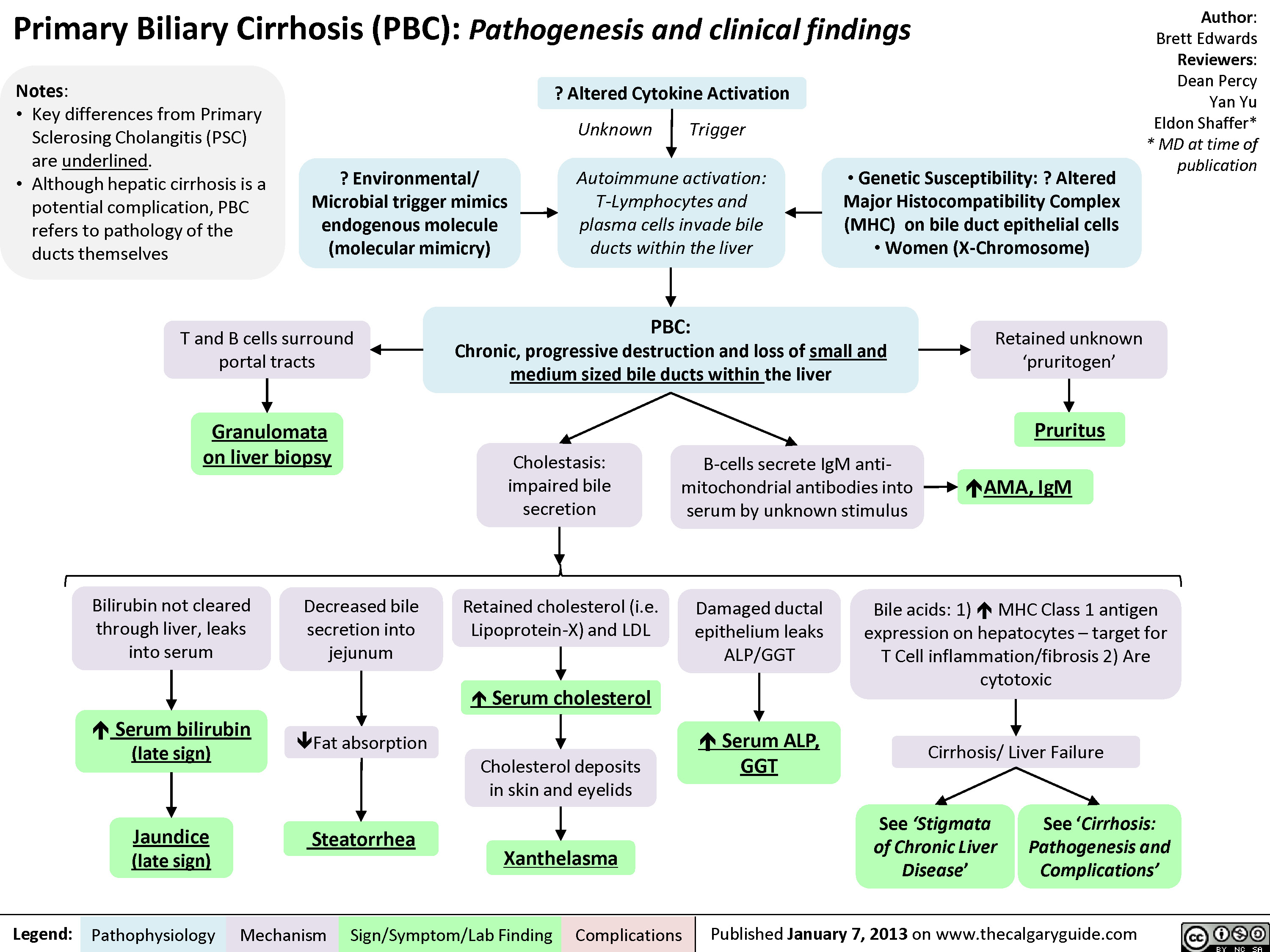
Primary Biliary Cirrhosis (PBC)
esophageal-gastric-varices

Legend:
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
• Venous drainage of spleen backed up into gastric anastomoses
Tachycardia and hypotension
Anemia Death Melena Coffee ground emesis Hematemesis Bright red blood per rectum")
Hepatitis C (HCV) Infections: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Hepatitis C (HCV) Infection: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Hepatic Encephalopathy: Pathogenesis and Clinical Findings

Hyponatremia- Physiology
![Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/01/Hyponatremia-Physiology-.jpg "Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com")
Biliary Atresia (BA)- Pathogenesis and clinical findings
- Pathogenesis and clinical findings Intrauterine environment genetic factors abnormal bile duct development toxic inflammatory response viral immunologic injury to bile duct epithelia pathophysiology poorly understood histology consistent with obstruction on liver biopsy biliary atresia progressive idiopathic fibre-obliterative disease extra-hepatic biliary tree biliary obstruction on intra-operative cholangiogram (diagnostic) partial complete bile duct obstruction delivery of bile acids to small intestine pressure in bile duct absorption of fat and soluble vitamins vitamin K+ deficiency coagulopathy INR PTT bruising petechiae acholic pale stool failure to thrive elimination of bilirubin conjugated direct bilirubin jaundice pruritus excreted urine dark urine diaper yellow pressure bile duct GGT backs up in liver cholestatic hepatitis firm enlarged liver fibrosis cirrhosis ALT AST Horwitz Adderley McKenzie")
Hemorrhoids - Pathogenesis and Clinical Findings

Increased Intra-Abdominal Pressure
I.e. pregnancy, constipation, chronic straining,
lifting, cirrhosis
Hemorrhoids: Pathogenesis and clinical findings
Dilations originate from inferior
hemorrhoidal venous plexus
Vascular cushions engorge
along anal canal
Legend: Published March 30, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Authors:
Aleeza Manucot
Reviewers:
Yoyo Chan
Sean Doherty
Dr. Sylvain Coderre*
* MD at time of publication
Supporting tissues of anal cushions weaken,
disintegrate, or deteriorate
Inflammatory reaction
occurs, involving vascular
wall and connective tissue
Thrombosis
Pain
↑ mucus secretions or fecal
soiling of prolapsing
hemorrhoids
Cushion epithelium erodes via
damage from compression
Painless
rectal
bleeding
Bleeding without prolapse
Prolapse with spontaneous
reduction
Prolapse requiring manual
reduction
Irreducible
1st degree
2nd degree
3rd degree
4th degree
Infarction and thrombosis
Acute severe pain
Anal cushions prolapse (downwardly slide)
into rectum or open space
Dentate line: divides
the upper two thirds
and lower third
of the anal canal
EXTERNAL Hemorrhoids
- Found distal to the dentate line
- Somatic innervation
Somatic nerve
receptors activated
Sebaceous glands
↑ secretions around
area of hemorrhoid
Itching Perianal
irritation
Swelling
Inflammation creates
prothrombotic state
Hemorrhoids")
Wilson's Disease

Hepatic Cu accumulation, deposition in hepatocyte lysosomes
Hepatocyte injury (speculated mechanism: free radicals)
Cu leak from damaged hepatocytes
Epidemiology:
• Autosomal Recessive condition with prevalence of 1:30,000 • 60% of cases present initially with neurologic Symptoms
• Fulminant cases present with acute liver failure and massive
hemolysis, treated with liver transplant
↓ ceruloplasmin release ↓ serum ceruloplasmin
Early asymptomatic liver dysfunction
Cu movement into bloodstream
Cu deposition in vulnerable tissues
Abbreviations:
• Cu - Copper
• AST - Aspartate Aminotransferase • ALT - Alanine Aminotransferase
↑ AST, ALT, and Bilirubin
↑ Serum free Cu (total usually low due to low ceruloplasmin)
Eyes: Kayser-Fleischer rings
CNS: Neurologic disease, Psychiatric disease MSK: Arthropathies
Kidney: Fanconi syndrome, Kidney stones
Chronic hepatitis, Cirrhosis with hepatic insufficiency, Portal hypertension, Hemolysis, Acute Liver Failure
Continued hepatocyte injuryà progressive liver damage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 17, 2019 on www.thecalgaryguide.com")
Incisional-Hernia
 that ↑ risk of infection
Post-op wound Infection
Obesity
Chronic constipation
Chronic cough Pregnancy
↓ clotting factors
Vigorous cough
Severe Hypertension
Seroma
Post-op hematoma Bulging fluid separates High risk
Sutures unsuitable Poor surgical for tension technique
↑ intraabdominal pressure
Fascial Incision separates
Notes:
fascial incision
surgeries* High Risk Surgeries*
Connective tissue disorder
Suboptimal fascial closure
• • •
Emergency surgeries Midline incisions
Acute abdominal surgeries
↓ wound healing/collagen synthesis
Fascial defect at previous incision site
Incisional Hernia:
Protrusion of tissues through prior fascial incision
• Deep wound infection = most common cause of incisional hernias
• Diagnosis on physical exam +/- CT scan if patient is obese
• Treatment = surgery
Bulge at prior incision site
Palpable fascial defect
Bowel and other abdominal contents protrude through defect
Mechanical bowel obstruction (see relevant slide)
Constipation /obstipation
Contents unable to be pushed back through defect (incarceration)
Vascular supply is compromised to herniated contents
Contents become ischemic (strangulated)
Prolonged pressure on skin & bowel over time
Ulceration & ischemia
↓ blood flow to skin layers
Discoloration of skin
Bulge ↑ with coughing/straining
Ulcers extend through bowel wall
Authors: Karly Nikkel Meaghan Ryan Reviewers Michael Blomfield Tony Gu Yan Yu* Edwin Cheng* *MD at time of publication
Colo-enteric fistula
Bowel Perforation
Abdominal Pain
Abdominal Distension
Nausea/ Vomiting
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 13, 2019 on www.thecalgaryguide.com")
A1AT-Deficiency
 allele(s)
Accumulation of mutant α1AT protein as ordered polymers in endoplasmic reticulum of hepatocytes
↓ α1AT inhibition of Hepatocyte Injury tissue proteases (Mechanism unclear)
↓ release from hepatocytes
Cirrhosis, chronic hepatitis, hepatocellular carcinoma
↓ lung elasticity, ↓ ability for lung to expel air on expirationà gas trapping, hyperinflation, airway collapse over time
Role of Genetics:
Low serum α1AT
In the skin: Subcutaneous proteases > Anti- proteases
Unopposed proteolysis in subcutaneous tissues
Panniculitis (Rare, most cases associates with ZZ Genotype)
Lung Proteases > Anti-proteases àproteolytic destruction of lung parenchymaàpanacinar emphysema (accelerated by smoking)
Stigmata of chronic liver disease (ascites, jaundice, spider nevi, petechiae, etc.)
Symptoms of chronic obstructive pulmonary disease (COPD): barrel chest/High residual volume (RV), low vital capacity (VC), wheezes on auscultation, etc) – see relevant slide
Degree of α1AT deficiency dependent on genotype:
• MM gives normal α1AT levels
• MZ genotype produces levels ~ 35% of normal
• ZZ genotype produces severe deficiency ( <10% of normal)
• Null phenotype is completely deficient of α1AT
N.B. Heterozygotes almost never develop phenotypic α1AT deficiency syndromes. Even some homozygotes don’t manifest the disease.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published January 12, 2020 on www.thecalgaryguide.com")
Viral-Hepatitis
 of hepatocytes
Infection with chronic viruses (HBV and HCV) persist over time and additional symptoms may develop
RUQ pain/tenderness
If infection is prolonged or severe, inflammation becomes systemic
Release of hepatocyte’s cellular contents into the bloodstream
Infection with acute viruses (HAV and HEV) resolve over time, and the symptoms above normalize
Notes:
• HDV can only infect people with concomitant HBV infection
• HAV and HBV vaccines are the only ones that currently exist
• Not all patients with viral hepatitis will develop each of these symptoms. The presentations vary.
Fever, nausea, vomiting ↑ serum ALT, AST
↓ Hepatic metabolic activity (e.g. reduction of gluconeogenesis) ↓Serum Glucose
↓ Synthesis of plasma proteins (albumin, clotting factors, etc) ↓ Albumin, ↑ INR
Abbreviations:
• HAV - Hepatitis A Virus
• HBV - Hepatitis B Virus
• HCV - Hepatitis C Virus
• HEV - Hepatitis E Virus
• RUQ - Right Upper Quadrant
• ALT - Alanine Aminotransferase
• AST - Aspartate Aminotransferase
• INR - International Normalized Ratio
↓ Bilirubin clearance from blood, bilirubin ends up under the skin Jaundice Portal Hypertension
Encephalopathy, Splenomegaly, Esophageal Varices, Ascites, Caput Medusae, Edema
Encephalopathy, Muscle Wasting, Metabolic Bone Disease, Terry’s Nails, Ascites, Bruising, Clubbing, Edema
Spider Nevi, Altered Hair Patterns, Testicular Atrophy, Gynecomastia, Palmar Erythema
Progressive deterioration in liver function, possibly ending up in cirrhosis. (See slide on “Cirrhosis: pathogenesis and complications” for more details on mechanisms and full explanations.)
Hepatic Insufficiency Hyperestrogenism
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published January 12, 2020 on www.thecalgaryguide.com")
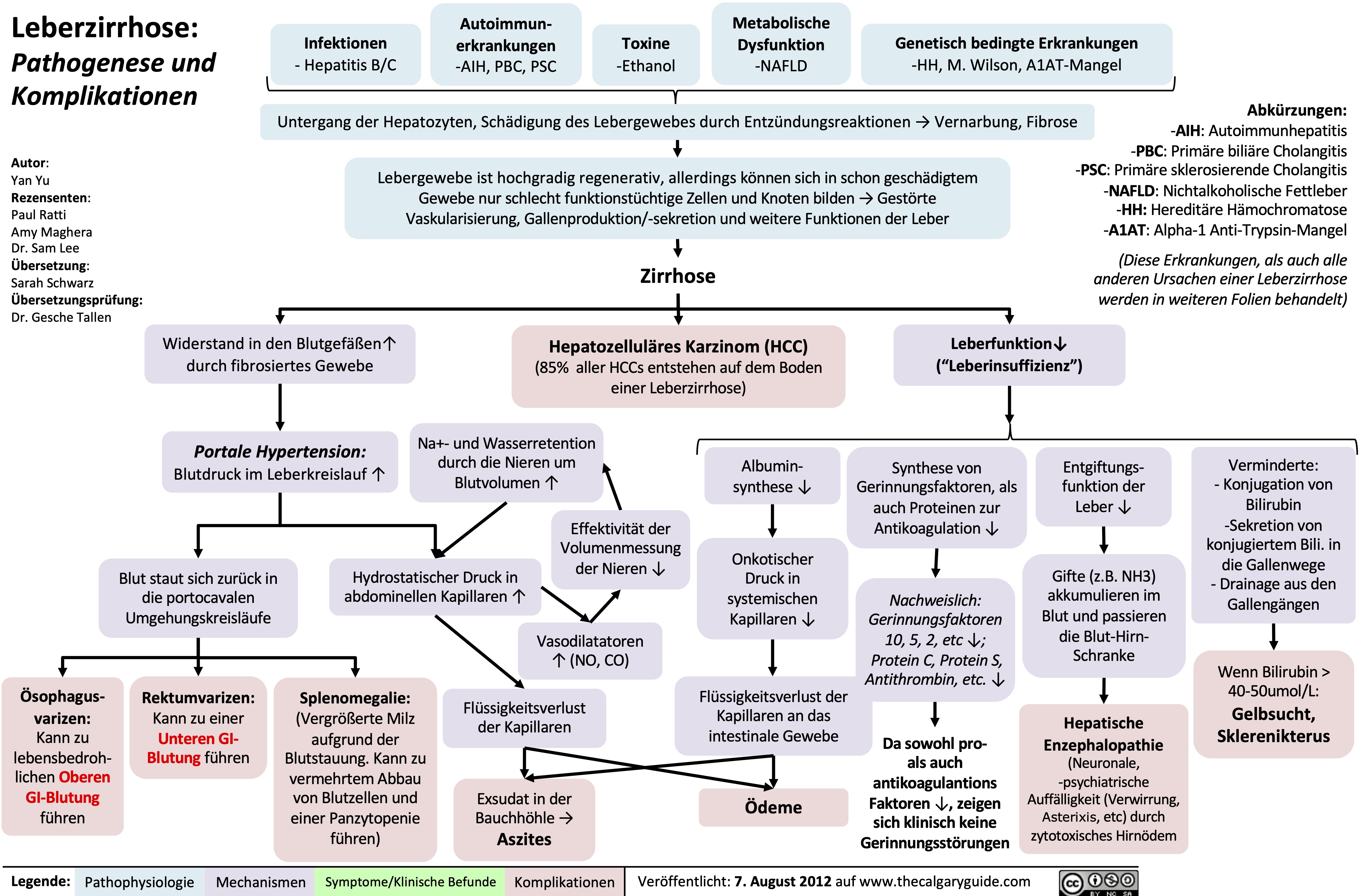
leberzirrhose-pathogenese-und-komplikationen
NSAIDs and the Kidney mechanism of action and side effects
 or angiotensin II receptor blockers (ARB)
AECi and ARBs act to ↓ renin- angiotensin-aldosterone system (RAAS) activation
Reduced angiotensin (AT) 2 activity at its receptors on efferent arteriole of the nephron
Net vasodilation of efferent arterioles ↓ in glomerular pressure
↓ blood perfusing kidney tissueà↑ hypoxemia & renal ischemia
Pre-existing ↓effective arterial blood volume (EABV) from
dehydration, GI loss, diuretics, CKD, CHF, cirrhosis, etc.
Decreased EABV triggers endogenous renal autoregulation, resulting in norepinephrine (NE) mediated vasoconstriction of afferent arteriole of the nephron
Net ↓ in renal blood flow and ↓ in glomerular pressure
↓ volume of blood filtered by the glomeruli per unit time
Non-steroidal anti-inflammatory drugs (NSAIDs)
Inhibition of Cyclooxygenase COX-1 (expressed in kidney) and COX-2 (expressed in kidney and sites of inflammation)
↓ Renal prostaglandin (PG) synthesis: local hormones involved in renal homeostasis
NSAID induced nephrotoxicity:
associated with chronic usage independent of dosage
(see Calgary Guide slide on NSAIDs and the Kidney: NSAID induced nephrotoxicity)
↓ intrarenal PG reduces inhibitory effects of PG over ADH in cortical colleting duct (CCD) of the kidneyà↓ antagonism on ADH activity
↑ ADH activity causes insertion of more
aquaporins (water channels) in the collecting duct of renal tubules
Net ↑ in volume of water reabsorbed into the blood
↓ vasodilatory effect of PG at the afferent arteriole of the nephron
↓ Glomerular filtration rate (GFR)
↓ PG signalling results in ↓ renin secretion at juxtaglomerular apparatus
Low renin levelsà↓ conversion of angiotensinogen into its AT1 form and, by extension, ACE mediated conversion of AT1 to AT2
↓ ACE 2 signalling leads to ↓ levels of aldosterone in the serum
↓ Na+ and K+ channel insertion on apical surface and ↓ Na/K ATPase activity on basolateral surface of principal cells
↓ K+ excretion into urine, and ↓ Na+ reabsorption
back into the blood, at the late DCT and collecting duct of the kidney
Pre-renal Acute Kidney Injury (AKI): kidney injury due to renal hypoperfusion
Prolonged and/or severe ischemia causes cell death and aggregation of tubular epithelial cells of the kidney with subsequent inability to reabsorb luminal Na+
Renal dehydration predisposes
precipitation of uromodulin protein
Renal tubules mold uromodulin into cylindrical structures known as “casts”. Casts that contain only uromodulin protein are known as “hyaline casts”
Hyaline cast seen on urinalysis
Hypoperfusion of the kidney activates the renin- angiotensin- aldosterone system (RAAS)
↑ amount of sodium (Na) reabsorbed from the filtrate (less Na excreted)
Fractional excretion of Na <1%
Papillary necrosis: ureteral passage of sloughed ischemic tissue causing ureteral obstruction
Acute tubular necrosis: a type of kidney injury causing damage to the tubules
Hypertension
Post-renal AKI: a type of kidney injury due to
obstruction of the urinary tract
Distal distal obstruction of the urinary tract causes fluid to accumulate within the kidneysàenlarging the kidneys
Renal Ultrasound shows hydronephrosis (enlarged kidneys)
Damaged tubule epithelial cells slough into the tubular lumen
Epithelial cell breakdown in the tubular lumen
releases uromodulin & other proteins, which aggregate into “casts” (cylindrical imprints of the renal tubule). The varied protein content of these casts result in them having a coarse, granular appearance
Damaged tubular epithelial cells are unable to properly reabsorb sodium
↓ amount of sodium (Na) reabsorbed from filtrate into the blood (more Na excreted)
Fractional excretion of Na >2%
True excess of free water relative to Na+ in the blood
Excess free water ↑ venous hydrostatic pressure (see Calgary Guide slide on edema for full mechanisms)
Pitting Edema
Hyperkalemia
Hyponatremia
Coarse granular casts seen on urinalysis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 29, 2022 on www.thecalgaryguide.com")
clostridium-difficile-infection-pathogenesis-and-clinical-findings
 Infection
Authors: Ryan Brenneis, Sravya Kakumanu Reviewers: Yoyo Chan, Sean Doherty, Vina Fan, Ben Campbell, Dr. Steve Vaughan*, Dr. Sylvain Coderre* * MD at time of publication
Community exposure
Infected close contacts
Nosocomial exposure (most common)
Poor hand hygiene and sanitization of surfaces and medical equipment
Nosocomial risk factors
Any antibiotic use
(Especially clindamycin, fluoroquinolones, penicillins, cephalosporins)
↑ Antibiotic resistant strains
Presence of pre-disposing risk factors
(Note: do not need to be present for infection)
Recent GI surgery
Chemotherapy that has antimicrobial and immunosuppressive effects
Usage of medications that reduce stomach acid (↑ pH)
↑ C. diff spores on surfaces and personnel
Contact exposure
Environmental exposure
to C. diff carriers
Inoculation of GI tract
Disruption of normal gut microbiome allowing C. diff overgrowth
Comorbidities
(>65 years old, cirrhosis, inflammatory bowel disease, enteral feeding, obesity)
via fecal-oral route
Clostridium difficile Infection of GI Tract
Spores unaffected by antibiotics germinate post-antibiotic treatment
Infection recurrence
Pseudomembranous colitis on endoscopy
(colonic ulcerations potentially seen with severe infection)
Hypotension Acute kidney injury
Release of C. diff toxin A and B inactivates Rho and Ras GTPases in colonic epithelial cells (colonocytes)
(Rho and Ras GTPases control cytoskeletal dynamics and gene expression)
Cytoskeletal disorganization and arrest of RNA synthesis causes necrosis of colonocytes and triggers host immune response
Neutrophil chemotaxis and activation
↑ Inflammation of colon
Disruption of tight junctions between colonocytes
Release of fluid into intestinal lumen and inability of colon to reabsorb it
Toxic megacolon
Bowel perforation
Bloody stool
(<10% of patients)
Abdominal cramps
Large bowel dilation from muscle paralysis
Inflammation and destruction of underlying smooth muscle
Breakdown of colonocyte cell membranes
Inflammation of visceral peritoneum
Volume depletion
Watery diarrhea: ↑ frequency, small volume
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 30, 2019, updated May 16, 2022 on www.thecalgaryguide.com")
transudative-pleural-effusions-pathogenesis-and-lab-findings

Left ventricle unable to pump sufficient blood into systemic circulation
Backup of blood in pulmonary veins
↑ Hydrostatic pressure
in pulmonary veins
Pulmonary embolism
R ventricle unable to pump blood due to clot in pulmonary artery
Backup of blood in systemic veins
↑ Hydrostatic pressure
in veins draining parietal pleura
Nephrotic syndrome
Damaged glomerulus has ↑ permeability to plasma proteins in blood
↑ Loss of proteins through urine
↓ Oncotic pressure
in systemic capillaries (including within parietal pleura)
Normally, permeable pleural capillaries do not allow protein leakage into the pleural space
↑ Interstitial fluid leakage across intact pulmonary or pleural capillaries into pleural space
Transudative Pleural Effusion
Absence of bacteria and inflammatory cells in pleural space
No increase in cellular activity in pleural space
Normal levels of glucose metabolism in pleural space = low lactate dehydrogenase (LDH) (LDH increases when glucose metabolism, particularly glycolysis, increases to maintain supply of NAD+)
Large accumulation of pleural fluid (PF) pressing against lung tissue and mediastinum
Lung atelectasis (lung collapse)
See Pleural Effusions: X- ray Findings and Physical Exam Findings of Lung Diseases slides
PF/serum protein ratio < 0.5
PF LDH < 2/3 upper limit of normal
Light’s Criteria: All three criteria must be met to be a transudative pleural effusion
PF/serum LDH ratio < 0.6
See Hypoxemia: Pathogenesis and Clinical Findings slide for pathophysiology and signs of hypoxemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 9, 2022 on www.thecalgaryguide.com")
lower-gi-bleed-risk-factors

Rectal varices (large veins in the rectum that are at risk for bleeding)
Splenomegaly (enlargement of the spleen)
Large spleen sequesters (traps) platelets, reducing blood platelet counts
↓ Clotting ability of the blood
↓ Epithelial protection along entire GI tract
Pre-existing damage to the lower GI tract epithelium
Malignant tissue invades the colon wall and disrupts colonic blood vessels
New, extremely friable blood vessels develop within the tumor
Venous blood pressure exceeds vessel wall strength, and the vessel ruptures and bleeds
Blood moves rapidly through the GI tract (this is an upper GI bleed that can produce lower GI bleed symptoms)
Hematochezia
(bright red blood per rectum)
Damaged liver tissue restricts
blood flow through liver
hypertension (high blood pressure in the veins running from the GI tract to the liver)
Blood backs up in the splenic vein
Venous blood pressure exceeds vessel wall strength, and the vessel ruptures and bleeds
Liver cirrhosis
Authors: Yan Yu, Miranda Schmidt Illustrator: Mizuki Lopez Reviewers: Michael Blomfield, Tony Gu, Jason Baserman, Jennifer Au, Vina Fan, Ben Campbell, Kerri Novak* * MD at initial time of publication
↓ Synthesis of blood clotting factors that are normally produced in the liver (i.e. fibrinogen)
Bleeding of capillaries under the skin
Petechiae
(small red dots on skin)
Inferior Vena Cava
Blood clotting defect (genetic disorder, Acetylsalicylic Acid use)
Non-Steroidal Anti- Inflammatory Drug (NSAID) Use
Prior lower GI bleeds
Family history of colorectal cancer
Diaphragm
Esophagus
↓ Systemic prostaglandin synthesis
↑ Risk for lower GI bleed
↑ Risk for colorectal cancer
Development of colorectal cancer
Duodenum
Ligament of Treitz
Lower GI Bleeds are intra-luminal GI tract bleeds that occur anywhere distal to the ligament of Treitz (transition between duodenum and jejunum)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 30, 2019, updated August 15, 2022 on www.thecalgaryguide.com")
Acute Liver Failure: Pathogenesis and clinical findings

NAPQI binds hepatocellular proteins
(see Acetaminophen Overdose: pathogenesis and clinical findings slide)
Drug-induced liver injury
Metabolism of drugs by the liver can produce reactive drug metabolites
Intracellular stress, mitochondrial injury, or immune response
Viral Hepatitis (i.e. HAV, HBV, HEV, HSV)
Acute infection or infection flare provokes an immune response against infected hepatocytes
Autoimmune Hepatitis
Autoimmune antibodies attack hepatocytes (see Auto-immune Hepatitis (AIH) slide)
Ischemia (i.e. from shock)
↓ O2 delivery to the liver
Hepatocellular hypoxia
Wilson’s Disease
Heritable mutation in the ATP7B gene
↓ Biliary excretion of copper
Hepatic copper accumulation injures hepatocytes (see Wilson’s Disease slide)
Accelerated rate of hepatocellular necrosis or apoptosis
Hepatocyte death exceeds regeneration such that liver function is compromised within a short amount of time
Acute Liver Failure
An illness of <26 weeks duration in the absence of pre-existing cirrhosis, characterized by INR ≥1.5 and evidence of altered mentation (hepatic encephalopathy)
Injured hepatocytes leak hepatic enzymes (AST, ALT, GGT) into circulation
↑ Liver enzymes
Hepatocellular inflammation
Stimulation of foregut
autonomic nerves
Right upper quadrant pain
↓ Toxin metabolism
Toxins build up and activate microglial cells (brain macrophage)
Oxidative stress and cerebral edema
Hepatic encephalopathy
Characteristic set of neuropsychiatric symptoms (see Hepatic Encephalopathy slide)
↓ Hepatocellular function and number
↓ Complement protein synthesis
↓ Ability to clear immune complexes and activate B cells
Accumulation of pigmented bilirubin
↓ Synthesis of coagulation factors
↑ INR
↓ Conjugation of bilirubin by the liver and ↓ transport into bile for excretion
↑ Serum bilirubin
Jaundice
Infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 15, 2022 on www.thecalgaryguide.com")
hypovolemic-shock

Inflammation (pancreatitis, cirrhosis, post-operative, etc.)
Inflammatory mediators vessel permeability and fluid leaks out
Trauma
Ruptured vessels leak fluid into potential spaces
Hemorrhagic losses
(GI bleed, postpartum hemorrhage, etc.)
↓ Intravascular volume
↓ Venous return to the heart
↓ Cardiac output (blood pumped from the heart)
Hypovolemic Shock
↓ Oxygen delivery to tissues due to low blood volume
Insufficient organ perfusion
Non-Hemorrhagic losses
(dehydration, GI losses, skin losses / burns, renal losses, etc.)
‘Third Spacing’ of fluid
(fluid located outside the intravascular or intracellular space; large collections can occur in the pelvis, thorax, GI tract, long bones of children, intra-abdominally, retroperitoneally)
P = Q x R; less ‘flow’ in the vessels (Q), with vessels not constricting enough to maintain resistance (R)à pressure (P) will drop
↓ Blood Pressure
Caution: young, healthy individuals can maintain blood pressure during circulatory collapse with cardiac output and vasoconstriction; do not use blood pressure as an indicator of shock severity in children
Carotid sinus baroreceptors sense low blood pressure ↓ Carotid sinus inhibition of sympathetic nervous system Release of sympathetic catecholamines (epinephrine and
↓ Pressure in venous circulation
Brain
Heart
Kidneys
↓ Blood in the right internal jugular vein
↓ Oxygen delivery to the brain
↓ Myocardial contractility (from lactic acidosis)
↓ Blood flow to kidneys
↓ Jugular Venous Pressure
Catecholamines bind to beta-1 receptors in the sinoatrial node of the heart
Beta-1 receptor activation causes ↑ heart rate
Tachycardia
norepinephrine)
Catecholamines bind to and stimulate alpha-1 receptors in peripheral vessels
Vasoconstriction of peripheral vessels
↓ Blood flow to peripheral tissue
Catecholamines bind to and stimulate beta receptors in sweat glands
Diaphoresis
(sweating)
In all body tissues
Inadequate oxygen delivery
↓ ATP production
↑ Anaerobic metabolism
↓ Body temperature
Impaired neurological functioning
Renal ischemia
Activation of the renin-angiotensin aldosterone system
↓ Glomerular filtration rate
↓ Clearance of lactic acid by the kidney
↑ Lactic acid production
↓ Rate of activity of clotting enzymes
Lactic Acidosis
Unknown mechanism
Coagulopathy Hypothermia
Trauma Triad of Death
↑ Capillary Cold, mottled refill time extremities
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 24, 2013, updated December 4, 2022 on www.thecalgaryguide.com")
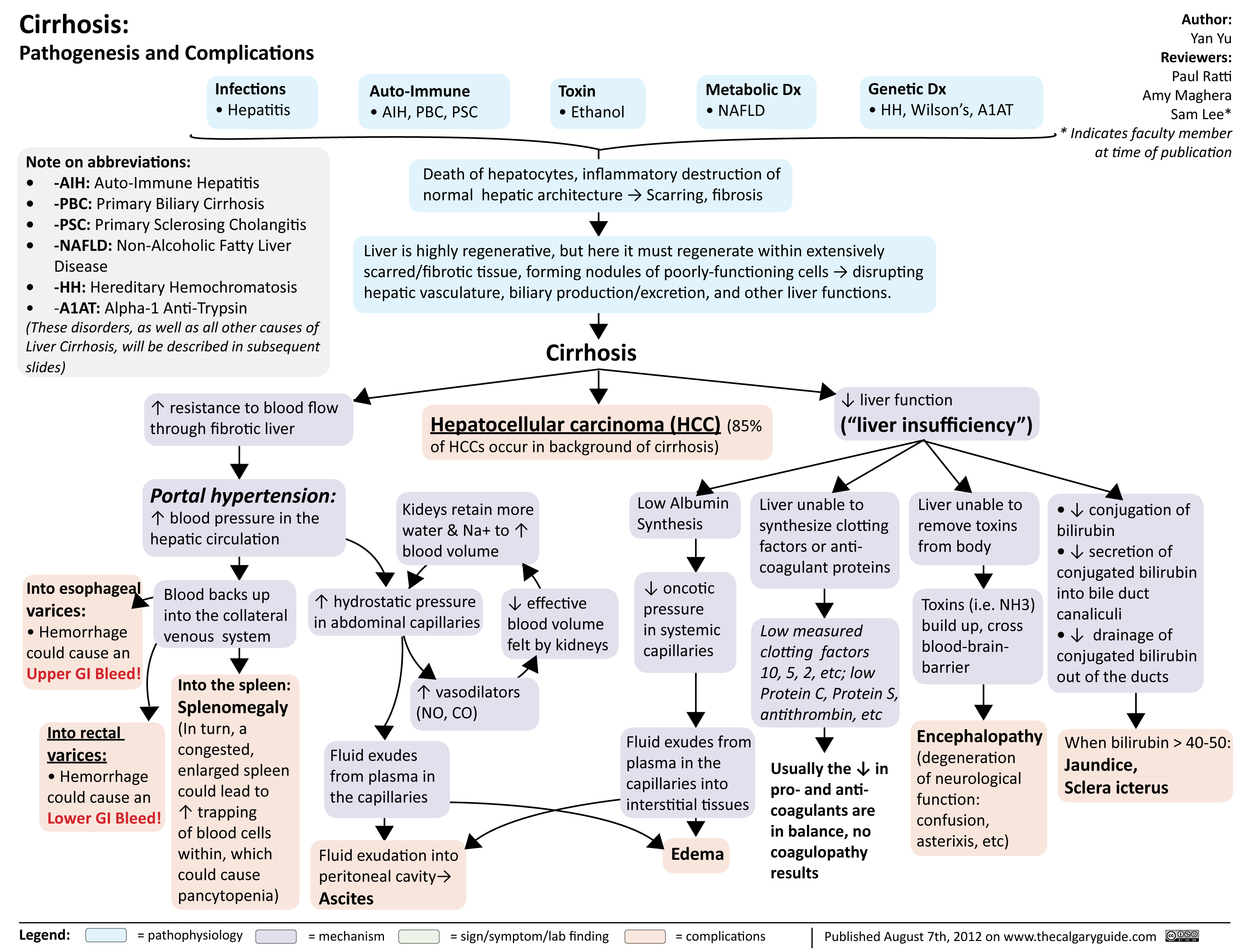
Cirrhosis
 Hepatitis D occurs with hepatitis B
Alcohol related liver disease
Non-alcoholic steatohepatitis
Autoimmune: autoimmune hepatitis, primary biliary & sclerosing cholangitis
Genetic: hemochromatosis, Wilson’s disease, α1- antitrypsin deficiency
Toxic: drugs may rarely cause chronic liver disease or cirrhosis
Severe or chronic hepatocyte injury overrides regenerative capacity → Fibrosis
Cirrhosis
Mild fibrosis may reverse with treatment of underlying cause
Nodular/shrunken liver on ultrasound
↑ Liver stiffness on transient elastography Diffuse fibrosis with nodular regeneration on biopsy
Fibrotic liver provides ↑ resistance to blood flow
Portal hypertension
Irreversible formation of fibrosis, within which hepatic cell regeneration is restricted to form nodules of poorly-functioning cells
Inflammation → epigenetic changes, oncogene mutations
Hepatocellular carcinoma
↑ Serum α-fetoprotein (sensitivity 50%, specificity 99%)
Fibrosis disrupts normal function of hepatic lobules
Hepatic insufficiency
↓ Liver synthetic function
↓ Thrombopoietin synthesis
Thrombocytopenia
↓ Conjugation of bilirubin,
↓ secretion of bilirubin into bile ducts, and
↓ drainage of bilirubin into hepatic duct
Accumulation of serum bilirubin >30 μmol/L
Jaundice
Scleral icterus, jaundiced frenulum
↑ Pressure in portal venous circulation
Portosystemic shunts
Increased flow to esophageal, rectal, and splenic veins
Vascular stretch → endothelial vasodilator (e.g. NO) release
Vasodilators enter systemic circulation
Pulmonary vasodilation
Blood cells in pulmonary vasculature have ↓ time for gas exchange
Hepatopulmonary syndrome (rare)
Dyspnea or hypoxemia, worsened when upright
↓ Synthesis of clotting factors (V, VII, IX, X, XI, XII, fibrinogen, prothrombin) and anticoagulant proteins (antithrombin, proteins C/S)
Unpredictable imbalance of hemostatic and anticoagulant factors
Elevated INR
± coagulopathy
Impaired metabolism of waste products and toxins
Toxins (mainly ammonia) accumulate and cross the blood- brain barrier
Hepatic encephalopathy
Day-night reversal, asterixis, delirium
Varices
(dilated veins in the esophagus, stomach, or rectum)
Variceal bleed
GI bleed and hypovolemia
Backflow of blood into spleen
Splenomegaly
Enlarged spleen sequesters (traps) blood cells
Cytopenias
(eg. thrombocytopenia or anemia), petechiae, easy bruising
↓ Blood flow to kidneys, which sense ↓ effective blood volume
Kidneys retain water and Na+
↑ Hydrostatic pressure in splanchnic vessels
↓ Albumin synthesis
↓ Capillary oncotic pressure
Net fluid flux out of vasculature into interstitial space
Ascites
(fluid in peritoneal cavity)
Peripheral edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 7, 2022, updated November 6, 2022 on www.thecalgaryguide.com")
Non-Alcoholic Fatty Liver Disease
)
Steatohepatitis: chronic inflammatory and apoptotic climate in the hepatocytes (in the absence of alcohol consumption, termed Non-Alcoholic Steatohepatitis (NASH))
Fibrosis of the Liver: excessive scarring of liver tissue resulting from chronic inflammation, although liver architecture is largely intact
Fat droplets form and grow in the hepatocytes
Hepatic mitochondria increase their workload in attempt to break down the excess free fatty acids through beta-oxidation
↑ in cellular workload creates more reactive oxygen speciesà Inflammation and apoptosis of hepatocytes
On-going inflammation damages hepatic stellate cells (the primary extracellular matrix–producing cells of the liver) causing the release of fibrinogenic cytokines
Cirrhosis of the liver: normal lobular structure distorts and is replaced by regenerating nodules and bridging septa, disrupting normal liver blood flow
Deposition of fibrotic
material and collagen within the perisinusoidal spaces of the liver
Decompensated Cirrhosis Hepatocellular carcinoma
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com")
Carbonic Anhydrase Inhibitor Diuretics

Inhibition of carbonic anhydrase on the apical surface of the brush border cells in the proximal convoluted tubule (PCT)
Activation of the Renin- Angiotensin-Aldosterone Systemfromvolume depletion
Activation of principle cell
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+ and waste K+
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical
Findings slide
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H2O available for excretion
Mild diuresis (increase in frequencyandvolumeof urine)
↓ Blood volume
Hypotension
↓ Na+ and HCO3- reabsorption in the PCT
↑ HCO3- delivery to cortical collecting duct
Urine alkalization (increased pH)
Chronic urine alkalization
↓Solubilityof citrate
↓ Urinary citrate
↓ Citrate binding with Ca2+à↑ Ca2+ complexing with oxalate
↑ Spontaneous nucleation, growth and agglomeration of calcium oxalate crystals
Formation of calcium oxalate renal calculi
↑ HCO3- is lost in the urine ↓ pH of the blood
Type II Renal Tubular Acidosis
See Type II/Proximal Renal Tubular Acidosis slide
CAI prevents the up- regulationofglutamine transporters in the PCT
Inability to correct the metabolic acidosis and impaired urinary NH3 excretion
Hyperammonemia (↑ serum NH3 )
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 3, 2024 on www.thecalgaryguide.com
Carbonic Anhydrase Inhibitor Diuretics: Renal Mechanism and Side Effects Carbonic Anhydrase Inhibitors (CAI)
Inhibition of carbonic anhydrase on the apical surface of the brush border cells of the proximal convoluted tubule (PCT)
Authors: Stephanie Happ Reviewers: Matt Hobart Name Name* * MD at time of publication
↓ Na+ and HCO3- reabsorption in the PCT
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H O available for 2
excretion
Mild diuresis
↓ Blood volume Hypotension
↑ HCO3- delivery to cortical collecting duct
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+
↑ Intracellular Na+ drives Na+/K+ ATPase activity on the principal cells (moving 2 K+ into cell and 3 Na+ out into the peritubular capillary)
↑ Intracellular K+ drives H+/K+ ATPase activity on the intercalated cells (moving 1 H+ into cell and 1 K+ out into the tubular filtrate)
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical Findings slide
Urine alkalization
↑ HCO3- is lost in the urine, leading to ↓ pH of the blood
Renal Tubular Acidosis Type II
See Type II/Proximal Renal Tubular Acidosis slide
CAI inhibit the up-regulation of glutamine transporters in the PCT
Inability to correct the metabolic acidosis and
impaired urinary NH3 excretion
Hyperammonemia
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Chronic urine alkalization leads to marked ↓ in urinary citrate
↓ Ability of citrate to bind to Ca2+ and calcium oxalate stones
↓ Inhibition of spontaneous nucleation
↓ Prevention of growth and agglomeration of crystals
Formation of calcium oxalate renal calculi
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com")
Gynecomastia

Hyperthyroidism
Klinefelter Syndrome (males with > 1 X chromosome)
Liver cirrhosis
Certain tumors (e.g., germ cell, adrenal, Leydig cell, Sertoli cell)
Anabolic steroid usage (containing testosterone)
Finasteride (treatment for benign prostate hyperplasia and male pattern baldness)
Cimetidine - inhibits stomach acid production
Spironolactone (diuretic
used to treat high blood pressure and heart failure)
Ketoconazole (antifungal)
Cytotoxic agents (e.g. alkylating agents, vincristine, methotrexate)
Imbalance between estrogens and androgens
Estrogen stimulates breast tissue growth in newborn
Changes in metabolic rate ↑ fat production
Unclear mechanism
↑ Proinflammatory mediators and cytokines (e.g. prostaglandin E2, TNF⍺, IL-1, IL-6, cyclooxygenase-2)
Prostaglandin E2 and IL- 6 upregulate aromatase enzyme expression
Available estrogen is higher than available testosterone
↑ Aromatase enzyme activity, converting androgens to estrogen
↓ Testosterone release from the testes
↓ Testosterone
↑ Serum sex hormone binding globulin (SHBG)
SHBG binds estrogen with less affinity to testosterone
Thyroid hormone stimulates liver to express more sex hormone binding globulin
Thyroid hormone stimulates aromatase activity
Overexpression of aromatase enzyme
Seminiferous tubules in the testes hyalinize and fibrose
Suppression of the hypothalamic pituitary thyroid axis through an unclear mechanism
Tumor may produce estradiol
Tumor produces β- human chorionic gonadotropin (β-HCG)
↑ serum testosterone
Inhibits 5-α reductase
Blocks binding of 5-DHT to androgen receptors
↓ 2-hydroxylation of estradiol
Mimics structures of testosterone
Inhibits 17,20 desmolase and 17α-hydroxylase
Damage to Leydig cells in testes
↑ Estrogen to androgen ratio
Pathological causes
Impaired spermatogenesis and testosterone production
↓ GnRH secretion from hypothalamus
↓ Testosterone
↓ Luteinizing hormone (LH) release from anterior pituitary
↓ 5-DHT and/or testosterone binding to androgen receptors in chest tissue
↓ inhibition of breast development
Normal or increased estrogen acts on estrogen receptor on chest tissue
Estrogen receptors stimulate breast development
Estradiol negatively feedbacks on luteinizing hormone
β-HCG stimulates LH receptors on Leydig cells in the testes
Aromatase enzyme converts excess testosterone into estrogen and estradiol
↓ conversion of testosterone to 5- dihydrotestosterone (5-DHT), a more potent form of testosterone
Glandular proliferation in male breasts
Gynecomastia
(development of breast tissue in males)
Drug side- effects
↓ Metabolism of estradiol
Competitively binds to androgen receptors
↑ Serum estradiol levels
Exhibits physical attributes that do not align with gender identity
Psychological distress
In some cases, hormones stabilize
Involution and atrophy of ducts
Gynecomastia resolves
↓ Steroid synthesis
↓ Androstenedione produced (testosterone precursors)
↓ Serum testosterone levels
↓ Testosterone production
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jun 9, 2024 on www.thecalgaryguide.com")
Underfill Edema Pathogenesis

Vasodilatory medications
Various mechanisms
Right-sided heart failure
Compromised right heart function ↓ forward flow
↓ Hepatic albumin synthesis
Blood is unable to pass through hepatic vessels disrupted by cirrhosis and backs up in portal vein
↑ Blood pressure in portal vein (portal hypertension)
Less blood volume in hepatic veins and vena cava (underfilling)
Pregnancy
↑ Estrogen, progesterone and relaxin
Vasodilation
Gravity causes fluid accumulation in peripheral veins
↑ Capillary hydrostatic pressure
↑ Net fluid movement into interstitial space
↓ Serum albumin
↓ Capillary oncotic pressure
Fluid extravasation into interstitial space
More blood in portal vein ↑ capillary hydrostatic pressure in venous system
Pressure creates net fluid
movement from vascular space into interstitial space
Less blood volume in arteries (underfilling)
↓ Effective arterial blood volume (EABV)
↓ Renal blood flow activates the renin-angiotensin-aldosterone system (RAAS)
Angiotensin and aldosterone ↑ Anti-diuretic hormone released by tubular Na+ and H2O resorption posterior pituitary ↑ H2O resorption
↑ Fluid in circulation, worsening existing venous congestion
↑ Hydrostatic capillary pressure and fluid extravasation into interstitial space Underfill edema (edema worsened by activation of RAAS)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 19, 2015; updated Aug 5, 2024 on www.thecalgaryguide.com")
Cystic Fibrosis

Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (transmembrane chloride ion
channel found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Pancreatic Manifestations
Trapped digestive
enzymes degrade
pancreatic tissue
Pancreatic tissue
damage triggers
inflammation,
scarring & fatty
tissue replacement
Islet cell damage
& destruction
Cystic-fibrosis related
diabetes (CFRD)
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
↓ Production & secretion of
pancreatic enzymes into GI
tract (pancreatic insufficiency)
Fat & protein malabsorption
Failure to
thrive
↓ Absorption of
fat-soluble vitamins
Steatorrhea
(↑ fat in stool)
Vitamin D
deficiency
Vitamin K
deficiency**
Rickets**
Osteoporosis**
Coagulopathies
Hepatic Manifestations
Delayed passage of bile
through biliary tree
↑ Loss of bile acids in stool
Inflammatory hepatic
response
↑ Production of lithogenic bile (bile
supersaturated with cholesterol)
Biliary cirrhosis with
portal hypertension
Cholelithiasis**
Gastrointestinal (GI) Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
**See corresponding Calgary Guide slide
Legend: Sign/Symptom/Lab Finding Complications
Pathophysiology Mechanism
Published Jan 21, 2013; updated Aug 20, 2025 on www.thecalgaryguide.com
Reproductive Manifestations
Degeneration of Wolffian duct derivatives
(vas deferens, epididymis, & seminal vesicles)
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Authors:
Navdeep Goraya, Spencer Montgomery
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Danielle Nelson*
*MD at time of publication
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Pancreatic Manifestations
Pancreas unable to
secrete digestive enzymes
into GI tract (pancreatic
insufficiency)
Fat & protein
malabsorption
↓ Absorption of
fat-soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage
triggers inflammation,
scarring & fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
Hepatic Manifestations
Delayed passage of bile
through biliary tree
Inflammatory hepatic
response
Cirrhosis** & portal
hypertension
Gastrointestinal Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
**See corresponding Calgary Guide slide
Published January 21, 2013 on www.thecalgaryguide.com
Please only review slide 1 – slides 3-7 are previous draft
versions.
Thank you!
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage triggers
inflammation, scarring
& fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas deferens
in utero
Retained secretions
in sinuses
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Accumulation of secretions in
secretory passages throughout the
body obstructing these passages
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Failure to clear
bacteria in
airways
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease i.e. lung
hyperinflation on x-ray & abnormal pulmonary
function tests
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion channel that is found in
exocrine tissue) dysfunction
Chloride channel no longer allows Cl- transport
CFTR proteins in
sweat glands reabsorb
Cl-
CFTR proteins in duct epithelial tissue of
other parts of the body facilitate diffusion
of Cl- into secretions
↓Reabsorption
↓Cl- diffusion into peri-ciliary fluid
↓Water composition of peri-ciliary fluid
↑Secretion of Cl-
into sweat
↓Clearance of mucociliary secretions
↑Sweat Cl-
concentration
Accumulation of secretions in secretory
passages throughout the body obstructing
these passages
Degeneration of vas deferens, Wolffian
ducts & associated structures
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Infertility in
affected males
In upper
respiratory
tract
Retained secretions
in sinuses
Nasal polyps
Bacterial
proliferation
Chronic
sinusitis
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Signs of obstructive lung disease
i.e. lung hyperinflation on x-ray &
abnormal pulmonary function
tests
Airway
infection &
inflammation
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓Movement
of intestinal
contents
In children/adults: Distal ileal obstruction
syndrome (DIOS)
In
newborns:
Meconium
ileus
↑Retention
of meconium
↑Reabsorption
of bilirubin
Prolonged
jaundice
in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Degeneration of
vas deferens,
Wolffian ducts
and associated
structures
Infertility in
affected males
Legend: Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Mutation of Cystic Fibrosis Transmembrane Regulator (CFTR) gene on chromosome 7 à
Dysfunction of the CFTR protein (a transmembrane chloride ion channel that is found in exocrine tissue)
Author: Spencer Montgomery
Reviewers: Yan Yu, Kayla
Nelson, Mark Montgomery*
* MD at time of publication
Chloride channel no longer allows Cl- transport
In sweat glands, CFTR
proteins are
responsible for the
reabsorption of Cl-
In duct epithelial tissue of other parts of
the body, CFTR proteins facilitate diffusion
of Cl- into secretions
Notes:
• The CFTR mutation exhibits an autosomal recessive inheritance pattern
• > 1700 different CFTR gene mutations are identified, ∆F508 mutation accounts for
~67% of cases in Caucasians.
• Cystic fibrosis is diagnosed based presence of ↑ sweat chloride concentration,
disease causing CFTR mutations, & symptoms of ≥ 1 associated organ system
↓ Cl- diffusion into peri-ciliary fluid →
↓water composition of peri-ciliary fluid
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↓ reabsorption =
↑secretion of Cl-
into sweat
In GI
tract
↓movement
of intestinal
contents
↓ clearance of mucociliary secretions
In
newborns:
Meconium
ileus
↑ retention of
meconium → ↑
reabsorption of
bilirubin
Prolonged
jaundice in
neonates
↑ Sweat chloride
concentration
Accumulation of secretions in secretory
passages throughout the body,
obstructing these passages
In biliary
tree
Delayed passage of bile →
inflammatory hepatic response
Cirrhosis & portal
hypertension
In upper respiratory tract
In pancreas
Trapped digestive
enzymes degrade
pancreatic tissue
Nasal
polyps
Retained
secretions in
sinuses →
bacterial
proliferation
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and
protein mal-
absorption
↓ absorption of fat
soluble vitamins
Inflammation →
scarring & fatty
tissue infiltration
→ islet cell
destruction
Chronic
sinusitis
↓ serum Vit. D
Type II Diabetes
Mellitus
Failure to
thrive
Osteoporosis
Published January 21, 2013 on www.thecalgaryguide.com
In lower respiratory tract
Chronic
productive
cough
Retained secretions in airways → bacterial proliferation
à Airway infection & inflammation
Persistent respiratory tract infections
Can progress to chronic bronchitis ± bronchiectasis
(This is the biggest cause of death in CF)
Pathophysiology Signs of obstructive lung dx: i.e.
Lung hyperinflation (on x-ray),
Abnormal pulmonary function
tests
Mechanism
Sign/Symptom/Lab Finding Complications")
Childhood Immunization Schedule

Spores enter contaminated wounds &
bacteria produce tetanospasmin to
invade central nervous system (CNS)
Muscle rigidity spasms,
hyperreflexia, autonomic
dysfunction, laryngeal spasms
↑ Mortality from
respiratory
obstruction & failure
Bacteria attach to ciliated
respiratory epithelial cells &
release toxins
Prolonged paroxysmal cough,
inspiratory “whoop” sound, emesis,
apnea, cyanosis, leukocytosis
↑ Risk of
pneumonia, seizures
& encephalopathy
Virus invades oropharynx/GI tract &
replicates in lymphoid tissue before
hematogenous spread to motor neurons
↑ Risk of paralytic
poliomyelitis &
respiratory failure
Bacteria colonize the
nasopharynx & invade
the bloodstream & CNS
Virus invades hepatocytes
via specific receptors &
replicates within liver cells
Bacteria colonize the
nasopharynx & may invade the
lungs, bloodstream, or meninges
Virus invades mature
enterocytes in the
small intestine
Bacteria colonize the nasopharynx
& enter the bloodstream to cross
the blood–brain barrier
Virus invades respiratory
epithelium & spreads to regional
lymphoid tissue & bloodstream
Virus infects upper respiratory tract
(URT) & disseminates via viremia to
salivary glands & other organs
Virus invades URT &
enters the bloodstream &
regional lymphoid tissue
Virus infects URT &
lymphoid tissue before
invading neural tissue
Virus infects anogenital
& oropharyngeal basal
layer epithelium tissue
Influenza virus
Virus invades upper
& lower respiratory
epithelium
Severe acute respiratory
syndrome coronavirus 2
(SARS-CoV-2)**
Viral invasion of mucous
membranes & may invade
extrapulmonary tissues
Legend: Muscle weakness,
asymmetric reduction
in tone, quadriplegia
Fever, fatigue, shortness of breath,
nausea, emesis, headache, stiff neck,
altered mental status, otitis media**
Fatigue, anorexia, nausea,
jaundice, arthralgia, right
upper quadrant pain
Otitis media**, sinusitis,
pneumonia**, meningitis**,
bacteremia
Gastroenteritis with
emesis, fever, diarrhea,
malaise & dehydration
Fever, headache, neck
stiffness, altered level of
consciousness, purpuric rash
Koplik spots, conjunctivitis, fever,
rhinorrhea, cough, diarrhea, otitis
media, pneumonia
Parotitis, headache, fever, malaise,
sensorineural hearing loss, orchitis,
mastitis, oophoritis, pancreatitis
Fever, lymphadenopathy, rash,
congenital anomalies such as hearing
loss, cataracts & cardiac defects
↑ Mortality from
meningitis,
pneumonia & sepsis
↑ Risk of cirrhosis,
hepatic malignancy,
& liver failure
↑ Mortality from
respiratory, CNS &
cardiac dysfunction
↑ Mortality from
hypovolemic shock
& CNS infection
↑ Mortality from
sepsis, multiorgan
failure & necrosis
↑ Mortality from
pneumonia &
encephalitis
↑ Mortality
from meningitis
& encephalitis
↑ Mortality
from congenital
rubella
Vesicular & pruritic rash,
fever, malaise, pneumonia,
encephalitis, cellulitis
↑ Morbidity from necrotizing
fasciitis, CNS, soft tissue &
respiratory infections
Often asymptomatic, or
may present with painless
anogenital warts
↑ Risk of anogenital
& head & neck
malignancy
Fever, cough, myalgia, malaise,
cough, headache, emesis, diarrhea,
abdominal pain, febrile seizures
↑ Mortality from
widespread
multiorgan infection
Fever, cough, fatigue, shortness of
breath, anosmia, ageusia,
pneumonia, multiorgan dysfunction
↑ Mortality from
respiratory distress
& multiorgan failure
DTaP-IPV-Hib-HB vaccine
Given at 2, 4 & 6 months old
Protects against
diphtheria, Tetanus,
Pertussis, Polio,
Haemophilus influenzae
type B, & Hepatitis B
DTaP-IPV-Hib vaccine
Given at 18 months old
Protects against
diphtheria, Tetanus,
Pertussis, Polio, &
Haemophilus
influenzae type B
Pneumococcal conjugate vaccine
Given at 2, 4 & 12 months old (additional 4th dose given at
6 months if at ↑ risk of invasive pneumococcal disease)
Authors:
McKayla Kirkpatrick, Stacey Holbrook
Reviewers:
Merry Faye Graff, Emily J. Doucette, Charissa
Chen, Amanda Ang, Danielle Nelson*
* MD at time of publication
Tdap-IPV vaccine
Given at 4 years old
Tdap vaccine
Given in Grade 9
Protects against
diphtheria, Tetanus,
Pertussis, & Polio
Protects against
diphtheria, Tetanus,
& Pertussis
HB vaccine
Given in Grade 6
Protects against
Hepatitis B virus
Protects against
Streptococcus pneumoniae
Rotavirus vaccine
Given at 2 & 4 months old
Protects against rotavirus
Meningococcal conjugate (MenconC)
Given at 4 & 12 months old
MenC-ACYW
(Meningococcal type A,
C, Y, W-135) in Grade 9
Protects against
Neisseria meningitidis
MMR-Var vaccine (e.g., Priorix-Tetra)
Given at 12 & 18 months old
Protects against measles,
mumps, rubella & varicella
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
HPV vaccine
Given in Grade 6 (2-3 doses over 6 months)
Seasonal influenza vaccine
Given annually starting at 6 months or older
COVID-19 vaccine
Given at 6 months or older Published Aug 19, 2015; updated Dec 31, 2025 on www.thecalgaryguide.com
Protects against HPV
Protects against influenza viruses
predicted to circulate each fall & winter
Protects against SARS-CoV2")
Sirosis patogenesis dan komplikasi
