SEARCH RESULTS FOR: Hyperthyroidism
Clinical Findings of Androgen Deficiency
![Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Clinical-Findings-of-Androgen-Deficiency.jpg "Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words")
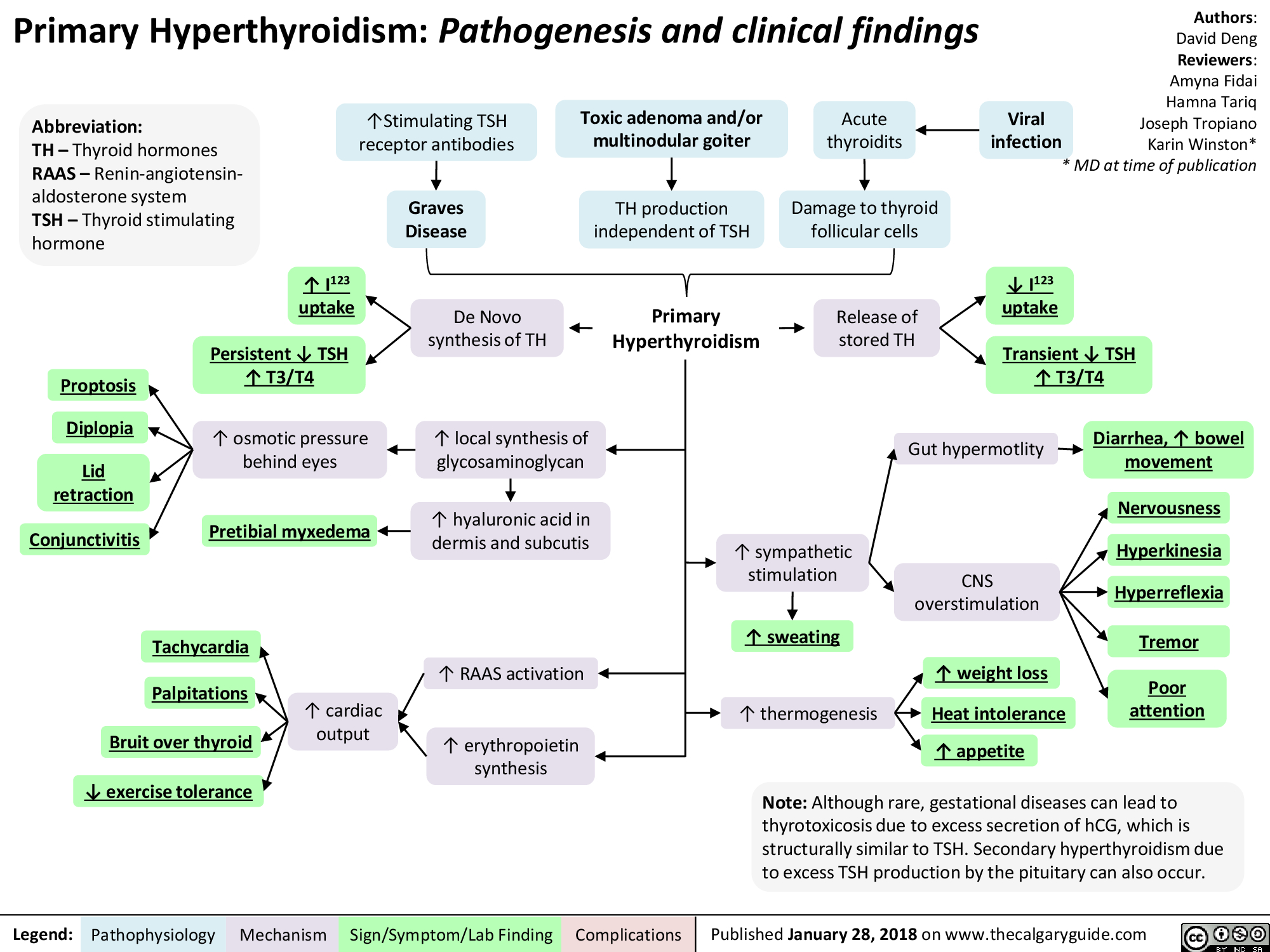
Hyperthyroidism

Hyperthyroidism
Erectile Dysfunction: Pathogenesis

1. Assess CVD Disease risk* a. I% Blood pressure b. I% Fasting glucose or HbA1c c. TG's & cholesterol 1. Penile duplex sonography 2. Cavernosometry
Legend:
Endocrinologic Erectile Dysfunction
Hypogonadism, hyperprolactinemia, hyperthyroidism, alcoholism, iatrogenic
.J, circulating free testosterone
•
1. 4, 7 AM free testosterone* 2. l• Thyroid Stimulating Hormone 3. l• Prolactin 4. l• Follicle Stimulating Hormone 5. l• Luteinizing Hormone
4, release of NO and cGMP levels within corpora cavernosa and smooth muscle relaxation
Pathophysiology Mechanism
Neurogenic Erectile Dysfunction
Neurologic disease, trauma, iatrogenic, diabetes mellitus
Central (cerebral or spinal cord); peripheral (afferent/sensory neuropathy) or efferent (autonomic neuropathy)
4, parasympathetic nerve firing
4, NO release
Psychogenic Erectile Dysfunction
•
Sudden onset, sporadic (circumstantial), younger, nocturnal/AM erection present
•
Anxiety, depression, strained relationship, lack of sexual arousal, psychological disorder
Possible mechanisms include an imbalance of central neurotransmitters, over inhibition of spinal erection center by the brain, and sympathetic overactivity
1. Abnormal Nocturnal penile 1. Normal Nocturnal penile tumescence and rigidity* tumescence and rigidity*
Erectile Dysfunction -• (persistent or recurrent inability to achieve an erection sufficient to achieve desired sexual performance)
Sign/Symptoni/Lab Finding
Complications
Authors: Braden Milian Reviewers: Alex Tang Usama Malik Jay C. Lee* * MD at time of publication")
Nodule-thyroïdien
 thyroïdien(s) hyperfonctionnel(s): Pathogénie et résultats cliniques
Traduction:
Radiation Tabagisme
↑ Âge Génétiques
Brianna Ghali Philippe Couillard* Autheur: Jaye Platnich Rédacteurs: Amogh Agrawal Alexander Arnold Hanan Bassyouni* *MD au moment de publication
ADN endommagée et mutée
La mutation du récepteur de la TSH dans le tissu thyroïdien entraîne une activation constitutive
(une activation indépendante de la TSH)
↑ Signalisation de la protéine G (spécifiquement Gs alpha)
Le tissu thyroïdien affecté devient hyperfonctionnel et
indépendant des mécanismes normaux de la régulation.
↑ Production et sécrétion de T4 et T3 à partir du nodule hyperfonctionnel.
↑ T4/T3 supprime la production de TSH par la glande pituitaire
Abbréviations:
• TSH - Hormone de stimulation de la thyroïde
Note: Les nodules thyroïdiens hyperfonctionnels sont très rarement malins : plus de 98 % de ces nodules sont bénins. La capacité à capter l'iode et à produire de la T4 et de la T3 suggère un niveau de différenciation cellulaire rarement atteint par les cellules malignes.
Prolifération localisée des cellules folliculaires de la thyroïde.
↑ Capture de l'iode radioactif et du technitium-99 par le tissu thyroïdien hyperfonctionnel.
Variety of mechanisms (see hyperthyroidism slide)
↓ Stimulation du tissu thyroïdien normal par la TSH
Nodule(s) palpable(s) sur la glande thyroïde
Captation de l'iode radioactif montre une ↑ quantitative de l'activité thyroïdienne.
La scintigraphie thyroïdienne au technitium 99 permet de visualiser qualitativement le ou les nodules hyperactifs (")
Osteoporosis Pathogenesis and risk factors
.
Secondary Osteoporosis
Smoking, alcohol, ↓ exercise, chronic malnutrition, hyperthyroidism, hyperparathyroidism, corticosteroid use, ↓ vitamin D, bone malignancies, chronic kidney or liver disease, and malabsorption.
Reduced peak bone mass achieved during skeletal growth and/or an imbalance in the factors favoring bone resorption compared to bone formation in adult bone
↓ Serum vitamin D from malabsorption, poor nutrition, or chronic liver/ kidney disease
↓ Serum activated vitamin D (precursor for Ca2+ transporters in the gut)
↓ Ca2+ absorption from gut
↓ Ca2+ available for mineralization of bone matrix
Age related bone degeneration and ↓ exercise
↑ Reactive oxygen species (ROS) systemically
due to aging
↑ Oxidative stress on bone
↑ Osteocyte death in cortical bones
↓ Bone Formation
↓ Estrogen
in post-menopausal women
Hyperparathyroidism/ bone malignanciesà ↑ parathyroid hormone (PTH) or parathyroid hormone-related (PTHR) protein released
↑ PTH and PTHR peptide receptor signaling in osteocytes results in ↓ osteoprotegerin (OPG) expression
↓ OPG secretion
Hyperthyroidism à↑ T3 and T4
↑ Thyroid receptor- alpha-1 activation (located in bones)
↑ Osteoclasts (cells that break down bone)
↑ Bone Resorption
Corticosteroid use
↑ Corticosteroid binding to glucocorticoid receptors on bone suppresses OPG
expression in bone
Smoking
Multiple mechanisms (e.g. ↓ blood supply to bone, ↑ free radicals, direct effects on RANKL/RANK/ OPG bone remodeling axis leading to alterations in osteogenesis
↑ Bone Resorption and ↓ Bone Formation
Abbreviations:
• T3 - Triiodothronine • T4 - Thyroxine
↓ Stimulation of OPG transcription in osteoblasts
Authors: Ben Wajda, Arsalan Ahmad, Lance Bartel Reviewers: Alyssa Federico, Mehul Gupta,
Tara Shannon, Reza Ojaghi, Usama Malik,
Carol Hutchinson*, David Hogan*
* MD at time of publication
↓ Inhibition of receptor activator of nuclear factor kappa-B ligand (RANKL) (receptor that stimulates osteoclast growth)
Osteoporosis: Imbalance of bone formation and resorption leading to decreased bone mineral density and bone mass, or quality changes that lead to a decrease in bone strength and an increase risk of fractures
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 20, 2022 on www.thecalgaryguide.com")
hypercalcemia-pathogenesis

Ectopic (outside of kidney) production of 1-α-hydroxylase
1-α-hydroxylase converts calcidiol to calcitriol (aka 1,25-OH Vitamin D or active Vitamin D)
↑ 1-25 OH Vitamin D
↑ Absorption of Ca2+ in the small intestine
↑ Vitamin D Intake
Dietary Vitamin D is converted to calcidiol (aka 25- OH Vitamin D or inactive Vitamin D) in the liver
Primary Hyperparathyroidism
↑ or normal* serum parathyroid hormone (PTH) level
Tumour released Parathyroid Hormone related Peptide (PTHrP) mimics natural PTH (PTH level itself is low)
Tumour produces bone- reabsorbing substances (IL-6, IL-1, RANKL)
Paget’s Disease
Osteoblasts produce abnormally high levels of RANKL
Block Na+/Cl- cotransporter (NCC) on distal convoluted tubule (DCT) cells of the nephron
↓ Na+ and Cl- transport from lumen into DCT cells
↓ Intracellular Na+ in DCT cells
+ To compensate Na ,
↑ Ca-ATPase and 3:Na:Ca exchanger activity on DCT cells (moves 3 Na+ into cell, 1 Ca+ out into peritubular capillary)
↑ Ca+ moving into bloodstream
↓ Mechanical stimulation of osteocytes
↓ Signaling of osteoblasts (cells that form bone)
↓ New bone formation
↓ Ca2+ incorporation
into bone
↑ Ca2+ in plasma
↑ reabsorption of Ca2+ from the distal portion of nephron back into the blood
↑ 1-α-hydroxylase production in the proximal convoluted tubule
Milk Alkali Syndrome
Ca2+ intake exceeding 2000 mg per day leads to unregulated gut Ca2+ absorption into the blood
PTH binds to osteoblasts on the surface of bone
Osteoblasts produce RANKL to stimulate osteoclast function
↑ Osteoclast (cells that breakdown bone) activity
↑ Bone breakdown
Ca2+ within bone is released into the bloodstream
Osteolytic bone metastases
Hyperthyroidism
↑ Catabolic thyroid hormones
↑ RANKL: OP ratio, RANKL promotes bone breakdown by stimulating osteoclast growth while OP (osteogenic protein) promotes bone formation
Hypercalcemia Hypercalcemia
Authors: Alexander Arnold, Peter Vetere, Huneza Nadeem Reviewers: Mark Elliott, Ran (Marissa) Zhang, Yan Yu*, Hanan Bassyouni* * MD at time of publication
See Hypercalcemia: Clinical Findings slide
*Note: A normal PTH value is abnormal in the context of hypercalcemia, since hypercalcemia would normally negatively feed back to suppress PTH production.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 11, 2014, updated Aug 11, 2022 on www.thecalgaryguide.com")
Gynecomastia

Hyperthyroidism
Klinefelter Syndrome (males with > 1 X chromosome)
Liver cirrhosis
Certain tumors (e.g., germ cell, adrenal, Leydig cell, Sertoli cell)
Anabolic steroid usage (containing testosterone)
Finasteride (treatment for benign prostate hyperplasia and male pattern baldness)
Cimetidine - inhibits stomach acid production
Spironolactone (diuretic
used to treat high blood pressure and heart failure)
Ketoconazole (antifungal)
Cytotoxic agents (e.g. alkylating agents, vincristine, methotrexate)
Imbalance between estrogens and androgens
Estrogen stimulates breast tissue growth in newborn
Changes in metabolic rate ↑ fat production
Unclear mechanism
↑ Proinflammatory mediators and cytokines (e.g. prostaglandin E2, TNF⍺, IL-1, IL-6, cyclooxygenase-2)
Prostaglandin E2 and IL- 6 upregulate aromatase enzyme expression
Available estrogen is higher than available testosterone
↑ Aromatase enzyme activity, converting androgens to estrogen
↓ Testosterone release from the testes
↓ Testosterone
↑ Serum sex hormone binding globulin (SHBG)
SHBG binds estrogen with less affinity to testosterone
Thyroid hormone stimulates liver to express more sex hormone binding globulin
Thyroid hormone stimulates aromatase activity
Overexpression of aromatase enzyme
Seminiferous tubules in the testes hyalinize and fibrose
Suppression of the hypothalamic pituitary thyroid axis through an unclear mechanism
Tumor may produce estradiol
Tumor produces β- human chorionic gonadotropin (β-HCG)
↑ serum testosterone
Inhibits 5-α reductase
Blocks binding of 5-DHT to androgen receptors
↓ 2-hydroxylation of estradiol
Mimics structures of testosterone
Inhibits 17,20 desmolase and 17α-hydroxylase
Damage to Leydig cells in testes
↑ Estrogen to androgen ratio
Pathological causes
Impaired spermatogenesis and testosterone production
↓ GnRH secretion from hypothalamus
↓ Testosterone
↓ Luteinizing hormone (LH) release from anterior pituitary
↓ 5-DHT and/or testosterone binding to androgen receptors in chest tissue
↓ inhibition of breast development
Normal or increased estrogen acts on estrogen receptor on chest tissue
Estrogen receptors stimulate breast development
Estradiol negatively feedbacks on luteinizing hormone
β-HCG stimulates LH receptors on Leydig cells in the testes
Aromatase enzyme converts excess testosterone into estrogen and estradiol
↓ conversion of testosterone to 5- dihydrotestosterone (5-DHT), a more potent form of testosterone
Glandular proliferation in male breasts
Gynecomastia
(development of breast tissue in males)
Drug side- effects
↓ Metabolism of estradiol
Competitively binds to androgen receptors
↑ Serum estradiol levels
Exhibits physical attributes that do not align with gender identity
Psychological distress
In some cases, hormones stabilize
Involution and atrophy of ducts
Gynecomastia resolves
↓ Steroid synthesis
↓ Androstenedione produced (testosterone precursors)
↓ Serum testosterone levels
↓ Testosterone production
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jun 9, 2024 on www.thecalgaryguide.com")
Hyperthyroidism in Pregnancy
 hormone stimulates TSH receptors which ↑T3/T4 & ↓ physiologic TSH production in 1st trimester & normalizes in 2nd trimester
Transient hyperthyroxinemia in pregnancy (often benign)
Autoantibodies ↑ stimulation of thyroid stimulating hormone (TSH) receptors
Transplacental passage of TSH- receptor antibodies (can occur with normal thyroid function)
Graves’ disease
Transient ↓TSH & ↑T3/T4
Persistent ↓TSH & ↑T3/T4
Low birth weight Maternal congestive heart failure Pre-eclampsia (high blood pressure in
pregnancy)
Thyroid storm (excessive release of T3/T4 leading to a life-threatening hypermetabolic state)
↑ Triiodothyronine (T3) & thyroxine (T4) production independent of TSH
Abnormal differentiation of trophoblast embryonic cells ↑ hCG levels (cells that provide nutrition to the embryo)
Gestational trophoblastic disease
Toxic multinodular goiter
Toxic adenoma
Viral infection
Subacute thyroiditis (thyroid inflammation)
Hyperthyroidism in Pregnancy
Anterior pituitary gland releases stored TSH
↑Sympathetic nervous system stimulation
↑Thermogenesis
(heat production, regulated by thyroid & variousbraincentres)
↑Hyaluronic acid in dermis & subcutis tissue of the skin (Graves’ disease specific)
Transplacental passage of ↑T3/T4 to fetus
Gut hypermobility
Central nervous system overstimulation
↑Weight loss ↑Appetite
Heat intolerance
Diarrhea & ↑ bowel movements
Nervousness & anxiety
Hyperkinesia (excessive activity of a body part)
Hyperreflexia (overactive muscle reflex response)
Tremor
Poor attention span
↑ Heart rate
Palpitations (noticeable abnormal heartbeats)
Bruit (turbulent blood flow) heard over thyroid
↓ Exercise tolerance
↑ Cardiac output
De novo synthesis of TSH (synthesis of TSH independent of normal regulatory signals & processes as seen in toxic adenoma & toxic multinodular goiter)
Pregnancy Complications (abnormallyhighfreeT4&thyroid stimulating antibodies in the blood impacts fetal thyroid function)
↑ Renin angiotensin aldosterone system (RAAS) activation (important regulator of electrolytes, blood volume, & systemic vascular resistance)
↑ Erythropoietin (EPO, hormone made by kidneys that
stimulates red blood cell production)
Pretibial myxedema (condition causing skin lesions from deposition of hyaluronic acid)
Spontaneous abortion (pregnancy loss naturally ≤20 weeks gestation)
Premature labour (labour ≤37 weeks gestation)
Stillbirth (fetal death >20 weeks gestation)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 29, 2024 on www.thecalgaryguide.com")
Bone Remodeling Physiology
 activity, ↑ osteoclast (bone cells that break down bone) activity
Hyperparathyroidism ↓ Blood Ca2+
↑ Parathyroid hormone (serum Ca2+ concentration increasing hormone)
Trauma
Osteoblasts detect breach in matrix integrity
Hyperthyroidism
↑ Triiodothyronine (T3)
↑ Bone turnover
Puberty
↑ Growth hormone
↑ Blood calcium (Ca2+)
↑ Calcitonin
(reduces serum Ca2+ by ↓ renal Ca2+ reabsorption & ↑ osteoclast activity)
Net bone resorption process (bone tissue released from bones)
Surveillance osteoblasts produce receptor activator of nuclear activator kappa beta (RANKL; osteoclast stimulating protein)
Monocytes fuse into osteoclasts (cells for bone breakdown)
Osteoclast actions
Secrete HCl to dissolve hydroxyapatite (bone matrix forming inorganic mineral)
Serum markers of bone resorption: C-Telopeptide (CTX) P-Telopeptide (PTX)
Net bone formation process
Hormones activate osteoblast
Osteoblast actions
Secrete osteoprotegerin that binds RANKL
Secrete osteoid seam (a new layer of unmineralized organic bone matrix)
Osteoblasts deposit hydroxyapatite on seam
Phagocytose osteocytes within bone matrix
Authors: Andrew Wu, Jason Kreutz Reviewers:Mizuki Lopez,
Gurreet Bhandal, Luiza Radu *Samuel Fineblit
* MD at time of publication
Secrete collagenase enzyme to help digest collagen
↓ Osteoclast activity
Osteoblasts become osteocytes (mature cells) within bone
Serum markers of bone formation:
↑ Alkaline phosphatase (ALP)
↑ Bone-specific alkaline phosphatase (BSAP; an enzyme produced by osteoblasts during mineralization of bone)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")
Chronic Hypertensive Retinopathy

2o Hypertension risk factors (ex. Cushing’s Syndrome**,
hypothyroidism**, hyperthyroidism**, acromegaly, diabetes mellitus**)
Ophthalmic Artery Hypertension (HTN)
↑ Blood pressure in the ophthalmic artery
(branch of the internal carotid artery)
Persistent ↑ systemic blood pressure
Authors:
Emily J. Doucette,
Kareem Sadek,
Graeme Prosperi-Porta
Reviewers:
Stephanie Cote,
Usama Malik,
Johnathan Wong*,
Mary Holdsworth*
* MD at time of publication
Stage 1:
Mild/vasoconstrictive
Stage 2:
Moderate/sclerotic
Stage 3:
Severe/exudative
Focal arteriole weakening
from chronic HTN
Retinal arterial macroaneurysm
(risk of hemorrhage or exudation)
Acute & chronic vasospasms
↑ vasomotor tone
Generalized arterial narrowing
& vascular tortuosity
Retinal arteriolar sclerosis
& thickening at arteriole-
venule crossings
Arteriovenous nicking (venule
compressed by arteriole)
Branch retinal vein occlusion (sectoral
hemorrhages & macular edema)
Central retinal artery
occlusion (CRAO)**
Copper wiring (reflected
light appears red-brown)
Chronic retinal hypoperfusion
(progressive vision loss)
Persistent HTN causes
arteriolar wall
thickening, hyaline
arteriosclerosis, &
atherosclerotic changes
Central retinal vein
occlusion (CRVO)**
Fragile microaneurysms or sclerotic
vessels rupture into vitreous cavity
Floaters & sudden
painless vision loss
Vitreous hemorrhage
Branch retinal artery
occlusion (partial vision
loss & retinal pallor)
Arteriolar changes ↑ risk of vessel occlusion
Terminal retinal
arteriole occlusion
Focal ischemia of nerve
fiber layer of retina
Cotton-wool spots (fluffy white
ischemic lesions on fundus exam)
Dot-blot & flame retinal hemorrhages
(inner retina & nerve fiber layer)
Chronic HTN results in endothelial
dysfunction & vascular leakage
Damaged blood-retinal barrier
breaks down, leaking whole
blood, serum proteins, & lipids
Extrusion of a fibrin
plug at site of rupture
Roth spots (white-centered
retinal hemorrhages)
Retinal detachment (retina
separates from pigment epithelium)
Siegrist streaks (linear hyperpigmented
streaks overlying choroidal vessels)
Yellow hard exudates (lipid-
protein retinal deposits)
Hard exudates
align radially
with nerve fiber
orientation
Retinal pigment epithelium clumps
around atrophic areas in the choroid
Elschnig’s spots (hyperpigmented patches
surrounded by a hypo-pigmented ring)
“Macular star”
pattern
Optic disc edema & disc pallor
Chronic optic neuropathy (irreversible
vision loss with optic nerve atrophy)
Published Jun 28, 2017; updated Feb 17 2026 on www.thecalgaryguide.com
Mechanism Complications")