SEARCH RESULTS FOR: Cystic-Fibrosis
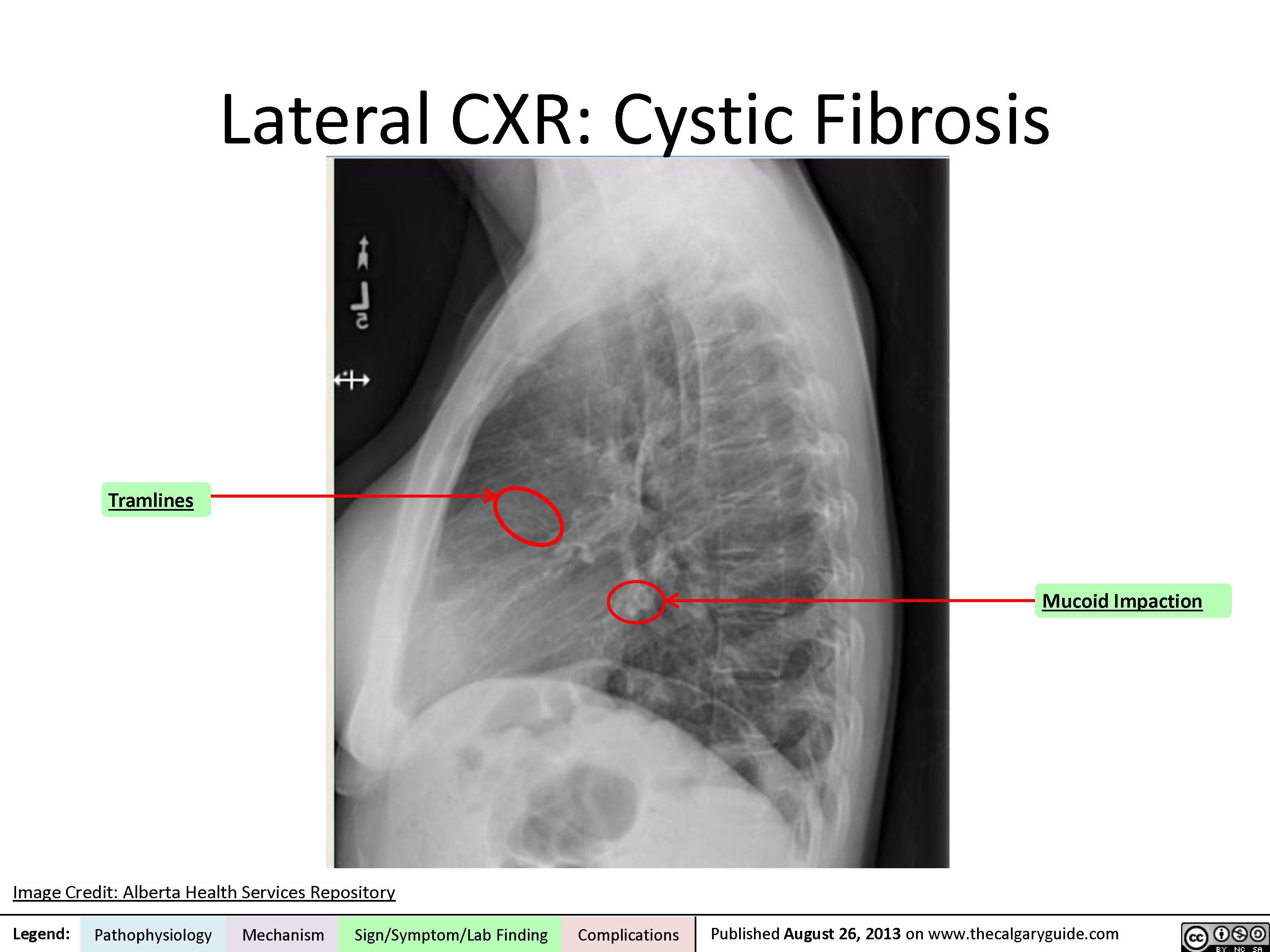
Lateral Chest X-Ray
Coronal CT
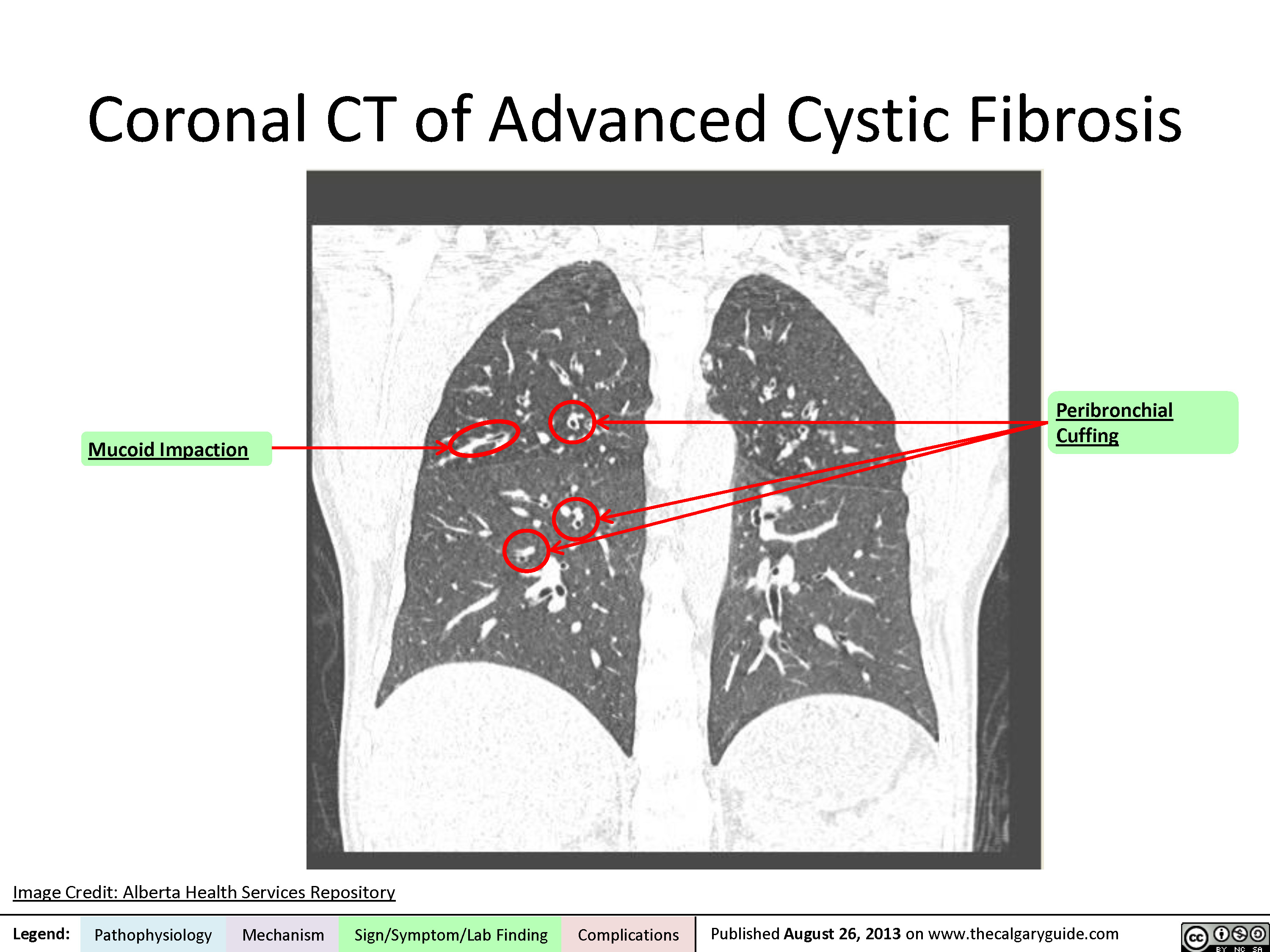
cystic-fibrosis-findings-on-chest-x-ray-and-lung-window-ct-scan
, Mark Montgomery* * MD at time of publication
Collapsed alveoli appears white on x-ray
Peribronchial Cuffing
secretions become more viscous. (See relevant slide for CF pathogenesis.)
As early as at birth, secretions collect in bronchial lumen, delaying mucociliary clearance
Mucus plugs and obstructs bronchial lumen
Air trapped distal to obstruction and cannot leave lungs
Lung Hyperinflation
Diaphragm domes below 10th posterior rib and 6th anterior rib on PA CXR
Flattened hemidiaphragm, enlarged retrosternal space on lateral CXR
With time, pulmonary capillaries gradually absorb gases in alveoli distal to obstruction àalveolar collapse (Atelectasis)
Collapsed alveoli more solid and radiodense than airà↓X-ray penetration
Adjacent structures may shift towards atelectasis on CXR
In first few years of life, retained bronchial secretions serve as nidus for recurrent bacterial colonization and infection
Late findings at 10- 30 years oldà secretion accumulation blocks inhaled air to affected lung segments àchronic hypoxia
Inflammatory response (cytokines, nitric oxide and radical oxygen species) leads to bronchial and peribronchial destruction
Hypoxia induces pulmonary capillary vasoconstriction
Some airways are blocked more than others
Leakage of fluid into bronchial walls & peri- bronchial regions.
Inflammatory cytokines destroy elastic components of bronchi
Accumulation of inflammatory exudate in bronchi
Pulmonary artery hypertension à Blood backs up in pulmonary arteries
Some segments of lung underventilated
Fluid around bronchial walls is more radiodense than air à↓X-ray penetration àappears white
Bronchiectasis: dilated, thickened, untapered bronchi on CXR/CT
Fluid/mucus in bronchi is more radiodense than air, thus appearing white on imaging
Edematous bronchi viewed end on are thickened and appear ring-like on CT/CXR
Tramlines (AKA Tramtracking)
Bronchus wider than corresponding blood vessel on CXR/CT
Advanced bronchiectasis is saccular in appearance
Mucus-filled bronchi form tubular opacities giving appearance of white fingers on CXR/CT
Signet Ring Sign
Bronchiectatic Cavities
Mucoid Impaction (AKA Finger in glove sign)
↑ Blood dilates pulmonary arteries
Blood backs up in right ventricle, dilating it
Pulmonary arteries look wider on CXR.
Main pulmonary artery >30 mm diameter on CT
Right Ventricle Enlargement on CXR/CT
Underventilated lung segments appear as lower intensity (darker) than normal ventilated segments which appear as normal intensity (brighter)
Mosaic Changes on CT(non- contrast
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 13, 2013, updated Aug 18, 2021 on www.thecalgaryguide.com")
囊性纤维化-发病机理临床表现及并发症
基因突变à
囊性纤维化跨膜传导调节( CFTR )蛋白 (一种表达在外分泌组织中的氯离子通道蛋白)功能紊乱
作者: Spencer Montgomery
审稿人: Yan Yu, Kayla Nelson, Mark Montgomery*
译者: Huiting Wang (王慧婷), Yang Xiang (向阳)
翻译审稿人:Ran zhong (钟然),
Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) *发表时担任临床医生
异常氯离子通道蛋白影响Cl-跨膜运输
注意:
• CFTR突变呈常染色体隐性遗传
• 已知有> 1700种不同CFTR基因突变类型, ∆F508突变占了高加索人群发病总
数的67%
• 囊性纤维化的诊断依据:汗液氯离子浓度↑, CFTR基因突变 & ≥1个相关内
在汗腺中, CFTR蛋白主要 功能为Cl-重吸收
重吸收↓ =汗 液中Cl- 浓度↑
汗液中Cl- 浓度↑
在母体 子宫内 输精管
中肾管、输精
管及相关结构
退行性变
男性不育
在身体其他部位的管道上皮组织中, CFTR蛋白促进 Cl- 扩散到分泌物中
外周纤毛液体层Cl- ↓ → 外周纤毛液 体层的含水量↓
黏液-纤毛系统清除分泌物↓ 分泌物异常聚集并阻塞全身各处的
分泌管腔
下呼吸道
脏有器官系统的 临床症状
儿童/成人: 远端肠梗阻综合征(DIOS)
胃肠道
胆道系统
鼻息肉
胃肠道内容
物蠕动↓ 新生儿:
胎粪性 肠梗阻
胎粪潴留↑→
肝硬化 & 门静脉高压
新生儿黄疸 胆红素重吸收↑ 时间延长
胆汁排出延迟 →肝炎症反应 上呼吸道 胰腺
淤积在胰腺内
的消化酶消化 胰腺自身
炎症 ;瘢痕增生 & 脂肪组织渗 透 ; 胰岛细胞 受损
II型糖尿病
慢性湿咳
诊断肺部阻塞标志: i.e. 肺过度充气(X线), 肺功能检测异常
鼻窦内分泌
胰腺分泌的消化酶无法进入 物潴留 → 细 胃肠道中 (胰液不足)
分泌物在气道内潴留→ 细菌增殖à 气道感染 & 炎症 持续呼吸道感染可进展为慢性支气管炎
± 支气管扩张(囊性纤维化最主要的死亡原因)
菌增殖
慢性鼻窦炎
脂质和蛋白 脂溶性维生素吸收 质吸收不良 ↓
发育不良
血清Vit. D ↓ 骨质疏松症
图注:
病理生理
机制
体征/症状/实验室检查
并发症
2013年1月21日发布于 www.thecalgaryguide.com")
囊性纤维化-胸部-x-线和肺窗-ct-扫描结果

Zystische Fibrose: Pathogenese, klinische Befunde und Komplikationen

Cystic Fibrosis

Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (transmembrane chloride ion
channel found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Pancreatic Manifestations
Trapped digestive
enzymes degrade
pancreatic tissue
Pancreatic tissue
damage triggers
inflammation,
scarring & fatty
tissue replacement
Islet cell damage
& destruction
Cystic-fibrosis related
diabetes (CFRD)
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
↓ Production & secretion of
pancreatic enzymes into GI
tract (pancreatic insufficiency)
Fat & protein malabsorption
Failure to
thrive
↓ Absorption of
fat-soluble vitamins
Steatorrhea
(↑ fat in stool)
Vitamin D
deficiency
Vitamin K
deficiency**
Rickets**
Osteoporosis**
Coagulopathies
Hepatic Manifestations
Delayed passage of bile
through biliary tree
↑ Loss of bile acids in stool
Inflammatory hepatic
response
↑ Production of lithogenic bile (bile
supersaturated with cholesterol)
Biliary cirrhosis with
portal hypertension
Cholelithiasis**
Gastrointestinal (GI) Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
**See corresponding Calgary Guide slide
Legend: Sign/Symptom/Lab Finding Complications
Pathophysiology Mechanism
Published Jan 21, 2013; updated Aug 20, 2025 on www.thecalgaryguide.com
Reproductive Manifestations
Degeneration of Wolffian duct derivatives
(vas deferens, epididymis, & seminal vesicles)
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Authors:
Navdeep Goraya, Spencer Montgomery
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Danielle Nelson*
*MD at time of publication
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Pancreatic Manifestations
Pancreas unable to
secrete digestive enzymes
into GI tract (pancreatic
insufficiency)
Fat & protein
malabsorption
↓ Absorption of
fat-soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage
triggers inflammation,
scarring & fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
Hepatic Manifestations
Delayed passage of bile
through biliary tree
Inflammatory hepatic
response
Cirrhosis** & portal
hypertension
Gastrointestinal Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
**See corresponding Calgary Guide slide
Published January 21, 2013 on www.thecalgaryguide.com
Please only review slide 1 – slides 3-7 are previous draft
versions.
Thank you!
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage triggers
inflammation, scarring
& fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas deferens
in utero
Retained secretions
in sinuses
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Accumulation of secretions in
secretory passages throughout the
body obstructing these passages
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Failure to clear
bacteria in
airways
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease i.e. lung
hyperinflation on x-ray & abnormal pulmonary
function tests
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion channel that is found in
exocrine tissue) dysfunction
Chloride channel no longer allows Cl- transport
CFTR proteins in
sweat glands reabsorb
Cl-
CFTR proteins in duct epithelial tissue of
other parts of the body facilitate diffusion
of Cl- into secretions
↓Reabsorption
↓Cl- diffusion into peri-ciliary fluid
↓Water composition of peri-ciliary fluid
↑Secretion of Cl-
into sweat
↓Clearance of mucociliary secretions
↑Sweat Cl-
concentration
Accumulation of secretions in secretory
passages throughout the body obstructing
these passages
Degeneration of vas deferens, Wolffian
ducts & associated structures
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Infertility in
affected males
In upper
respiratory
tract
Retained secretions
in sinuses
Nasal polyps
Bacterial
proliferation
Chronic
sinusitis
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Signs of obstructive lung disease
i.e. lung hyperinflation on x-ray &
abnormal pulmonary function
tests
Airway
infection &
inflammation
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓Movement
of intestinal
contents
In children/adults: Distal ileal obstruction
syndrome (DIOS)
In
newborns:
Meconium
ileus
↑Retention
of meconium
↑Reabsorption
of bilirubin
Prolonged
jaundice
in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Degeneration of
vas deferens,
Wolffian ducts
and associated
structures
Infertility in
affected males
Legend: Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Mutation of Cystic Fibrosis Transmembrane Regulator (CFTR) gene on chromosome 7 à
Dysfunction of the CFTR protein (a transmembrane chloride ion channel that is found in exocrine tissue)
Author: Spencer Montgomery
Reviewers: Yan Yu, Kayla
Nelson, Mark Montgomery*
* MD at time of publication
Chloride channel no longer allows Cl- transport
In sweat glands, CFTR
proteins are
responsible for the
reabsorption of Cl-
In duct epithelial tissue of other parts of
the body, CFTR proteins facilitate diffusion
of Cl- into secretions
Notes:
• The CFTR mutation exhibits an autosomal recessive inheritance pattern
• > 1700 different CFTR gene mutations are identified, ∆F508 mutation accounts for
~67% of cases in Caucasians.
• Cystic fibrosis is diagnosed based presence of ↑ sweat chloride concentration,
disease causing CFTR mutations, & symptoms of ≥ 1 associated organ system
↓ Cl- diffusion into peri-ciliary fluid →
↓water composition of peri-ciliary fluid
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↓ reabsorption =
↑secretion of Cl-
into sweat
In GI
tract
↓movement
of intestinal
contents
↓ clearance of mucociliary secretions
In
newborns:
Meconium
ileus
↑ retention of
meconium → ↑
reabsorption of
bilirubin
Prolonged
jaundice in
neonates
↑ Sweat chloride
concentration
Accumulation of secretions in secretory
passages throughout the body,
obstructing these passages
In biliary
tree
Delayed passage of bile →
inflammatory hepatic response
Cirrhosis & portal
hypertension
In upper respiratory tract
In pancreas
Trapped digestive
enzymes degrade
pancreatic tissue
Nasal
polyps
Retained
secretions in
sinuses →
bacterial
proliferation
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and
protein mal-
absorption
↓ absorption of fat
soluble vitamins
Inflammation →
scarring & fatty
tissue infiltration
→ islet cell
destruction
Chronic
sinusitis
↓ serum Vit. D
Type II Diabetes
Mellitus
Failure to
thrive
Osteoporosis
Published January 21, 2013 on www.thecalgaryguide.com
In lower respiratory tract
Chronic
productive
cough
Retained secretions in airways → bacterial proliferation
à Airway infection & inflammation
Persistent respiratory tract infections
Can progress to chronic bronchitis ± bronchiectasis
(This is the biggest cause of death in CF)
Pathophysiology Signs of obstructive lung dx: i.e.
Lung hyperinflation (on x-ray),
Abnormal pulmonary function
tests
Mechanism
Sign/Symptom/Lab Finding Complications")