SEARCH RESULTS FOR: tamponade
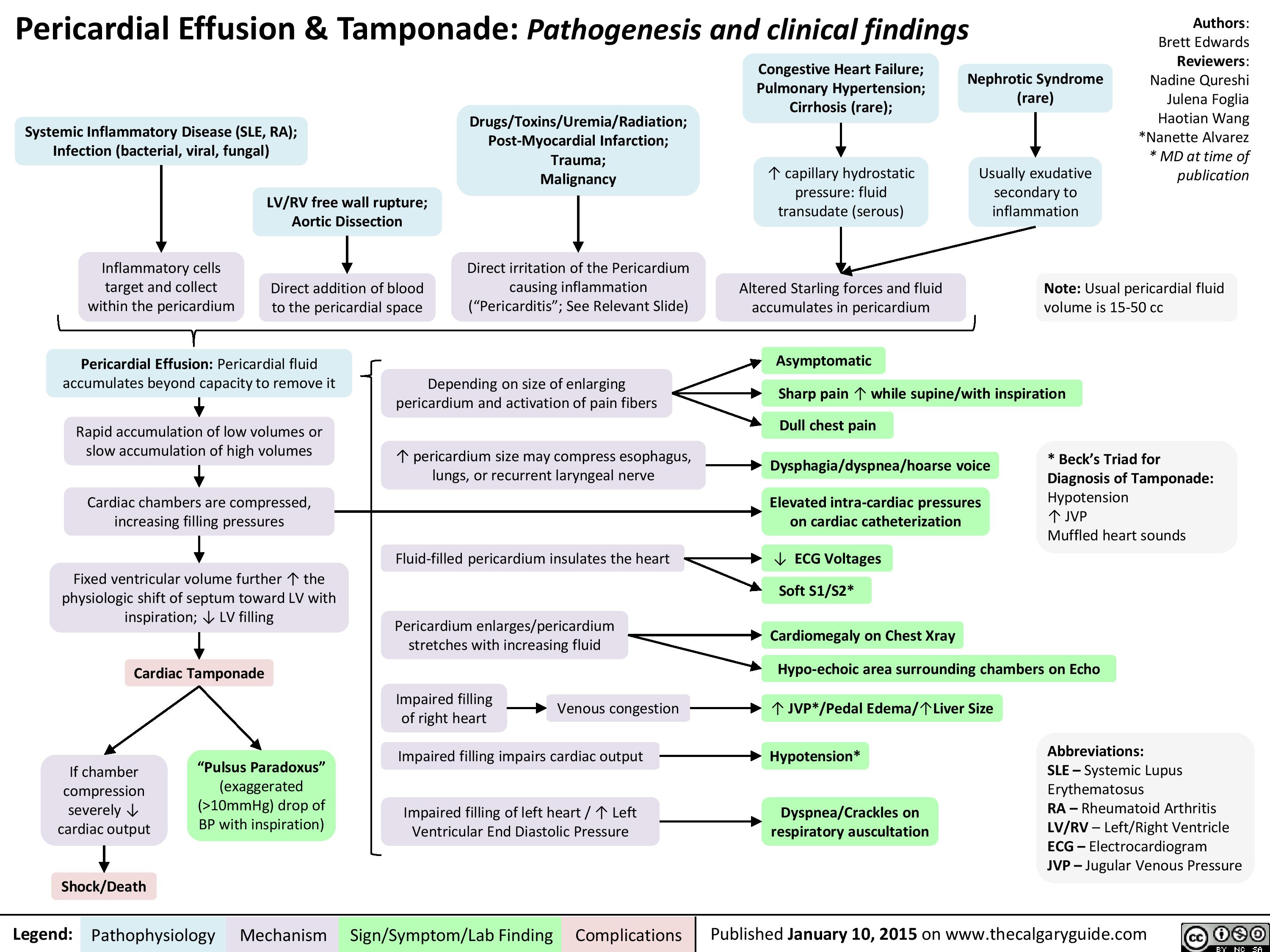
Pericardial Effusion and Tamponade: Pathogenesis and Clinical Findings
jvp-kussmals-sign-explained
: Kussmal's Sign explainedExcessive pericardial fluid compresses heart walls on all sidesLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publication? Right ventricle wall complianceConstrictive pericarditisRight ventricle prevented from fully expanding ? ability of the right ventricle to accommodate higher venous returnBackup of venous blood into right atrium and preceding internal jugular veinsRestrictive cardiomyopathyInflamed, fibrotic pericardium restricts expansion of heartRight ventricle myocardial infarct Cardiac tamponade (rare)InspirationMore venous blood tries to enter the low-pressure thoracic cavity via the right ventricle? pressure in thoracic cavity
JVP should return to normal within 3 respiration cyclesJugular Venous Pressure (JVP): Physical Exam FeaturesExerts less force against vesselsTilting the head of the bed:Low pressure, & the thinner walls of the internal jugular veins, are less able to keep lumen open when compressedLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publicationBlood in internal jugulars settles to bottom of the vein (analogy: half-full tube of water is turned vertically)Visible waves in the JVP correspond to stages of the cardiac cycleNon-palpableBiphasic waveform? JVP The Jugular Venous Pressure (JVP) Blood pressure in the internal jugular veinsV-waveA-waveRight atrial contractionBlood passively fills right atrium during ventricular systole? JVP? JVPIn: ? intrathoracic pressurePressing hard on abdomen (overlying the liver), or doing a valsalvaFacing lower afterload, Right heart more readily pumps blood into pulmonary circulation? abdominal pressure? venous blood forced up into right atriumVenous blood pressure is normally very lowOccludableNote: Since the internal jugular veins are continuous with the right atrium, the JVP is a reliable estimate of right atrial blood pressure (Central Venous Pressure). The JVP on the right side is a better")
AAA-Clinical-Findings-and-Complications
: Clinical Findings and Complications AAA = Abnormal, irreversible dilation of a focal area of abdominal aorta (area of aorta between
diaphragm & aortic bifurcation) to twice the diameter of adjacent normal artery segments
Asymptomatic, non-ruptured aneurysm:
Most AAAs are asymptomatic until rupture or days before impending rupture
Asymptomatic AAAs are only detectable on imaging or by palpation
Given their structural weakness, AAAs are at risk of rupture (risk ↑ with ↑ size of aneurysm)
Ruptured AAA: a medical emergency
Aorta lies in between the peritoneal and retroperitoneal space
Symptomatic, non-ruptured aneurysm: rarely, an unruptured AAA can cause symptoms or complications (0.1%-1% of AAAs)
Authors: Olivia Genereux, Davis Maclean, Yan Yu* Reviewers: Jason Waechter*, Amy Bromley*, Sandeep Aggarwal*, Gregory Samis* *MD at time of publication
Posterior aortic wall rupture
Retroperitoneal hemorrhage
Sudden and severe abdominal and/or back pain
Anterior aortic wall rupture
Peritoneal hemorrhage
Peritoneal space is larger and holds larger volumes of blood
Peritoneal hemorrhages are large (entire blood volume can pool in the peritoneal space in minutes)
Prior to rupture, the adventitia (thin outermost collagenous layer of the aorta) may dilate significantly
Adventitia is the only layer of the aorta that contains sensory innervation à nociceptors there can be activated by adventitia dilation
Very rarely (0.1%), areas of stagnant blood flow within the AAA allow for blood & clotting factors to accumulate
Thrombi (blood clots) develop in these aneurysms
Thrombi may dislodge and travel (embolize) to distal vasculature, cutting off blood- flow to these areas
This process (referred to as tamponade) is crucial in preventing catastrophic blood loss, allowing for a window of opportunity for treatment
Compensated Hypovolemic Shock: Low blood pressure &
poor organ perfusion, but blood loss has temporarily stopped. This state of shock is compatible with life if patient is otherwise healthy (e.g. no coronary artery disease)
↓ space for blood to accumulate in the retroperitoneal space (compared to the peritoneal space)
Rapid pressure ↑ in retroperitoneal space overcomes the pressure in aorta
Since blood will only travel from areas of ↑ pressure to areas of ↓ pressure, this pressure gradient prevents further blood loss from ruptured aorta
Massive hemorrhage due to high blood flow volume through aorta
Hypotension and rapid progression to hypovolemic shock
Abdominal and/or àorgan ischemia
back pain
The most common symptom of a symptomatic non- ruptured aneurysm, and may be the first sign of an impending aneurysm rupture
Death within minutes
(rare)
If low blood pressure is now (inappropriately) treated with fluid resuscitation, the blood pressure will ↑
Differential pressure gradient is reversed (aortic blood pressure > pressure in retroperitoneal space)
Bleeding into retroperitoneal space resumes
Decompensation of hypovolemic shock Possible death
Kidney ischemia
Lower limb ischemia
Time exists to transfer patient to tertiary care center for surgical treatment
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published February 28, 2021 on www.thecalgaryguide.com")
perikarderguss-tamponade-pathogenese-und-klinische-befunde

Death Cardiovascular Respiratory and Neurologic Mechanisms

Hypoxemia (Type I Respiratory Failure): low dissolved oxygen in blood (PaO2)
Lungs can’t oxygenate blood fast enough
Lungs can’t rid blood of CO2 fast enough
Hypercapnia / hypercarbia (Type II Respiratory Failure): elevated dissolved CO2 in blood (PaCO2)
Cerebral vasodilation
Toxins: e.g. cyanide, pesticides, arsenic Severe anemia
Distributive problems:
Systemic inflammation (sepsis, anaphylaxis, pancreatitis), adrenal insufficiency, vasodilatory drugs
Obstructive problems: Cardiac tamponade*, tension pneumothorax* or massive pulmonary embolism*
Hypovolemic* problems (low blood volume): Hemorrhage, dehydration, widespread skin disruption or burns
Cardiac valve dysfunction
Myocardial infarction* or cardiomyopathy
Cardiac arrhythmia or heart block
Disturbed electrical activity in cardiomyocytes
Peripheral metabolic disturbances
Hypokalemia*, Hyperkalemia* Acidosis* (including renal failure) Hypothermia*
Toxins* (e.g. cocaine, beta blockers, tricyclics) Severe thyroid derangement
Inappropriate systemic vasodilation
Adjacent forces impair heart filling
Low cardiac preload
Low stroke volume (SV; depends on valves, contractility, preload)
Decreased systemic vascular resistance (SVR)
Low blood pressure (BP = CO x SVR)
Decreased cardiac output (CO = SV x HR)
Disseminated intravascular coagulationàwidespread thrombi that occlude blood flow (also causes hemorrhage, see relevant box at left)
Methemoglobinemia: some hemoglobin gets stuck in a state that can’t carry O2
Hemoglobin has reduced capacity to carry or release O2
Drugs: e.g. dapsone, nitrates
Carbon monoxide poisoning
Circulatory collapse / shock: inadequate perfusion of tissue with blood
Respiratory collapse: blood has insufficient useable O2 content
Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)
Hypoxia*: inadequate O2 delivery or utilization in tissues
Hypoxia creates metabolic disturbances that impair cardiac cells. Alternatively, any of the preceding conditions marked with (*) can directly trigger cardiac arrest first
Pulseless Electrical Activity (PEA): organized activity on ECG with no cardiac output (can be preceded or mimicked by pseudo-PEA, in which there is still some output on ultrasound)
Low atmospheric pressure or oxygen content Severe lung disease
Asthma, COPD, interstitial lung disease, congestive heart failure, pulmonary hypertension, pulmonary embolism, lung collapse / atelectasis
Acute respiratory distress syndrome
Pneumonia, aspiration pneumonitis, inhalational injury, systemic inflammation, drowning
Severe hypoventilation
Respiratory fatigue, advanced COPD, chest wall disorders, neuromuscular disorders, upper airway obstruction, toxins (e.g. opioids, botulism)
Can degenerate at any time
Asystole: no cardiac electrical activity or output
Death
Respiratory arrest: cessation of breathing
Inability to protect airway
Decreased level of consciousness
Note
This is a broad overview of the many scenarios that can result in death. For detailed explanations of the various disease mechanisms, refer to the corresponding slides.
* = reversible causes of cardiac arrest (Hs and Ts)
Author:
Ben Campbell
Reviewers:
Yan Yu*
Huma Ali*
* MD at time of publication
Bradycardia
(low heart rate, HR)
Unopposed parasympathetic stimulation of heart (can also cause vasodilation, see Distributive problems)
Disruption of spinal cord sympathetic control
Injury to cervical or upper thoracic spinal cord
Irreversible cessation of cardiac, respiratory, and brain function
Prolonged seizure initially causes increased cardiovascular activity, until the system fatigues
Disruption of respiratory control center in medulla
Expanding skull contents squeeze brainstem (herniation)
Increased intracranial pressure
Edema from intracranial hemorrhage, trauma, brain mass
Edema, inflammation, hypoxia and/or metabolic derangements cause diffuse neuron dysfunction
Central nervous system infection
Dementia, particularly with delirium
Massive ischemic stroke
Seizure
activity prevents or alters breathing
Metabolic disturbances that affect the central nervous system Hypoglycemia Hypocalcemia, hypercalcemia Hyponatremia, hypernatremia Uremia
Acute liver failure (hyperNH4) Many drugs / toxins Withdrawal (e.g. EtOH)
Status epilepticus
Brainstem lesion (e.g. stroke, neoplasm, inflammatory)
Nervous System Insult
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 11, 2023 on www.thecalgaryguide.com
Respiratory System Insult
Cardiovascular System Insult Cardiogenic problems")
Pulsus Paradoxus

Thoracic cavity expands
Lungs expand and intrathoracic pressure ↓
Physiologic:
↑ Venous return to right (R) heart
↑ R heart preload (volume of blood inside the ventricle right before it contracts)
↑ Blood pools in the right side of the heart
Obstructive lung diseases (e.g., COPD**, asthma**)
Hyperinflated lungs
↑ Stretching of pulmonary vessels at rest
On inspiration, ↑↑ stretching of pulmonary vessels
↑↑ Blood pools within pulmonary vasculature
↓↓ Flow to L heart
Pathologic: Constrictive pathologies (e.g., cardiac
tamponade**, constrictive pericarditis**) Decreased pericardial compliance
Constriction of ventricles
On inspiration, ↑ venous return to R heart (normal)
R ventricle unable to fully expand due to ↓ compliance
Septum bows into L ventricle
L ventricle unable to fully expand ↓↓ Filling of L heart
↓↓ L ventricular end diastolic volume
↓↓ L heart stroke volume ↓↓ Cardiac output Pulsus Paradoxus
Exaggerated ↓in systolic BP on inspiration (>10mmHg)
Air flows into the lungs
Pulmonary vessels are physically stretched/pulled
↑ Blood pools in pulmonary vessels
↓ Return of blood to left (L) heart
↓ L heart preload
↓ L heart stroke volume
↓ Cardiac output
Obstruction of superior or inferior vena cava (e.g., clot)
↓↓ Venous return to R heart at rest
↓↓ Right heart filling
↓↓ Blood flow to pulmonary arteries
Pulmonary embolism**
Clot occludes pulmonary arteries/ arterioles
↓↓ Flow to pulmonary veins
At rest, ↓↓ flow to L heart
On inspiration, ↓↓↓ flow to L heart
↓ Systolic blood pressure (BP) of < 10mmHg on inspiration
BP = cardiac output x systemic vascular resistance
**See corresponding Calgary Guide slides
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 21, 2013; updated Dec 3, 2024 on www.thecalgaryguide.com")
心包积液及心包填塞

Obstructive Shock

↓ Right ventricle stroke volume
(blood volume ejected per beat)
↓ Blood return to left atrium
Underfilled left ventricle
Obstructive shock
↓ systemic blood flow due to a physical
obstruction of the heart’s pumping function
Insufficient
organ
perfusion
Tension pneumothorax**
↑ Pressure in the pleural cavity
Intrathoracic pressure exceeds
venous filling pressures &
compresses heart chambers
↓ Venous return to right
atrium & left atrium
Author:
Ryan Dion
Sergio F. Sharif
Dean Percy
Reviewers:
Yan Yu
Tristan Jones
Jason Waechter*
* MD at time of publication
** See corresponding
Calgary Guide slides
↓ Preload (degree of left ventricular filling)
as left ventricle receives low levels of blood
↓ Cardiac output (volume of
blood ejected from the
↓ Blood pressure (BP)
heart/min)
Baroreceptors in carotid sinus & aortic
arch detect low blood pressure
Skin
Reflexive release of catecholamines
via sympathetic nervous system
Blood supply diverted
away from peripheral
tissues to vital organs
Tachycardia
Hypotension
Cold
extremities
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Brain
↓ Cerebral blood
flow causes
cerebral hypoxia
Altered consciousness
Heart
↓ Coronary
artery
perfusion
Myocardial
ischemia**
Complications
Blood backs up into
venous system
Kidneys
↓ Blood flow
to kidneys
Prerenal acute kidney
injury **
↑ Pressure distends
veins
↑ Jugular
venous
pressure
Pressurized fluid leaks
out of veins into
tissue
Fluid enters
pulmonary
perivascular spaces
Fluid impedes normal gas
exchange in lungs
Tachypnea (↑
respiratory rate)
Dyspnea
Published July 7, 2013; updated Sept 28, 2025 on www.thecalgaryguide.com")