SEARCH RESULTS FOR: Acute-Respiratory-Distress-Syndrome
急性呼吸窘迫综合征: 发病机制及临床表现
、溺水及吸入化学物质(如胃内容物或直接吸入性肺损伤)。
作者 : David Olmstead
审稿 : Midas (Kening) Kang, Usama Malik, Kevin Solverson* 译者:Xiumei Deng(邓秀梅)
翻译审稿人: Yonglin Mai (麦泳琳),Zesheng Ye(叶泽生) • 出版时担任临床医生
间接性肺损伤
病因包括非肺源性的脓毒血症、创伤、严重烧伤、输血相关
性肺损伤以及胰腺炎。
Note: 急性呼吸窘迫综合征是一种以急性肺损伤为 主要表现的临床综合征,表现为严重低氧血症及 双侧肺泡损伤,不伴左心压力增高。
肺组织炎症
渗出期: 由于炎症性刺激,中性 粒细胞迁移聚集至肺泡
Note: 虽然ARDS的三个病理阶段相 继发生,但是肺组织的每一个区 域并非同时处于相同的病理阶段, 因此三个病理阶段常重叠存在。
增生期: 机体试图修复肺损伤, 若修复失败,则进入纤维化期
以中性粒细胞为主的炎性渗出液
破坏肺泡表面活性物质的功能
中性粒细胞浸润及促炎细
胞因子导致肺水肿、肺功
能障碍及继发肺上皮损伤
缩略词表:
PaO2: Partial pressure of oxygen in arterial blood(动脉氧分压)
SpO2: Peripheral oxygen saturation(外周 血氧饱和度).
CXR: Chest radiograph(肺部影像学).
由于缺乏肺泡表面活性物
质,导致肺泡塌陷
肺上皮损伤,气体交换障碍
肺毛细血管不能
完全吸收渗出液
机体尝试修复肺损伤,肺
透明膜形成
通气/血流 比值失调
肺水肿 气体扩散障碍
↓ PaO2, ↓SpO2
呼吸急促
心动过速
呼吸困难
CXR:双肺 浸润影
↓ PaO2, ↓SpO2 ↑ PaCO2
↑ PaO2, ↓PaCO2
呼吸恢复正常 ↓需O 量
吞噬细胞清除肺泡腔里细胞碎片
肺泡上皮细胞修复
疾病迁延导致机体功能损伤
成纤维细胞的作用导
致胶原蛋白沉积于肺
泡腔及肺毛细血管内
气体交换的有效 肺泡表面积↑
肺泡上皮的修复,有
助于渗出液的重吸收
2 CXR:肺浸润影消散
抑郁, 焦虑,创 伤后应激障碍
咳嗽/呼吸困难 神经源性肌无力 杵状指
纤维化期: 肺修复能力不足导 致长期的肺损伤(少见)
肺纤维化
肺动脉高压 疲劳
慢性呼吸功能障碍
图注:
病理生理学
机制
体征/症状/实验室检查
并发症
2018年2月6日发布于 www.thecalgaryguide.com")
Syndrome de détresse respiratoire aigu: Pathogenèse et trouvailles cliniques
سندرم-زجر-تنفسی-حاد-ards

Acute Respiratory Distress Syndrome
 is a clinical syndrome involving acute lung injury. It results in severe hypoxemia and bilateral
Authors: David Olmstead Mao Ding Reviewers: Midas (Kening) Kang Usama Malik Kevin Solverson* * MD at time of publication
↓ PaO2 (Partial pressure of oxygen in arterial blood ↓SpO2 (Peripheral oxygen saturation)
Tachypnea (↑ RR) Tachycardia (↑ HR)
Dyspnea
Bilateral Opacity on chest radiograph
↓ PaO2, ↓SpO2
↑ PaCO 2
↑ PaO2, ↓PaCO2 Eupnea (normal
breathing)
↓ O2 Requirements Depression, Anxiety, PTSD Neuromuscular Weakness
Chronic Respiratory Dysfunction
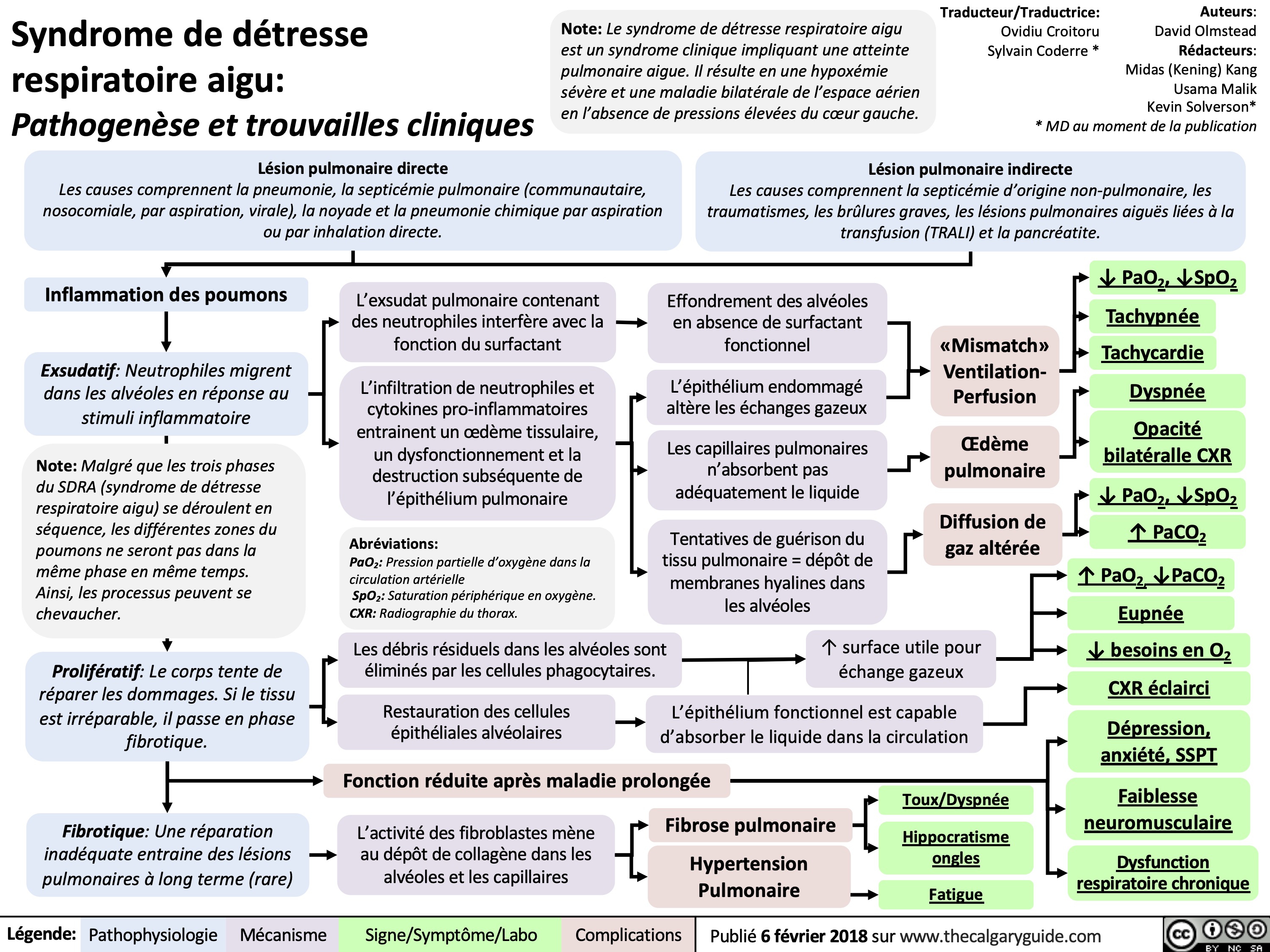
airspace disease in the absence of elevated left-heart pressures.
Direct Lung Injury
Causes include pneumonia and pulmonary sepsis (community- acquired, hospital-acquired, aspiration, viral), drowning, and chemical pneumonitis from aspiration or direct inhalational injury
Indirect Lung Injury
Causes include sepsis with a non-pulmonary source, trauma, severe burns, transfusion- related acute lung injury (TRALI) and pancreatitis
Lung Tissue Inflammation
Exudative: Neutrophils migrate into the alveoli in response to inflammatory stimulus
Note: While the three phases of ARDS take place in sequence, all areas of the lung may not be in the same phase at the same time. For this reason, the processes can be thought of as overlapping.
Proliferative: Body attempts to heal damage. If it is not successful, the tissue transitions to the fibrotic phase
Neutrophil-containing pulmonary exudate interferes with surfactant function
Neutrophil infiltration and proinflammatory cytokines lead to tissue edema, dysfunction and subsequent destruction of pulmonary epithelium
Residual debris in alveoli are cleared by phagocytic cells
Restoration of alveolar epithelial cells.
Alveoli collapse in absence of working surfactant
Damaged epithelium impairs gas exchange
Pulmonary capillaries do not adequately absorb fluid
The body’s attempts to heal lung tissue result in deposition of hyaline membranes in the alveoli
Ventilation- Perfusion Mismatch
Pulmonary Edema
Impaired Gas Diffusion
Functional epithelium is able to absorb fluid back into circulation
↑ useful surface area for gas exchange
Clearing of CXR
Impaired Function After Prolonged Illness
Pulmonary Hypertension
Fibrotic: Inadequate healing results in long-term pulmonary damage (rare)
Fibroblast activity leads to deposition of collagen in alveoli and alveolar capillaries
Fatigue Pulmonary Fibrosis
Nail Clubbing (nails appear wider & swollen) Cough/Dyspnea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 6, 2018, updated Oct 10, 2023 on www.thecalgaryguide.com
Acute Respiratory Distress Syndrome: Note: Acute respiratory distress syndrome is a clinical
Authors: David Olmstead Reviewers: Midas (Kening) Kang Usama Malik Kevin Solverson* * MD at time of publication
Pathogenesis and clinical findings
Direct Lung Injury
Causes include pneumonia and pulmonary sepsis (community-acquired, hospital-acquired, aspiration, viral), drowning, and chemical pneumonitis from aspiration or direct inhalational injury
Indirect Lung Injury
syndrome involving acute lung injury. It results in severe hypoxemia and bilateral airspace disease in the absence of elevated left-heart pressures.
Causes include sepsis with a non-pulmonary source, trauma, severe burns, transfusion-related acute lung injury (TRALI) and pancreatitis
Lung Tissue Inflammation
Exudative: Neutrophils migrate into the alveoli in response to inflammatory stimulus
Note: While the three phases of ARDS take place in sequence, all areas of the lung may not be in the same phase at the same time. For this reason, the processes can be thought of as overlapping.
Proliferative: Body attempts to heal damage. If it is not successful, the tissue transitions to the fibrotic phase
Neutrophil-containing pulmonary exudate interferes with surfactant function
Neutrophil infiltration and proinflammatory cytokines lead to tissue edema, dysfunction and subsequent destruction of pulmonary epithelium
Abbreviations:
PaO2: Partial pressure of oxygen in arterial blood
SpO2: Peripheral oxygen saturation.
CXR: Chest radiograph.
Residual debris in alveoli are cleared by phagocytic cells
Restoration of alveolar epithelial cells.
Alveoli collapse in absence of working surfactant
Damaged epithelium impairs gas exchange
Pulmonary capillaries do not adequately absorb fluid
The body’s attempts to heal lung tissue result in
deposition of hyaline membranes in the alveoli
Ventilation- Perfusion Mismatch
Pulmonary Edema
Impaired Gas Diffusion
↓ PaO2, ↓SpO2 Tachypnea
Tachycardia
Dyspnea
Bilateral Opacity on CXR
↓ PaO , ↓SpO 2 2
↑ PaCO2
↑ PaO2, ↓PaCO2 Eupnea
↓ O2 Requirements
Clearing of CXR
Depression, Anxiety, PTSD
Neuromuscular Weakness
Chronic Respiratory Dysfunction
↑ useful surface area for gas exchange
Functional epithelium is able to absorb fluid back into circulation
Impaired Function After Prolonged Illness
Fibrotic: Inadequate healing results in long-term pulmonary damage (rare)
Fibroblast activity leads to deposition of collagen in alveoli and alveolar capillaries
Pulmonary Fibrosis
Pulmonary Hypertension
Cough/Dyspnea Nail Clubbing Fatigue
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 06, 2018 on www.thecalgaryguide.com")
Acute Respiratory Distress Syndrome ARDS CXR findings
: Chest X-Ray Findings
Author: Iffat Naeem
Direct or indirect lung injury causing acute respiratory distress syndrome
(see Acute Respiratory Distress Syndrome slide for pathogenesis and clinical findings)
Activation of dysregulated inflammatory cascade
Absent pleural effusion
Normal heart size
Absent Kerly B lines
No perihilar infiltrate pattern
Bilateral infiltrate that can present in all regions of lung
Air bronchograms
Silhouette sign
Reviewers: Victória Silva, Mao Ding Tara Lohmann* *MD at the time of publication
Edema not due to a cardiogenic cause
Damage to alveolar epithelium
Necrosis of epithelial cells
Erosion of alveolar basement membrane
↑ Alveolar epithelium permeability
Damage to lung capillary endothelium
Release of inflammatory cytokines
Neutrophils migrate into alveoli
Fluid-filled alveoli show as white/grey opacities
Air-filled bronchi appear dark when surrounded by grey/white opacification of fluid-filled alveoli
Increased opacification from fluid-filled alveoli results in lack of differentiation of heart borders
Diffuse and
widespread damage to alveoli and interstitium that show as white/grey opacities
↑ Capillary endothelium permeability
Alveolar edema
Degradation of alveolar- capillary barrier
Proliferative phase
Alveolar epithelium attempts to recover
Chronic phase
Can either resolve or progress to fibrotic thickening and scaring of alveoli
↑ Leakage of fluid from capillaries into alveoli and lung interstitium
Pulmonary fibrosis (scarring)
‘White lung’ appearance
Image credit: Radiopaedia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com
Acute Respiratory Distress Syndrome (ARDS): Chest X-Ray Findings Direct or indirect lung injury causing acute
Author: Iffat Naeem Reviewers: Victória Silva
respiratory distress syndrome*
Activation of dysregulated inflammatory cascade
Bilateral infiltrate that show as white/grey can present in
Damage to alveolar epithelium
Necrosis of epithelial cells
Erosion of alveolar basement membrane
↑ Alveolar epithelium permeability
Damage to lung capillary endothelium
Fluid-filled alveoli opacities
Air-filled bronchi appear dark when surrounded by grey/white opacification of fluid-filled alveoli
Increased opacification from fluid-filled alveoli results in lack of differentiation of heart borders
Diffuse and
all regions of lung
Release of inflammatory cytokines
Neutrophils migrate into alveoli
Alveolar edema
Air bronchograms
↑ Capillary endothelium permeability
Degradation of alveolar-capillary barrier
Proliferative phase
Alveolar epithelium attempts to recover
Chronic phase
Can either resolve or progress to fibrotic thickening and scaring of alveoli
↑ Leakage of fluid from capillaries into alveoli and lung interstitium
Silhouette Sign
widespread Pulmonary damage to alveoli
‘White lung’ appearance
fibrosis (scarring)
and interstitium that show as white/grey opacities
*See corresponding Calgary Guide slides for more details
Image credit: Radiopaedia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published X, 2023 on www.thecalgaryguide.com
Acute Respiratory Distress Syndrome (ARDS): Chest X-Ray Findings Direct or indirect lung injury causing acute respiratory
Author: Iffat Naeem Reviewers: Victória Silva
distress syndrome*
Activation of dysregulated inflammatory cascade
Bilateral infiltrate that show as white/grey can present in
Damage to alveolar epithelium
Necrosis of epithelial cells
Denudation of alveolar basement membrane
↑ epithelium permeability
Degradation of alveolar-capillary barrier
Alveolar epithelium
attempts to recover through (proliferative phase)
Damage to lung capillary endothelium
Fluid-filled alveoli opacities
Air-filled bronchi appear dark when surrounded by grey/white opacification of fluid-filled alveoli
Increased opacification from fluid-filled alveoli results in lack of differentiation of heart borders
Diffuse and
all regions of lung
Air bronchograms
Release of proinflamm atory cytokines
Neutrophil migration into airspace
Alveolar Edema
↑ capillary endothelium permeability
↑ leakage of fluid from vasculature into airspace and lung interstitium
Can either resolve or progress to fibrotic
Silhouette Sign
widespread Pulmonary damage to alveoli
‘White lung’ appearance
thickening and scaring of Fibrosis alveoli (chronic phase)
and interstitium that show as white/grey opacities
Image credit: Radiopaedia
*See corresponding Calgary Guide slides for more details
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published X, 2023 on www.thecalgaryguide.com
Acute Respiratory Distress Syndrome (ARDS): Chest X-Ray Findings
Absent pleural effusion
Normal heart size
Absent Kerly B lines
No perihilar infiltrate pattern
Author: Iffat Naeem Reviewers: Victória Silva
Acute Lung Injury (see ‘ARDS: Pathogenesis and Clinical findings’ slide) causing impaired oxygenation
Lung injury not due to cardiogenic cause
(see ‘ARDS: Pathogenesis and Clinical findings’ slide)
Alveolar endothelium damage promotes inflammatory marker release
Exudative phase (1-6 days): neutrophils adhere to damaged endothelium and release pro- inflammatory mediators
Accumulation of intra-alveolar fluid that is rich in neutrophils, macrophages, and red blood cells
Proliferative phase (7-14 days): proliferation of alveolar epithelial
Fibroblasts deposit collagen tissue in alveolar walls and spaces
Can either resolve or progress to fibrotic thickening and scaring
Alveolar Edema
Fluid-filled alveoli show as white/grey opacities
Air-filled bronchi appear dark when surrounded by grey/white opacification of fluid-filled alveoli
Increased opacification from fluid-filled alveoli
Bilateral infiltrate present in all regions
Air bronchograms
results in lack of Silhouette Sign differentiation of
heart borders
Diffuse alveolar damage
‘White lung’ appearance
Image credit: Radiopaedia
*See corresponding Calgary Guide slides for more details
Legend:
(chronic phase) Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published X, 2023 on www.thecalgaryguide.com
Lung injury not due to a cardiogenic cause
Absent pleural effusion
Normal heart size
Absent Kerly B lines
No perihilar infiltrate pattern
Acute Respiratory Distress Syndrome (ARDS): Chest X-Ray Findings")