Content
Collaboration
About Us
Contact Us
SEARCH RESULTS FOR:
subdural hematom
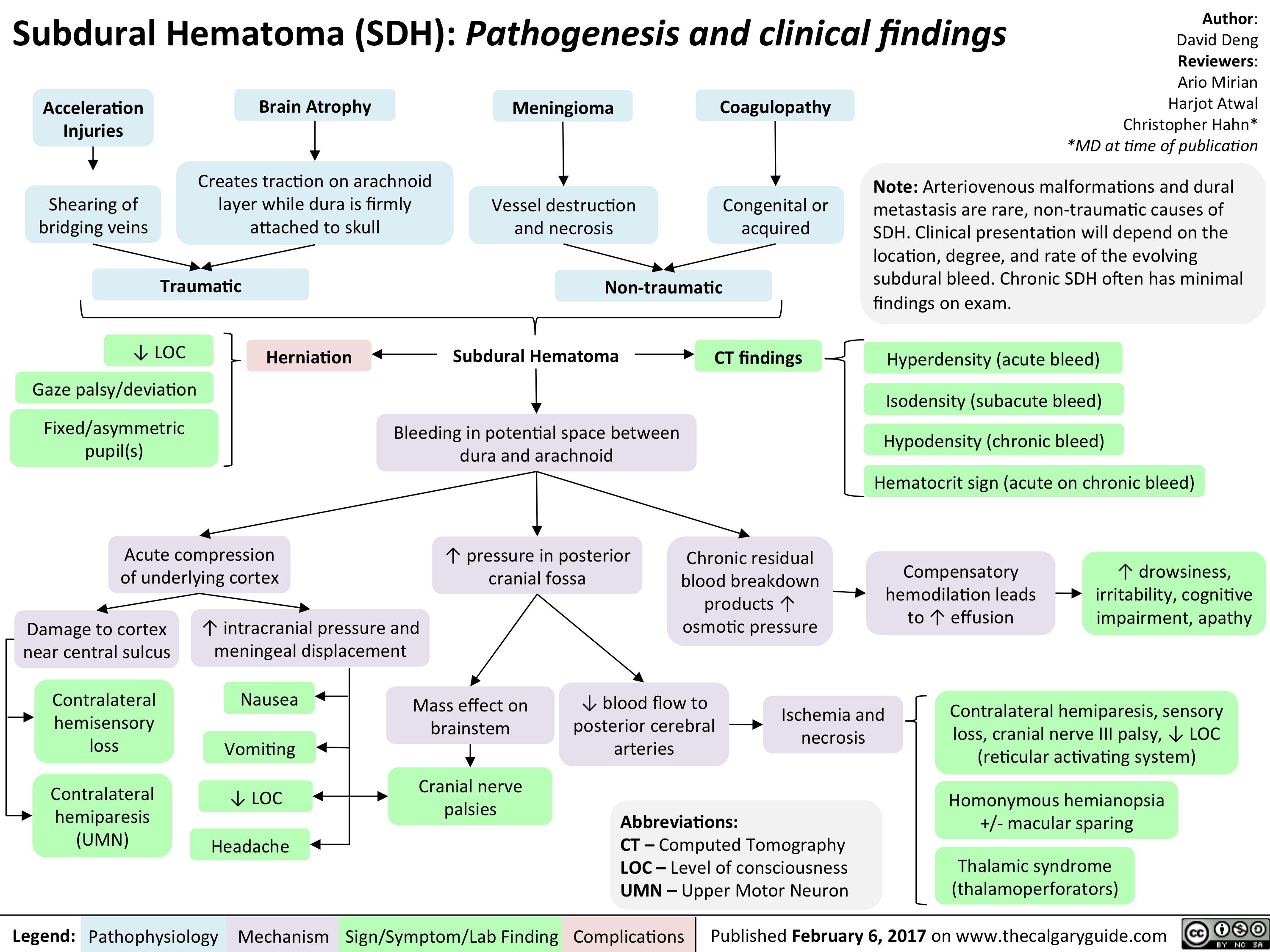
Subdural hematoma overview
Subdural Hematoma on CT
Chronic Subdural Hematoma
Acute Subdural Hematoma

Other (i.e. brain mass)
Stretching & tearing of bridging cortical veins that cross from the cortex to dural sinuses
Crescent shape
Blood accumulation in the potential space between the dura mater & the arachnoid mater
As the blood clots over time, its appearance varies on CT and is measured as different radiodensities (MRI may be needed to detect subtle bleeds)
Acute < 3 days
Subacute 3 days to 3 weeks
Chronic > 3 weeks Acute on Chronic
Acute blood (50-60 HU) is hyperdense to the surrounding cortex
As blood clot ages and protein degradation occurs, the density drops to 35-40 HU
The collection of blood becomes hypodense (~0 HU) to adjacent cortex
Both hypodense & hyperdense collections visible forming a hematocrit level
Hounsfield units (HU) are a measure of radiodensity (Air -1000 HU appears black, CSF is 0 HU appears dark, and cortical bone is >1000 HU appears white)
Hypodense collection
A pre-existing chronic hematoma
Hematocrit level
Fluid-fluid level in the case of an acute bleed into a pre-existing chronic subdural collection.
This can also be seen in patients with coagulopathy as blood clots improperly, allowing for dependent blood layering
Hyperdense collection
Acute blood sinks inferiorly (as CT is taken with patient supine)
Authors: Nameerah Wajahat, Aly Valji, Omer Mansoor Reviewers: Reshma Sirajee, Tara Shannon, Mao Ding, Petra Cimflova* *MD at time of publication
Subdural hemorrhages spread past suture lines to take on a crescent shape (seen bilaterally on this CT), but limited by dural reflections (falx cerebri, tentorium)
R
Intracranial pressure ↑
Mass effect on the brain tissue
Midline shift
Shift of brain tissue across the center line of the brain (dashed line shows ideal midline)
Ventricular effacement (partial)
Ventricles appear smaller as some cerebrospinal fluid (CSF) is pushed out
Sulcal effacement
CSF filled sulci become less apparent as CSF is squeezed out and gyri are lying on each other
Herniation
Protrusion of brain through rigid membranes or foramina of skull
Axial CT Head: Acute on Chronic Bilateral Subdural Hematoma showing features of both acute and chronic bleeding. Image Source: Radiopaedia.org
Legend:
Pathophysiology
Mechanism
Radiographic Findings
Complications
Published May 10, 2023 on www.thecalgaryguide.com")
: Pathogenesis and Clinical Features Atraumatic SDH risk factors
Authors: Cora Laidlaw Reviewers: Braxton Phillips Shahab Marzoughi Gary Michael Klein* * MD at time of publication
For more information on acute subdural hematoma, see Calgary Guide slide - Acute Subdural Hematoma (SDH):
Traumatic SDH mechanisms
Intoxication leading to decreased balance and coordination
Neurodegenerative disease causes cerebral atrophy (such as ALS, MS, and dementia)
General cerebral atrophy with increased age
Chronic alcohol use dilates blood vessels, thinning the walls
Thinner, developing vessels in infants
Age related risks: decreased vision, decreased mobility, decreased balance
Low Impact trauma such as minor falls
Child abuse
Increased tension on bridging veins as ↓ brain volume ↑ distance they must span
Bridging veins are more delicate
Abusive head trauma
Cytokines increase the leaky nature of vessels
Blood degradation over time releases proinflammatory cytokines
Atraumatic risk factors combined with traumatic mechanisms results in the breaking of bridging veins
Low pressure venous blood slowly accumulates between the dura and arachnoid meningeal layers (increased with anticoagulation, hypertension, or other bleeding risk factors)
Damaged tissue release inflammatory factors that promote angiogenesis through secondary intention (the use of granular tissue to fill in the non-approximated edges of the blood vessels)
As the vessels are not approximated (connected to be rejoined), the granular tissue does not create a solid blood vessel wall
Vessels are partially repaired and leaky in nature
Recurrent bleeding due to small traumas and fluid accumulation due to leaky vessels results in expansion
Chronic Subdural Hematoma
(Bleeding within potential space between dura and arachnoid meningeal layers present >14 days)
Dural attachments limits fluid expansion
Local increased pressure and a mass effect on underlying brain tissue
Cerebral atrophy (specific areas and therefore symptoms will depend on lesion location)
Mesial temporal lobe
Impaired memory (including verbal)
Acute blood is present in small volumes with larger volume chronic hematoma
Damaged tissues release proinflammatory cytokines from immune cells (astrocytes, peripheral immune cells, neurons, and microglial cells)
Acute blood appears hyperintense on T2 MRI
Chronic blood appears hypointense on T2 MRI
Cytokines inflame nociceptive neurons (such as the trigeminal neuron)
Recurrent headaches
Altered mental status (confusion) Personality changes
Damage to neuronal tissue
Mass compression of underlying vasculature Hypoperfusion of brain tissue
T2 MRI Brain shows lesions with hyperintensive cores surrounded by hypointensive
Pressure placed indirectly onto cerebellum with inferior displacement of brain mass
Gait ataxia
Frontal lobe atrophy (specifically in orbitofrontal area) Orbitofrontal area Prefrontal cortex
Impaired working memory (short term memory used for rapid executive, phonological visuospatial thought processes)
Atrophy of focal brain structure
Contralateral homonymous hemianopsia (loss of the half visual fields in both eyes)
Somatic motor cortex
Contralateral hemiplegia (inability to move the body opposite to the side of lesion)
Primary visual cortex Pontine micturition centre
Urinary incontinence (uncontrolled leakage of urine)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")
: Clinical Presentation Subdural Hematoma
Authors: Cora Laidlaw
Reviewers: Braxton Phillips Shahab Marzoughi Sina Marzoughi* * MD at time of publication
Ischemia of cranial nerve tissue in brainstem
Cranial nerve palsies
↓ Level of consciousness
Generalized or focal seizures
Uncal herniation
Compression of oculomotor nerve (CN III) – responsible for eye movement (adduction, elevation, and depression) and parasympathetic tone
Eyes fixed outwards and down with pupillary dilation
↑ Pressure compresses intracranial tissue
Compression of brain structures
Compression of arterial vasculature in brain
↓ Global perfusion to intracranial tissue
Uncus (mediobasal aspect of temporal lobe) herniates into the infratentorial via the tentorial notch
Cerebellar tonsils (part of posterior lobe of cerebellum) herniates through foramen magnum (opening in base of skull)
Cerebellar tonsil herniation
Tonsils compress brainstem
Brainstem loses ability to control vital functions of life (such as respiration, heart rate, blood pressure)
Coma or death
Blood accumulation results in ↑ intracranial pressure
(Bleeding within potential space between dura and arachnoid meningeal layers )
Compression of nociceptors in meninges and meningeal vasculature
Headache
Compression of medulla (contains emetic center)
Stimulation of emetic centers
Loss of function of primary sensory cortex (posterior to central sulcus)
Contralateral hemisensory loss (including proprioception, fine touch, and two point discrimination)
Loss of function of primary motor cortex (anterior to central sulcus)
Contralateral hemiparesis (upper motor neuron)
Ischemia and necrosis of brain parenchyma
Cerebral disturbances altering neuronal networks
Vomiting
Nausea
See Calgary Guide slide - Chronic Subdural Hematoma (SDH): Clinical Presentation
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")