SEARCH RESULTS FOR: stroke
Myocardial Infarction: Findings on History
 L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" title="Yu Yan - MI Findings on History - FINAL.pptx -
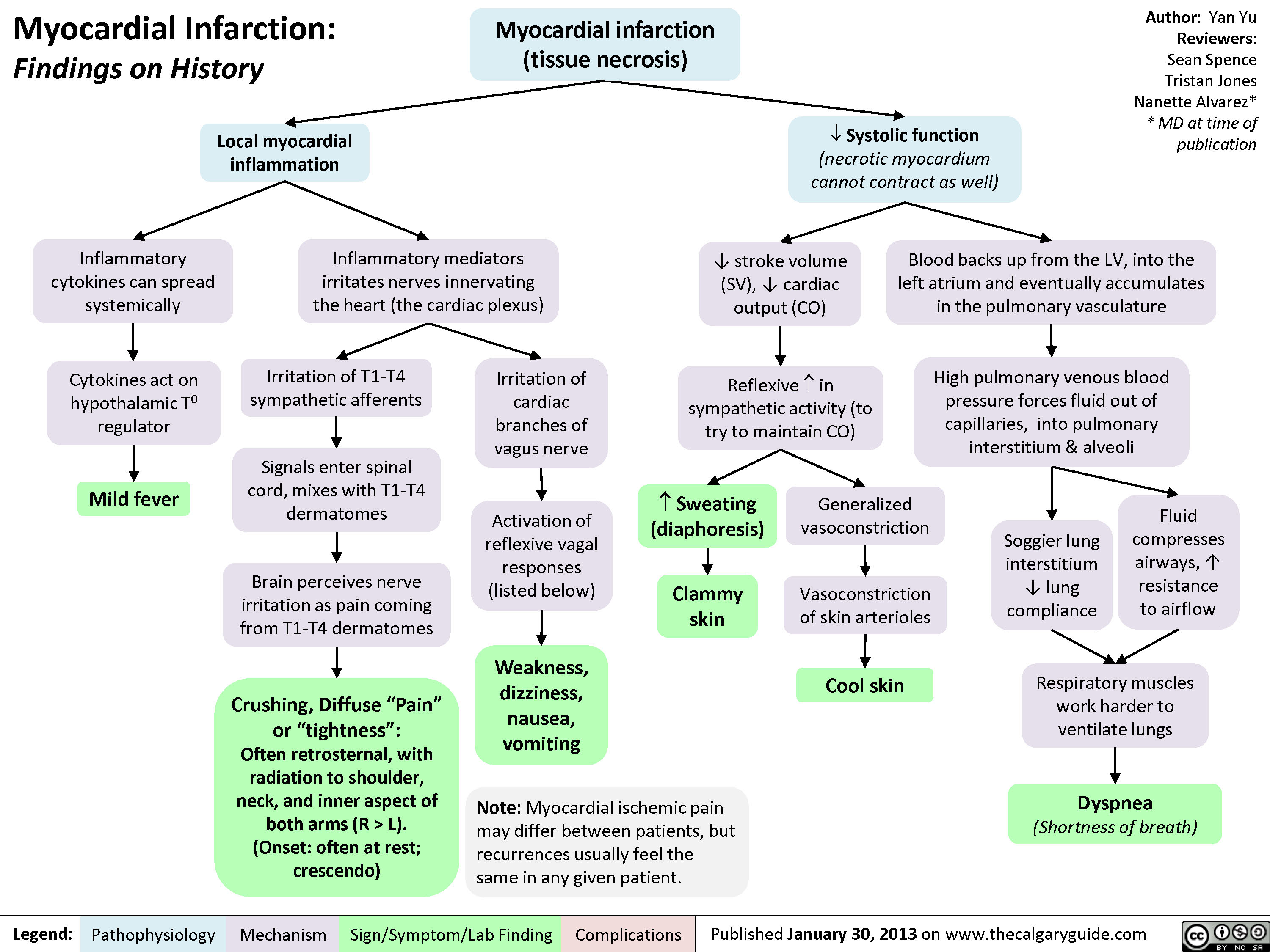
Myocardial Infarction: Findings on HistoryLegend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceTristan JonesNanette Alvarez** MD at time of publication Systolic function(necrotic myocardium cannot contract as well)Reflexive ? in sympathetic activity (to try to maintain CO)Clammy skin? stroke volume (SV), ? cardiac output (CO)Myocardial infarction (tissue necrosis)Note: Myocardial ischemic pain may differ between patients, but recurrences usually feel the same in any given patient.Generalized vasoconstrictionVasoconstriction of skin arteriolesCool skinLocal myocardial inflammationIrritation of T1-T4 sympathetic afferentsIrritation of cardiac branches of vagus nerveSignals enter spinal cord, mixes with T1-T4 dermatomesCrushing, Diffuse "Pain" or "tightness": Often retrosternal, with radiation to shoulder, neck, and inner aspect of both arms (R > L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" />
L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" title="Yu Yan - MI Findings on History - FINAL.pptx -
Myocardial Infarction: Findings on HistoryLegend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceTristan JonesNanette Alvarez** MD at time of publication Systolic function(necrotic myocardium cannot contract as well)Reflexive ? in sympathetic activity (to try to maintain CO)Clammy skin? stroke volume (SV), ? cardiac output (CO)Myocardial infarction (tissue necrosis)Note: Myocardial ischemic pain may differ between patients, but recurrences usually feel the same in any given patient.Generalized vasoconstrictionVasoconstriction of skin arteriolesCool skinLocal myocardial inflammationIrritation of T1-T4 sympathetic afferentsIrritation of cardiac branches of vagus nerveSignals enter spinal cord, mixes with T1-T4 dermatomesCrushing, Diffuse "Pain" or "tightness": Often retrosternal, with radiation to shoulder, neck, and inner aspect of both arms (R > L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" />
myocardial-infarction-findings-on-physical-exam
 Diastolic compliance (necrotic myocardium does not relax as well to accommodate blood)Necrosis of papillary muscles:S4(4th heart sound)? Force of ventricular contractionsMitral valve regurgitationBlood")
jvp-kussmals-sign-explained
: Kussmal's Sign explainedExcessive pericardial fluid compresses heart walls on all sidesLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publication? Right ventricle wall complianceConstrictive pericarditisRight ventricle prevented from fully expanding ? ability of the right ventricle to accommodate higher venous returnBackup of venous blood into right atrium and preceding internal jugular veinsRestrictive cardiomyopathyInflamed, fibrotic pericardium restricts expansion of heartRight ventricle myocardial infarct Cardiac tamponade (rare)InspirationMore venous blood tries to enter the low-pressure thoracic cavity via the right ventricle? pressure in thoracic cavity
JVP should return to normal within 3 respiration cyclesJugular Venous Pressure (JVP): Physical Exam FeaturesExerts less force against vesselsTilting the head of the bed:Low pressure, & the thinner walls of the internal jugular veins, are less able to keep lumen open when compressedLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publicationBlood in internal jugulars settles to bottom of the vein (analogy: half-full tube of water is turned vertically)Visible waves in the JVP correspond to stages of the cardiac cycleNon-palpableBiphasic waveform? JVP The Jugular Venous Pressure (JVP) Blood pressure in the internal jugular veinsV-waveA-waveRight atrial contractionBlood passively fills right atrium during ventricular systole? JVP? JVPIn: ? intrathoracic pressurePressing hard on abdomen (overlying the liver), or doing a valsalvaFacing lower afterload, Right heart more readily pumps blood into pulmonary circulation? abdominal pressure? venous blood forced up into right atriumVenous blood pressure is normally very lowOccludableNote: Since the internal jugular veins are continuous with the right atrium, the JVP is a reliable estimate of right atrial blood pressure (Central Venous Pressure). The JVP on the right side is a better")
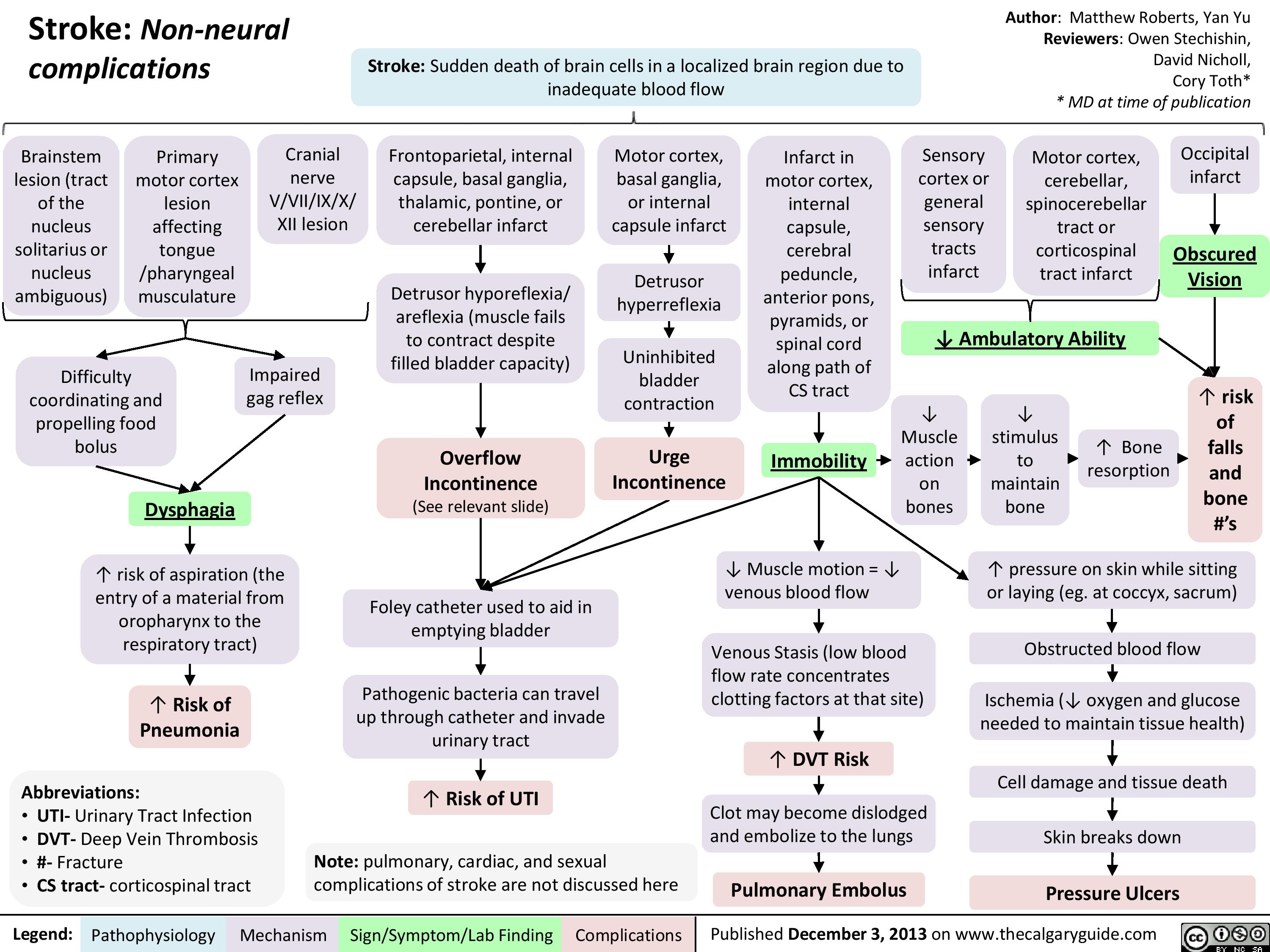
Non Neural Complications of Stroke
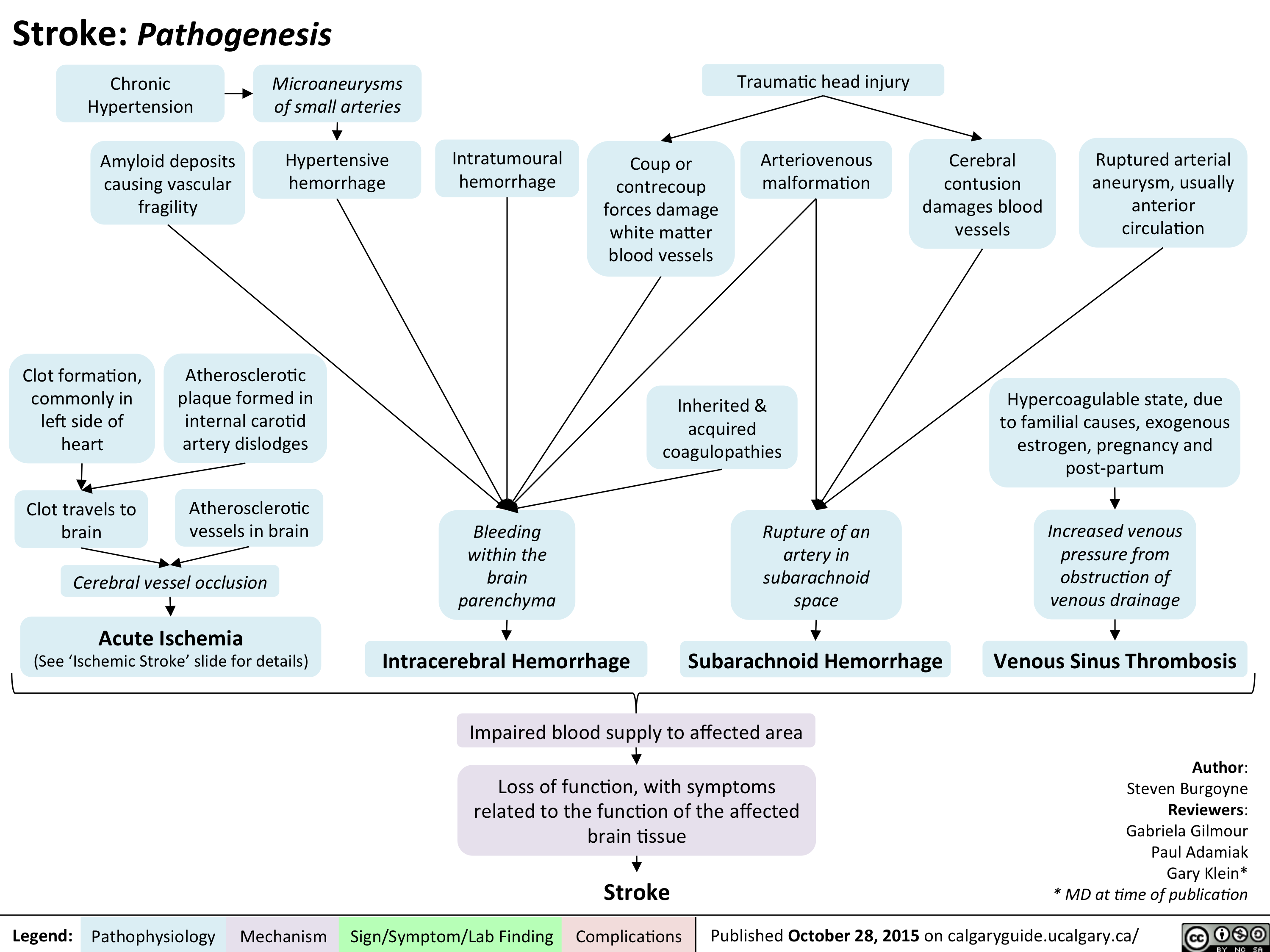
Stroke - Pathogenesis
Left Heart Failure: Pathophysiology (Neurohormonal Activation)

Frank Starling Mechanism • The Frank Starling mechanism of the heart represents the relationship between preload (EDV) and SV • As preload (EDV) increases, SV increases, because higher volumes of blood in the ventricles stretch the cardiac fibers and increases cardiac contraction during systole. However, volume overload causes reduced SV.
Myocardial Dysfunction: • Left ventricular Compensatory 4, SV 4A, CO 4 Mechanisms
4, BP
Important equations: • BP = CO x SVR • CO = SV x HR Cardiac hemodynamics: • Stroke volume is affected by three factors 1) Preload (end-diastolic volume (EDV)) 2) Afterload (resistance to LV ejection) 3) Contractility (inherent strength of contraction of LV myocytes) Definition of heart failure: • Myocardial dysfunction (systolic or diastolic) results in decreased CO, such that the heart cannot meet the body's metabolic demands or can only do so at elevated filling pressures
Anti-diuretic hormone (ADH) activation: Arginine 4, BP 4 carotid sinus Vasopressin --• and aortic arch (V2) receptor baroceptors activation activation 4 I` ADH release
RAAS System: 4, BP 4 t release of renin from the juxtaglomerular kidney cells due to renal hypoperfusion
SNS System: In response to CO, 4 SNS t release of (catecholamines) norepinephrine and epinephrine
Adrenal Glands: Aldosterone release
Angiotensin II Type 1 receptor activation
al receptor activation
13, receptor activation
—•
Renal Collecting Ducts: t H2O retention
Renal Distal —• Tubules: t Na+ & H2O retention
Heart: Activation of fibroblasts 4 collagen synthesis and hypertrophy
Blood Vessels: Peripheral vasoconstriction 4 SVR
Heart: Chronic p, receptor activation 4 Ca2+ overload myocyte apoptosis
Heart: Increase HR to maintain normal CO
Maladaptive Response: t preload (EDV), —• volume overload
Abbreviations: • SV — Stroke volume • CO — Cardiac output • SVR — Systemic vascular resistance • BP — Blood pressure • RAAS — Renin-Angiotensin-Aldosterone System • SNS — Sympathetic nervous system
tin systemic and pulmonary congestion via the Frank-Starling Mechanism
Maladaptive 1` resistance Response: t BP, —• against LV afterload ejection 4 4, SV
Maladaptive Response: Adverse LV remodelling
Maladaptive Response: t myocardial oxygen demand and 4, diastolic time
4, contractility —• of the heart
4, coronary blood flow 4 myocardial ischemia
Physical signs and symptoms of congestive heart failure (see relevant slide)
Authors: Sunny Fong Reviewers: —• I Jack Fu Usama Malik Dr. Jason Waechter* *MD at time of publication")
Benzodiazepine (BZD) withdrawal: clinical findings and complications
 withdrawal: clinical findings and complications
Abrupt cessation of chronic ingestion of BZDs
Administration of BZD antagonist (flumazenil) on patients who have developed -* tolerance/dependence to BZD
Withdrawal Seizure
Negative physiological reactions BZD intake inhibition a mygd to f, • of a la Withdrawal symptoms Benzodiazepine Withdrawal GABA receptor activity (less inhibition alleviated by ingesting BZD Tolerance GABA BZD intake Conformational changes in the GABA receptor 1, receptor's Withdrawal Insomnia Pro-excitatory 4— state of excitatory neurotransmitters) 4— to the agent activity affinity for the agent
A
Activation of ACC and OFC
Feelings of fear
Activation of PAG
Behavioural response of fight or flight
Legend: Pathophysiology Mechanism
Activation of hypothalamus '1` Cortisol CAD, T2DM, Stroke
Sign/Symptom/Lab Finding
Activation of PBN
V
t RR, SOB, Asthma, or a sense of being smothered
Activation of LC
t Sympathetic Activity
t BP, t HR variability, tremor, and diaphoresis
Authors: Usama Malik Reviewers: Sina Marzoughi Aaron Mackie* * MD at time of publication
Notes: • The onset of withdrawal can vary according to the half-life of the BZD involved. Symptoms may be delayed up to three weeks in BZDs with long half-lives, but may appear as early as 24 to 48 hours after cessation of BZDs with short half-lives.
Abbreviations: • ACC: Anterior Cingulate Cortex • BP: Blood Pressure • CAD: Coronary Artery Disease • HR: Heart Rate • LC: Locus Coeruleus • MI: Myocardial Infarction • OFC: Orbitofrontal Cortex • PAG: Periaqueductal Gray • PBN: Parabrachial Nucleus • RR: Respiratory Rate • SOB: Shortness of Breath • T2DM: Type 2 Diabetes
I` atherosclerosis, cardiac ischemia, MI, or sudden death")
Arterial Insufficiency- Signs and symptoms

Reactive Neutrophilia- Pathogenesis and Clinical Findings

adrenergic-agonists-for-treating-hypotensionlow-blood-pressure
 β1-receptor
activation on
cardiac
myocytes
↑ contractility
α1-receptor
activation on
the smooth
muscle of blood
vessel walls
↑ intra-cellular Ca2+
in these cells, ↑
their contraction
Ephedrine
Direct
effect
Indirect
effect
↑ release of endogenous norepinephrine
from the adrenal medulla (see above)
Mimics epinephrine
(see above)
Primary
Indications:
anaphylaxis,
cardiac arrest
Primary
Indications:
Hypovolemic states
(e.g. blood loss),
Low systemic
vascular resistance
states (e.g. sepsis,
Anesthesia-induced
hypotension)
Primary
Indications:
mainly used in
Anesthesiainduced
hypotension
↑ intracellular
Ca2+ ↑ rate of
myocyte
contraction
Phenylephrine
↑ Cardiac
Output
↑ heart rate
↑ strength
of myocyte
contraction
↑ arterial
wall tone
↑
stroke
volume
Pushes more
blood to flow
back to heart
(↑ preload)
↑ systemic vascular
resistance (SVR)
More blood in
ventricles stretch
myocytes more
optimally for ↑
contractility
(Frank Starling
Law)
↑ venous
wall tone
↑ Blood
Pressure
Nonspecific activation of α and β receptors on other areas of the body
(e.g. on the autonomic nervous system) as well as on cardiac myocytes
Hypertension
Cardiac Dysrythmias: e.g.
palpitations, ventricular fibrillation
Tremors Cardiac
arrest
All four
drugs")
virchows-triad-and-deep-vein-thrombosis-dvt
:
Authors: Dean Percy Yan Yu Reviewers: Tristan Jones Ryan Brenneis Man-Chiu Poon* Maitreyi Raman* * MD at time of publication
Pregnancy, Oral Contraceptives (OCP)
Pathogenesis and Complications
Platelet Activation
Increased clot formation
Hypercoagulable State
↑ ability for the blood to coagulate upon stimulation
Inherited Disorders
Congenital defect in coagulation (ie. Factor V Leiden, Factor II
mutation, Protein S/C deficiency) ↑ blood clotting ability
Estrogen promotes
hypercoagulability, especially in presence of other risk factors
Notes:
• Venous thrombus causes pulmonary embolism, arterial thrombus causes stroke
• Previous DVT is risk factor for current DVT
Trauma/Surgery
Malignancy
Abnormal release of coagulation-promoting cytokines
Systemic injuryà activation of coagulation cascade
Hypertension
Bacteria Artificial Valve
Physically damages blood vessel walls
Adhere/invade vessel wall
Abnormal surface
Vessel Injury
Exposes tissue factor on damaged cells and subendothelium for vWF binding
Virchow’s Triad
Venous Stasis
Low blood flow rate over site of vessel injury, concentrating blood clotting factors at that site
Fat contains more aromatase, converts more androgens to estrogen
Sedentary lifestyle, poor venous return
Obesity
Clot formation typically occurs in leg veins
Deep, large veins allow for blood pooling (stasis, hypercoagulability) Venous return from legs often against gravity (stasis)
Valves in leg veins prone to backflow (stasis)
↓ muscle motion = ↓ venous blood flow
Fracture, immobilization, bedrest, long vehicle/airplane ride
Destruction of vein valve by clot
Venous Insufficiency
Clot prevents blood from returning to heart. Blood accumulating in the leg results in unilateral leg edema and venous inflammation (redness, warmth, tenderness)
1. 2. 3.
Clot embolizes to the lungs
Thromboembolus
-*Pulmonary embolism (acute life threatening complication)
-Chronic thromboembolic pulmonary hypertension
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published September 1, 2019 on thecalgaryguide.com")
Aphasia
: Pathogenesis and clinical findings
Authors: Davis Maclean Reviewers: Heather Yong Tony Gu Yan Yu* Scott Jarvis* *MD at time of publication
Ischemic stroke (common)
Local Invasion (e.g. by a tumour, Head infection, or hemorrhage) Trauma
Intracerebral Hemorrhage
Dementia (e.g. Fronto- temporal Dementia)
Episodic occurrences (e.g., migraine, epilepsy)
Damage to language-dominant cerebral hemisphere (the left hemisphere, for the majority of humans):
Damage affecting Broca’s Area in the Inferior frontal gyrus (area 44 & 45)
Damage affecting Wernicke’s Area in the posterior part of the superior temporal gyrus (area 22)
Localization: Inferior frontal gyrus, superior sylvian fissure
Blood supply: superior division M2 branch middle cerebral artery
Localization: Posterior perisylvian region, temporal lobe
Blood supply: inferior division M2 middle cerebral artery
Sensory speech
areas still intact (posterior superior temporal lobe)
Intact comprehension (intact hearing & reading)
Impaired function of Broca’s Area
↓ output or generation of speech/ text
If function of nearby motor areas is also impaired
Contralateral hemiparesis (face, arm > leg)
If function of other nearby areas is also impaired
Impaired naming and repetition
Motor speech areas still intact (inferior frontal lobe)
Fluent (but non-sensical) speech output
Impaired function of Wernicke’s Area
Impaired compre- hension (i.e. cannot understand speech or text)
Loss of sensory speech input to motor areas
Errors in word usage, tense, structure
If function of nearby sensory areas is impaired
Contralateral sensory deficits
Broca’s Aphasia
Wernicke's Aphasia
(Expressive language impairment: non-Fluent)
Notes/Definitions:
(Receptive language impairment/Fluent: the person can talk but their speech is nonsensical)
• Dysarthria ≠ Aphasia (Dysarthria: disruption to neurons controlling the muscles that produce sounds, resulting in slurred/disjointed speech. Aphasia: acquired deficit in language comprehension or generation/output usually due to disruption of neurons in the cerebral cortex.)
• “Global” aphasia affects both receptive and expressive language.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 1, 2020 on www.thecalgaryguide.com")
vomiting-pathogenesis
 Center
Toxins circulating in bloodstream: Chemotherapy, Opioids
Offending substance travels through circulation and binds to receptors in the CTZ, outside the blood brain barrier
Abbreviations:
GERD: Gastroesophageal Reflux Disease PUD: Peptic Ulcer Disease
IBD: Inflammatory Bowel Disease
CTZ: Chemoreceptor Trigger Zone
CNX: Cranial Nerve Ten
H1: Histamine Receptor
M1: Muscarinic Receptor
Disrupted inner ear balance: Motion Sickness
Activation of H1 & M1 receptors in vestibular center traveling via Cerebellum
Stimulates Solitary Tract Nucleus (Medulla)
(Medulla)
Vagus Nerve (CNX) and enteric nervous system activation, resulting in:
Gastric relaxation, ↓ pylorus tone, retrograde duodenal peristalsis
Downward diaphragm contraction, abdominal & chest wall muscles contract: ↑ intra-gastric pressure
Vomiting
(Forceful expulsion of material from stomach and intestines)
Upper and lower esophageal sphincter relaxation and glottis closure
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-published February 16, 2020 on www.thecalgaryguide.com")
Marfan-Syndrome

Dural ectasia
(widening of the dural sac)
Diminished and disorganized dural elastic fibres
Abnormalities in connective tissues
Tear in the aortic intima (innermost layer of aorta)
Aortic dissection
Type A (tear in ascending aorta) > Type B (tear in descending aorta)
Back pain
Sensory and motor deficits
Ectopia lentis
(lens dislocation)
Development of lung bullae and blebs
Rupture of bullae/blebs
Pneumothorax
** Abnormal properties of lens + cornea
** Scoliosis
** Myopia
Tall stature Chest wall (pectus)
Inherited (autosomal dominant) or de novo mutation in FBN1 gene
Distortion of neural roots
Thinning of ciliary zonules of the eye
Weakness and rupture of alveolar tissue
Production of aberrant or reduced fibrillin-1
Formation of unstable microfibrils in extracellular matrix of connective tissues
**
inactivate TGF-β1
↑ production of matrix metalloproteinases
↑ cellular signaling cascades
↑ production of growth factors in the endocardium
Cell proliferation and apoptosis suppression in mitral valve leaflets
Change in valvular architecture
Mitral prolapse
Mitral regurgitation
↑ degradation of extracellular matrix
Thinning of the aortic media
Weakness of the aortic wall
Inability of fibrillin- 1 to sequester and
↑ TGF-β1 signalling
Abbreviations
• TGF-β: Transforming
growth factor beta (a cytokine)
Notes
**The underlying
mechanisms are unclear
Authors:
Tony Gu Reviewers: Amanda Nguyen Davis Maclean Yan Yu* Michelle Keir*
* MD at time of publication
Aortic root dilation
Aortic valve leaflets stretched outwards, unable to fully close
Aortic regurgitation
Aneurysmal dilation of the abdominal & thoracic aorta
Aortic rupture
Stroke
Blood enters and pressurizes a ‘false lumen’
Obstruction of aortic branches
End organ malperfusion
** deformities
** Joint hypermobility
Thumb sign: Thumb tip extends from palm of hand when thumb is folded into closed wrist
Wrist sign: thumb and fifth finger of the hand overlap when grasping opposite wrist
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 28, 2020 on www.thecalgaryguide.com")
Hereditary Hemorrhagic Telangiectasia (Osler-Weber-Rendu disease)
:
Pathogenesis and Clinical Findings
Inherited or de novo mutation in the ACVRL1, ENG, or Smad4 genes
Abnormal signalling within the transforming growth factor ß (TGF-ß) pathway
Unclear mechanismsàInability of vascular mural cells to stabilize and remodel newly formed blood vessels
Excessive proliferation of endothelial cells and ensuing overgrowth of blood vessels
Authors: Tony Gu Reviewers: Brian Rankin Yan Yu* Laurie Parsons* * MD at time of publication
Formation of friable telangiectasias
(small dilated vessels apparent near the surface of skin or mucous membranes)
Formation of Arteriovenous malformations (AVMs):
Direct connection between arteries and veins without intervening capillary bed
Nasal telangiectasias
Epistaxis (nosebleeds)
Gastrointestinal telangiectasias
Gastrointestinal bleeding
Mucocutaneous telangiectasias
Cerebral AVMs
Hepatic AVMs
Left to right shunting of blood
Heart works harder to perfuse tissues
Heart failure
Pulmonary AVMs
Rupture
High flow left to right shunting of blood (the steal effect)
Cerebral ischemia
No oxygenation at capillaries
Hypoxemia
↑ erythropoietin production
Secondary polycythemia
No filtering from capillaries
Hemorrhage, shock, death
Venous emboli enter arteries (paradoxical embolism)
Stroke
Venous bacteria enter arteries
Cerebral abscess
Iron deficiency anemia
↓ serum iron is associated with ↑ coagulation factor VIII levels (mechanism unclear)
Venous thromboembolism
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 28, 2020 on www.thecalgaryguide.com")
Anesthetic-Considerations-Aortic-Stenosis
 for Patients with Aortic Stenosis Undergoing Non-Cardiac Surgery
CRRAP Goals:
Contractility, Rate, Rhythm, Afterload, Preload
Pathophysiology Driving Anesthetic Management Hemodynamic Anesthetic Intervention (CRRAP) Goals
Author:
Ryan Brenneis Reviewers: Stephen Chrusch Hannah Yaphe Yan Yu*
Karl Darcus*
* MD at time of publication
Aortic stenosis = Narrow aortic valve opening
Notes:
-Cardiac Output = Heart Rate x Stroke Volume
-Stroke volume has 3 determinates:
1. Contractility 2. Afterload
3. Preload
If the patient’s heart cannot ↑ contractility to maintain cardiac output...
↑ resistance to forward blood flow àheart must ↑ its contractility (↑ the forcefulness of its contractions) to overcome this resistance
Applying ↑ force over time causes left ventricle to undergo concentric hypertrophy
Contractility deteriorates over time
Heart rate must compensate for maintaining cardiac output
Coronary Perfusion Pressure = Diastolic BP (DBP) – Left Ventricular End Diastolic Pressure (LVEDP)
↑ cardiac muscle massà↑ myocardial metabolism and oxygen demand
↑ left ventricular wall stiffnessà↓ LV filling while relaxed (diastolic dysfunction)
Intraoperative ↓ in contractility compromises cardiac output
Bradycardia ↓ cardiac output
Tachycardia ↓ filling time of left ventricle (↓ preload)
Coronary perfusion occurs during diastole
Coronaries require a high DBP to maintain perfusion
Tachycardia ↓ perfusion time
Hypotension ↓ coronary perfusion pressure
Possible myocardial ischemiaà ↓ blood pumped into vessels
40% of LV preload supplied from atrial kick
Loss of atrial kick with arrhythmias à↓ cardiac output
Note: Aortic stenosis severity (see slide on aortic stenosis) and the type/risk of surgery guide the hemodynamic consequences and need for intervention
Adequate intravascular volume required to passively fill stiff ventricle
Contractility
↓ use of negative inotropic Maintain drugs, e.g. calcium channel
contractility blockers (“Inotrope”: drug that alters heart’s contractility)
Rate
Keep heart rate above 60 bpm
Keep heart rate below 80 bpm
Consider transcutaneous pacing, anticholinergics, & sympathetic agonists
↑ anesthetic depth, consider beta blocker (e.g. Esmolol)
Afterload
Maintain a Mean Arterial Pressure >70mmHg
Consider sympathomimetic drugs to treat hypotension
Monitor blood pressure closely via arterial line
Consider increasing anesthetic depth for severe hypertension
Rhythm
Maintain Sinus Rhythm
Consider presurgical placement of defibrillator pads & crash cart
Amiodarone ready & available during operation, to terminate any arrhythmias
Preload
Maintain Euvolemia
Possible use of transesophageal echo to monitor preload
Ensure adequate venous access- consider central venous catheter and large bore IV’s
Legend:
Pathophysiology
Mechanism
Goal
Anesthetic Intervention
Published October 25, 2020 on www.thecalgaryguide.com")
Beta-Blockers-Mechanism-of-Action-and-Side-Effects
 to these receptors, ↓ their normal adrenergic tone
Beta-2 receptor antagonism Beta-1 receptor antagonism
Lungs Eyes Central nervous system Heart Kidneys ↓ cAMP (intracellular messenger) productionàcomplex, tissue-specific intracellular mechanisms resulting in a variety of effects in different tissues:
Throughout body tissue
Epinephrine (via cAMP) indirectly ↑ the activity of the Na+/K+ pump on cell membranes (a pump that moves 3 Na+ out of cells per 2 K+ moved into cells)
Blocking epinephrine from binding
the beta-2 receptor and producing cAMPà↓ activity of Na+/K+ pump à↓K+ moved into cells
↑ proportion of K+ now resides in extracellular fluid, detectable in serum (total body K+ remains the same)
Hyperkalemia (see Calgary Guide: Hyperkalemia – Clinical findings)
Blocking sympathetic hormonesà↓ relaxation of smooth muscle circumferentially wrapped around airways
↑ resting airway muscle toneà bronchoconstriction
↑ resistance to airflow
Wheezing, dyspnea, chest tightness
Exacerbation of underlying airway disease (e.g. asthma)
↓ ciliary epithelium’s production of aqueous humor (fluid that fills anterior chamber of the eye)
Reduced intraocular pressure
Blocking adrenergic response mediated by epinephrine and norepinephrine (e.g. the physiologic “fight- or-flight” response to stress)
↓ tremor, irritability, anxiety
↓ ability to produce adrenergic symptoms in response to hypoglycemia
Hypoglycemia unawareness
Coronary perfusion pressure = diastolic blood pressure in aorta – LV end diastolic pressure
↓ inotropy (contractility of cardiac muscle)
↓ chronotropy (heart rate and conduction velocity)
↓ renin releaseà↓ creation of angiotensin II & aldosterone
+ ↓ reabsorption of Na
and H2O in nephron
↑ urinary Na+ & H2O loss
↓ total blood volume
Decompensation of acute heart failure
Dizziness and fatigue Hypotension (Blood pressure = cardiac
output x systemic vascular resistance)
↓ O2 demand of myocardial tissue
Bradycardia
Inability to ↑ heart rate in response to stress (e.g. shock, sepsis)
↓ stroke volume
↓ cardiac output
Beta blockers ↓ diastolic blood pressure, & thus may ↓ coronary perfusion pressure
Before giving beta blockers, ensure blood pressure isn’t too low
Otherwise, may worsen acute myocardial ischemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 14, 2021, updated Feb 7, 2021 on www.thecalgaryguide.com")
acute-mca-territory-ischemic-stroke-findings-on-non-contrast-ct
 strokes are generally caused by emboli (blood clot that travelled from elsewhere in the body) and less commonly caused by thrombus (blood clot that has developed locally in the MCA)
Embolism (or thrombus) occludes flow through the MCA
Acute embolism
(or thrombus) is more dense than surrounding tissue
Acute embolism (or thrombus) material attenuates (absorbs more X-rays) more than surrounding tissue (results in area of brightness)
Hyperdense MCA sign
↓ blood supply to MCA vascular territory (e.g. basal ganglia or insula)
↓ oxygen for aerobic metabolism (produces large amounts of ATP)
↓ ATP production in area of ischemia
↓ energy for ATP-dependent Na+/K+ pumps (that move Na+ out of cells) in affected neurons (grey matter)
Neurons have a higher metabolic rate than other nervous system cells (e.g oligodendrocytes that make myelin) and thus are more vulnerable to hypoperfusion and ischemia
As grey matter contains more neurons than white matter, grey matter is more vulnerable to hypoperfusion and ischemia
Grey matter shows changes on CT earlier than does white matter
Normal grey versus white matter on CT
On CT, structures that are more dense (e.g. bone, tissues) absorb more X-raysà brighter. Less dense regions (e.g. water, fluids, fat) absorb less X-raysàdarker.
Authors:
Evan Allarie Davis Maclean Viesha Ciura* Yan Yu* Reviewers:
Katie Lin* Aravind Ganesh* Gary Klein*
*MD at time
of publication
↓ extra-cellular Na+ concentration
Na+ in extracellular space is replenished via capillaries
Water follows the Na+ out of the capillaries
↑ intra-cellular Na+ concentration
Change in osmotic gradientàwater moves from extracellular space into cells
↑ water content inside & around affected neurons (grey matter)
Affected grey matter looks darker on CT (more similar to white matter)
White matter contains more fatty myelin (lower density than grey matter)à appears darker on CT
Normal insular ribbon (difficult to see here): grey matter usually seen lateral to red line shown here
Grey matter, with more neurons, has a higher densityà appears brighter on CT
Normal basal ganglia: Lentiform nucleus (putamen + globus pallidus) outlined here
Loss of grey-white differentiation throughout MCA vascular territory Difficult to see on this window (adjustable brightness of image) but is present on this scan and easily seen at different window levels
Areas with the least collateral circulation
(e.g. basal ganglia or insula) show findings first
Insular ribbon sign
(loss of insular ribbon)
Disappearing basal ganglia sign (loss of visible basal ganglia)
Comparison to normal anatomy helps outline pathologic findings
Comparison to normal anatomy helps outline pathologic findings
Images presented here are multiple CT images from the same patient with a large MCA territory ischemic stroke (Image credit: Alberta Health Services Repository)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 7, 2021 on www.thecalgaryguide.com")
VITT
: Pathogenesis and Clinical Findings
Current leading theory: COVID-19 viral vector vaccines (Johnson and Johnson and AstraZeneca) contain an anionic molecule (currently unspecified), which binds to the cationic platelet factor 4 (PF4) molecule in the bloodstream, forming vaccine/PF4 complexes
Authors: Brooke Fallis Reviewers: Yan Yu* Katie Lin* * MD at time of publication
Spleen macrophages remove antibody/platelet complexes from circulation
Fewer unbound platelets in circulation detected on complete blood count (CBC)
Thrombocytopenia: Platelets <150x!")
disseminated-intravascular-coagulation
: Pathogenesis and clinical findings
Authors: Emily Wildman Mehul Gupta Sean Spence Yan Yu* Reviewers: Kiera Pajunen Wendy Yao Tristan Jones Man-Chiu Poon* Lynn Savoie* * MD at time of publication
Sepsis
Microorganisms express pathogen- associated molecular patterns (PAMPs)
Severe Trauma
Damaged endothelial cells release damage- associated molecular patterns (DAMPs)
Solid and Hematologic Malignancies
Cancer cells express tissue factor and release procoagulants
Immune cells recognize DAMPs and PAMPs and begin expressing tissue factor and releasing procoagulants
Systemic activation of coagulation cascade
Activation of coagulation cascade results in the factor X mediated conversion of large quantities of prothrombin (factor II) to its active form, thrombin (factor IIa)
Thrombin cleaves fibrinogen (factor I) circulating in blood to an activate form known as fibrin (factor 1a)
↓ Serum fibrinogen
Diffuse coagulation causes imbalances between coagulation and anticoagulation pathways
Consumption of coagulation factors (including platelets, fibrinogen, prothrombin, factor V, factor VIII) exceeds rate of production
Fibrin, in conjunction with platelets, form widespread thrombi within vasculature
Fibrin thrombi accumulate in the microvasculature and shear transiting red blood cells
Microangiopathic hemolytic anemia (MAHA)
↑ thrombi formation ↑ fibrinolysis, a parallel process that naturally degrades fibrin thrombi
Relative deficiency of coagulation factors leads to a bleeding diathesis (tendency to bleed) despite widespread clots
↑ Prothrombin time (PT)
↑ Partial thromboplastin time (PTT)
↑ D-dimer Fibrin thrombi
↑ Fibrin degradation products
Platelets are used up forming thrombià less free platelets in circulation
↓ Platelets on Complete Blood Count
accumulate in microvasculature of major organs
Deposition of thrombi occlude blood flow resulting in ischemia of organ parenchyma
Lack of coagulation factors can predispose spontaneous hemorrhage in various organs
Multiple organ dysfunction syndrome (MODS) - (renal failure, hepatic dysfunction, stroke, pulmonary disease)
Clinical manifestations of bleeding, including petechiae (pinpoint red spots on skin), ecchymoses (bruising), weeping wound sites, bleeding mucous membranes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published Aug 7, 2012, updated July 27, 2019 & Aug 29, 2021 on www.thecalgaryguide.com")
chronic-hypertension-complications
 ≥ 135/85 (on ambulatory or home blood pressure measurement) in patients without diabetes, or BP ≥ 130/80 in patients with diabetes
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Jessica Krahn Juliya Hemmett* * MD at time of publication
↑ Afterloadà ↑ Resistance to left ventricle ejection
To overcome resistance and preserve cardiac
output, the myocardium undergoes structural and functional changes
Left ventricular hypertrophy and fibrosis
Stiff ventricle
↓ Contractility of the left ventricle
Impaired forward flow of blood from heart
Chronic stress on the endothelium of systemic blood vessels
↑ Blood pressure in retinal circulation
Hypertensive Retinopathy (See
slide on Chronic Hypertensive Retinopathy: Pathogenesis and Clinic Findings)
Smooth muscle of kidney’s
afferent arterioles constricts to prevent transmission of ↑ blood pressure to glomerulus
Overtime, smooth muscles of afferent arterioles hypertrophy from prolonged vasoconstriction
Chronic stress and trauma on endothelial and smooth muscle cells of kidney
Injury leads to excretion of cytokines and extracellular matrix such as fibrin and collagen into subendothelial layer
Endothelial dysfunction (See slide on Atherosclerosis: Pathogenesis)
Atherosclerosis
Loss of normal arterial architecture in the brain due to stress of ↑ blood pressure
Weakening of cerebral arteries
Formation and rupture of microaneurysms
Intracerebral Hemorrhage
Accumulation of plaques in
the walls of cerebral arteries
↓ Cerebral blood flow
Ischemic Stroke
Accumulation of plaques in
the walls of coronary arteries
↓ Myocardial blood flow
Oxygen supply- demand mismatch
Coronary Artery Disease
Thickening of arteriolar wall and narrowing of afferent arterioles
↓ Glomerular blood flow
Glomerular and tubular ischemia
Glomerular sclerosis and tubular atrophy
Blood backs up into lungs
↓ perfusion of blood throughout the bodyà inability of the heart to meet metabolic demands
Congestive Heart Failure
Hypertensive Nephrosclerosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2021 on www.thecalgaryguide.com")
Syndrome of Inappropriate Anti-Diuretic Hormone SIADH Pathogenesis and Clinical Findings
: Pathogenesis and clinical
Malignancy
(e.g. Small cell lung cancer, head and neck cancer)
Tumor originates from neuroendocrine cells
Tumor acts as an ectopic site of ADH production
ADH binds receptors on basolateral side (facing peritubular capillary) of principal cells in nephron
ADH ↑ principal cells’ production of Aquaporin type II channels on their apical surface (side facing tubule lumen)
↑ Reabsorption of water from the collecting ducts back into circulation
↑ Blood Volume (↑ extracellular fluid volume)
Blood Na+ levels diluted
Hyponatremia
(blood Na+ <135 mEq/L)
Brain injury
(e.g. Stroke, encephalitis hemorrhage, trauma)
↑ hypothalamic ADH production, storage in posterior pituitary, & pituitary secretion of ADH
↑ Uncontrolled ADH secretion
SIADH
(Syndrome of Inappropriate Anti-Diuretic Hormone)
Drugs
(e.g. Cyclophosphamide, SSRIs, vincristine)
Break down into active metabolites
Metabolites mimic ADH activity
findings
Authors: Krusang Patel Yan Yu* Reviewers: Davis Maclean Brooke Fallis Juliya Hemmett* * MD at time of publication
Atria and Ventricles of the heart stretch
Heart secretes ↑ atrial natriuretic and
B-type natriuretic peptides (ANP/BNP)
Peptides promotes natriuresis (excretion of Na+ into urine)
Loss of Na+ in serumàalters charge balance across neuron
membranesàImproper action potential firing:
↓ Renin secretion
↓ Release of Angiotensin II & Aldosterone
↓Reabsorption of Na+ into circulation
in area postrema of medulla
in hypothalamus in motor neurons
Extracellular fluid volume becomes hypotonic relative to intracellular fluid volume
Water moves from circulation into cells
Extracellular fluid volume normalizes
Euvolemia
Nausea
Headaches Muscle Cramps
↓ Urine volume
Cells, particularly neurons, swell up
Cerebral edema
Neurons burst and die
Severe Neurocognitive
Effects (confusion, mood swings, hallucinations, seizure, coma)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 30, 2021 on www.thecalgaryguide.com")
Renal Artery Stenosis
 of the renal artery
Renal Artery Stenosis can be unilateral or bilateral
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Jessica Krahn Timothy Fu, Brooke Fallis, Juliya Hemmett* * MD at time of publication
↓ Pressure perfusing the kidney
↑ RAAS (renin-angiotensin- aldosterone system) activation
↓ pressure gradient in glomerulus
↓ Glomerular filtration rate (GFR)
↑ Secretion of aldosterone
Turbulent blood flow through area of stenosis
Abdominal bruit on side of affected kidney(s)
↑ Secretion of Angiotensin IIà ↑ Systemic vasoconstriction
Hypertension
↑ Expression of epithelial sodium channels in cortical collecting duct
↑ Blood volume within volume- constrained space of blood vessels
↓ Renal blood flowà ischemic renal injury
Atrophy and fibrosis of affected kidney(s)
Unilateral stenosis à Kidney size asymmetry (≥1.5cm difference)
↓ Positively charged Na+ in lumen à Electronegative lumen compared to the interstitial/tubular epithelial cells
K+ follows the electrical gradient and is secreted into the electronegative tubular lumen
↓ Serum K+ concentration
Hypokalemia
*Note: In unilateral renal artery stenosis, the contralateral (normal) kidney can compensate for the increase in renal perfusion pressure caused by hypertension by increasing sodium excretion (pressure natriuresis), preventing flash pulmonary edema.
↑ NHE3 (Sodium Hydrogen Exchanger 3) activity in proximal collecting tubule
↑ Na+ and water reabsorption from renal tubular lumen into blood vessels
Chronic left ventricle pressure overload àLeft ventricle hypertrophy (see Left Heart Failure: Pathogenesis Slide)
Systolic dysfunction → ↓ left ventricle stroke volume
Normally, ↑ in renal perfusion pressureà↑ Na+ excretion and water loss (pressure natriuresis)
In bilateral renal artery stenosis*, ↓ GFRàinability for kidney to ↑ renal Na+ & water excretion à volume overload
Acute increase in afterload or preload → sudden ↑ in left ventricular filling pressures → blood backup into lungs
Pulmonary vasculature hypertension → ↑ fluid filtration across the pulmonary endothelium into interstitium and alveolar spaces
Flash (rapid onset) pulmonary edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 30, 2021 on www.thecalgaryguide.com")
obstructive-sleep-apnea-pathogenesis-and-clinical-findings
![Obstructive Sleep Apnea: Pathogenesis and clinical findings
Vascular Factors: During recumbent sleep, more bodily fluids enter the head and neck area (compared to when the patient is standing/sitting)
↑ volume of head/neck tissue surrounding the upper airwayà possible airway obstruction
Authors: Ciara Hanly Austin Laing Alexander Arnold Reviewers: Steven Liu Amogh Agrawal Yonglin Mai (麦泳琳) Naushad Hirani* Yan Yu* *MD at time of publication
Neuromuscular Factors: Sleep onset and/or the sleeping state reduces the drive of respiratory muscles to breathe
↓ Upper airway neuromuscular activityà↓ upper airway caliber, ↑ upper airway resistance, ↑ upper airway collapsibility during sleep
Structural Factors: Obesity, tonsillar or adenoid hypertrophy, macroglossia, ↑ neck circumference, craniofacial abnormalities
Excess pressure on upper airway, or deformity to that area, ↑ risk of upper airway collapse
Polysomnography
Absence of airflow but persistent ventilatory effort
Hypopnea or Apnea
Paradoxical breathing Chest wall draws in and abdomen expands during inspiration
Ventilatory effort persists against closed airway
No air entry due to collapsed upper airway
↑ Negative intrathoracic pressure
↑ Venous return to right atrium
Stretching of right atrial myocardium à secretion of atrial natriuretic peptide (ANP)
ANP inhibits epithelial Na+ channels (ENaC) in the collecting ducts of the kidney from reabsorbing Na+ à Na+ excretion
↑ Na+ excretionà↑ water excretion
Nocturia
Complete or partial upper airway obstruction during sleep
↑ PCO2 & ̄ PO2
in the lungsà ̄ diffusion gradient of CO2 & O2 between lungs & arteries
↑ PaCO2,, ̄ PaO2
Respiratory acidosis (↑ [H+] in blood)àactivation of vascular endothelial voltage gated K+ channels
Cerebral blood vessel dilation to provide adequate O2 to brain
Morning Headaches
Activation of central (medulla oblongata) & peripheral (carotid body) chemoreceptors
↑ Respiratory drive à ↑ activation of respiratory muscles (ventilatory effort )
Transient arousal from sleep
↑ sympathetic nervous system activityà arterial vasoconstriction
↑ systemic vascular resistance
Systemic Hypertension
↑ intraluminal pressure within blood vesselsàadaptive vascular endothelial and smooth muscle changes
Artery walls thicken, harden and lose elasticityà ̄ perfusion to end organs (such as the brain)
Ischemic stroke
Hypoxia during the day and night
↑ pulmonary vascular resistance
Pulmonary Hypertension
Right heart pumps against higher pulmonary pressure àcardiomyocytes undergo concentric hypertrophy over time
Cor Pulmonale
(Right heart failure due to pulmonary hypertension, separate from left heart failure)
Respiratory muscles overcome upper airway obstructionà airway patency restored
Sleep fragmentation
̄ Daytime cognitive performance and attentiveness
↑ Risk of motor vehicle accidents
Daytime Sleepiness
Eg. Epworth Sleepiness Scale >10
Abbreviations:
PCO2: partial pressure of carbon dioxide PO2: partial pressure of oxygen PaCO2: partial pressure of carbon dioxide in arteries PaO2: partial pressure of oxygen in arteries
Ventilatory response overcompensatesà breathe out more CO2 than is required for homeostasisà ̄ PaCO2
̄ respiratory driveà ̄ ventilatory effort
Resuscitative Gasping
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 19, 2013, updated May 31, 2022 on www.thecalgaryguide.com
阻塞性睡眠呼吸暂停:发病机制及临床表现
作者:Ciara Hanly, Austin Laing, Alexander Arnold 审稿人: Steven Liu, Amogh Agrawal, Naushad Hirani*,Yan Yu* 译者: Zesheng Ye(叶泽生) 翻译审稿人: Yonglin Mai(麦泳琳) *发表时担任临床医生
神经肌肉因素: 睡眠状态下, 患者无法通过 适当增加上气道肌张力来维持气道通畅
上气道神经肌肉活动 ̄à上气道直径 ̄, 上气道 阻力↑, 睡眠时上气道塌陷
结构(解剖)因素: 肥胖、扁桃体或腺样体 肥大, 舌体肥大, 颈围增大, 颅面部畸形
上气道压力过大或上气道畸形, 上气道塌陷 的风险 ↑
血管因素: 仰卧位睡觉引起 夜间嘴侧液体移位
周围组织与压力 ↑à上气道阻塞
多导睡眠描记术
没有气流,但持
续通气
呼吸浅慢或 呼吸暂停
反常呼吸 吸气时胸壁凹陷, 腹部膨隆
持续通气以抵抗气道 闭合
上气道塌陷导致空气进
入气道受阻
腹膜腔负压↑ 静脉血回流右心室阻力↑
右心房心肌细胞拉伸 à心房利钠肽分泌 (ANP)
ANP抑制肾集合管的上 皮Na+通道(ENaC)对 Na+重吸收à Na+排出
Na+排出量↑ à 水排出量 ↑
睡眠时全部
或部分上呼
吸道阻塞
肺内PO2 ̄ 且 PCO2↑ à CO2 及 O2在肺和动脉 间的扩散梯度 ̄
↑ PaCO2, ̄ PaO2
呼吸性酸中毒 (血液中 [H+] ↑) à激活血管内皮电压
门控 K+
脑血管扩张为大 晨间头痛 脑提供足够的 O2
激活中央(延髓)和外周(颈动脉体)的化学感受器 呼吸驱动↑à呼吸肌活动 (呼吸做功 )↑
短暂的睡眠唤醒
通道 交感神经系统活动↑
全天缺氧 肺血管阻力↑
肺动脉高压
右心泵血以抵抗肺 动脉高压à 随着时 间推移,心肌向心 性肥大
肺心病(区别于左
心衰,右心衰是肺
动脉高压所致)
呼吸肌克服上气道阻力à 气道 明显恢复
睡眠过程不连续
白天的认知功能
及注意力 ̄
机动车辆事故风险↑
白天嗜睡
à 动脉收缩 全身血管阻力↑
高血压
血管内压力↑ à 血 管内皮和平滑肌发生 适应性改变
动脉壁增厚、硬化、失 去弹性à器官血液灌 注量 ̄ (如脑部)
缩写: PCO2:二氧化碳分压 PO2:氧分压 PaCO2:动脉二氧化 碳分压 PaO2:动脉血氧分压
通气过度 à呼出CO2 ↑ à PaCO2 ̄
呼吸驱动 ̄à 呼吸做功 ̄
复苏性鼾音
夜尿症
如:伊普沃斯嗜睡评分
>10
缺血性卒中
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年8月19日发表 www.thecalgaryguide.com, 2022年5月31日更新](https://calgaryguide.ucalgary.ca/wp-content/uploads/2014/09/OSA-2021-1.jpg "Obstructive Sleep Apnea: Pathogenesis and clinical findings
Vascular Factors: During recumbent sleep, more bodily fluids enter the head and neck area (compared to when the patient is standing/sitting)
↑ volume of head/neck tissue surrounding the upper airwayà possible airway obstruction
Authors: Ciara Hanly Austin Laing Alexander Arnold Reviewers: Steven Liu Amogh Agrawal Yonglin Mai (麦泳琳) Naushad Hirani* Yan Yu* *MD at time of publication
Neuromuscular Factors: Sleep onset and/or the sleeping state reduces the drive of respiratory muscles to breathe
↓ Upper airway neuromuscular activityà↓ upper airway caliber, ↑ upper airway resistance, ↑ upper airway collapsibility during sleep
Structural Factors: Obesity, tonsillar or adenoid hypertrophy, macroglossia, ↑ neck circumference, craniofacial abnormalities
Excess pressure on upper airway, or deformity to that area, ↑ risk of upper airway collapse
Polysomnography
Absence of airflow but persistent ventilatory effort
Hypopnea or Apnea
Paradoxical breathing Chest wall draws in and abdomen expands during inspiration
Ventilatory effort persists against closed airway
No air entry due to collapsed upper airway
↑ Negative intrathoracic pressure
↑ Venous return to right atrium
Stretching of right atrial myocardium à secretion of atrial natriuretic peptide (ANP)
ANP inhibits epithelial Na+ channels (ENaC) in the collecting ducts of the kidney from reabsorbing Na+ à Na+ excretion
↑ Na+ excretionà↑ water excretion
Nocturia
Complete or partial upper airway obstruction during sleep
↑ PCO2 & ̄ PO2
in the lungsà ̄ diffusion gradient of CO2 & O2 between lungs & arteries
↑ PaCO2,, ̄ PaO2
Respiratory acidosis (↑ [H+] in blood)àactivation of vascular endothelial voltage gated K+ channels
Cerebral blood vessel dilation to provide adequate O2 to brain
Morning Headaches
Activation of central (medulla oblongata) & peripheral (carotid body) chemoreceptors
↑ Respiratory drive à ↑ activation of respiratory muscles (ventilatory effort )
Transient arousal from sleep
↑ sympathetic nervous system activityà arterial vasoconstriction
↑ systemic vascular resistance
Systemic Hypertension
↑ intraluminal pressure within blood vesselsàadaptive vascular endothelial and smooth muscle changes
Artery walls thicken, harden and lose elasticityà ̄ perfusion to end organs (such as the brain)
Ischemic stroke
Hypoxia during the day and night
↑ pulmonary vascular resistance
Pulmonary Hypertension
Right heart pumps against higher pulmonary pressure àcardiomyocytes undergo concentric hypertrophy over time
Cor Pulmonale
(Right heart failure due to pulmonary hypertension, separate from left heart failure)
Respiratory muscles overcome upper airway obstructionà airway patency restored
Sleep fragmentation
̄ Daytime cognitive performance and attentiveness
↑ Risk of motor vehicle accidents
Daytime Sleepiness
Eg. Epworth Sleepiness Scale >10
Abbreviations:
PCO2: partial pressure of carbon dioxide PO2: partial pressure of oxygen PaCO2: partial pressure of carbon dioxide in arteries PaO2: partial pressure of oxygen in arteries
Ventilatory response overcompensatesà breathe out more CO2 than is required for homeostasisà ̄ PaCO2
̄ respiratory driveà ̄ ventilatory effort
Resuscitative Gasping
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 19, 2013, updated May 31, 2022 on www.thecalgaryguide.com
阻塞性睡眠呼吸暂停:发病机制及临床表现
作者:Ciara Hanly, Austin Laing, Alexander Arnold 审稿人: Steven Liu, Amogh Agrawal, Naushad Hirani*,Yan Yu* 译者: Zesheng Ye(叶泽生) 翻译审稿人: Yonglin Mai(麦泳琳) *发表时担任临床医生
神经肌肉因素: 睡眠状态下, 患者无法通过 适当增加上气道肌张力来维持气道通畅
上气道神经肌肉活动 ̄à上气道直径 ̄, 上气道 阻力↑, 睡眠时上气道塌陷
结构(解剖)因素: 肥胖、扁桃体或腺样体 肥大, 舌体肥大, 颈围增大, 颅面部畸形
上气道压力过大或上气道畸形, 上气道塌陷 的风险 ↑
血管因素: 仰卧位睡觉引起 夜间嘴侧液体移位
周围组织与压力 ↑à上气道阻塞
多导睡眠描记术
没有气流,但持
续通气
呼吸浅慢或 呼吸暂停
反常呼吸 吸气时胸壁凹陷, 腹部膨隆
持续通气以抵抗气道 闭合
上气道塌陷导致空气进
入气道受阻
腹膜腔负压↑ 静脉血回流右心室阻力↑
右心房心肌细胞拉伸 à心房利钠肽分泌 (ANP)
ANP抑制肾集合管的上 皮Na+通道(ENaC)对 Na+重吸收à Na+排出
Na+排出量↑ à 水排出量 ↑
睡眠时全部
或部分上呼
吸道阻塞
肺内PO2 ̄ 且 PCO2↑ à CO2 及 O2在肺和动脉 间的扩散梯度 ̄
↑ PaCO2, ̄ PaO2
呼吸性酸中毒 (血液中 [H+] ↑) à激活血管内皮电压
门控 K+
脑血管扩张为大 晨间头痛 脑提供足够的 O2
激活中央(延髓)和外周(颈动脉体)的化学感受器 呼吸驱动↑à呼吸肌活动 (呼吸做功 )↑
短暂的睡眠唤醒
通道 交感神经系统活动↑
全天缺氧 肺血管阻力↑
肺动脉高压
右心泵血以抵抗肺 动脉高压à 随着时 间推移,心肌向心 性肥大
肺心病(区别于左
心衰,右心衰是肺
动脉高压所致)
呼吸肌克服上气道阻力à 气道 明显恢复
睡眠过程不连续
白天的认知功能
及注意力 ̄
机动车辆事故风险↑
白天嗜睡
à 动脉收缩 全身血管阻力↑
高血压
血管内压力↑ à 血 管内皮和平滑肌发生 适应性改变
动脉壁增厚、硬化、失 去弹性à器官血液灌 注量 ̄ (如脑部)
缩写: PCO2:二氧化碳分压 PO2:氧分压 PaCO2:动脉二氧化 碳分压 PaO2:动脉血氧分压
通气过度 à呼出CO2 ↑ à PaCO2 ̄
呼吸驱动 ̄à 呼吸做功 ̄
复苏性鼾音
夜尿症
如:伊普沃斯嗜睡评分
>10
缺血性卒中
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年8月19日发表 www.thecalgaryguide.com, 2022年5月31日更新")
Status-Epilepticus
 Zhang Carlos Camara-Lemarroy* * MD at time of publication
Structural brain injury (stroke, trauma, hypoxia)
Drugs that lower seizure threshold
Antiseizure drug discontinuation
Alcohol, barbiturate, benzodiazepine withdrawal
Metabolic disturbance
Infection
See “Generalized Seizures”
Altered excitability and communication between neuronal structures
Isolated generalized seizures
Ongoing seizure activity and repetitive neuronal firing
Changes in receptor trafficking (seconds to minutes)
Changes in neuromodulator expression in hippocampus (minutes to hours)
Endocytosis of synaptic GABAA inhibitory receptors
↓ Number of inhibitory GABAA receptors
Progressive resistance to benzodiazepines (drugs that upregulate GABA receptors) as seizure continues
↑ Expression of excitatory peptides (substance P, neurokinin B)
Abbreviations:
• GABA- γ-aminobutyric acid
• NMDA- N-methyl-D-aspartic acid • AMPA- α-amino-3-hydroxy-5-
methyl-4-isoxazolepropionic acid
NMDA and AMPA excitatory receptors mobilize to synaptic membrane
↑ Number of excitatory NMDA and AMPA receptors
↓ Expression of inhibitory peptide (dynorphin, galanin, somatostatin, neuropeptide Y)
Seizure-induced failure of inhibitory mechanisms involved in seizure termination and increased neuronal excitability
Status Epilepticus (SE)
An abnormally prolonged seizure ≥ 5 minutes or 2+ sequential seizures without full recovery in between
↑↑ Glutamate release and activation of NMDA excitatory receptors
↑ Ca2+ entry into neurons
Mitochondrial dysfunction
↑ Reactive oxygen species (nitric oxide) production
Neuronal injury/death (↑ risk of developing chronic epilepsy)
↑ Autonomic activity
Intense, sustained muscle contractions
Persistent stimulus OR altered neuronal landscape
(i.e., Immune mediated)
Refractory SE:
SE that does not respond to 1st or 2nd line therapy
Prolonged seizures (≥30 mins) lead to failure of compensatory mechanisms
Circulatory collapse
↓ Cerebral blood flow
• Hypertension • Hyperglycemia • ↑ Cardiac
output
• ↑ Secretions
• Hypotension
• Hypoventilation
Energy demands > ATP produced through oxidative phosphorylation
Myocytes start utilizing anerobic glycolysis
↑ Lactic acid production
↑ Serum lactate
Sustained muscle activity produces body heat
Hyperpyrexia (axillary temperature ≥ 40° C)
Myocyte injury
Leakage of muscle contents into the circulation (Rhabdomyolysis)
↑ Serum creatine kinase
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 27, 2022 on www.thecalgaryguide.com")
pheochromocytoma-pathogenesis-and-clinical-findings
 Zhang Hanan Bassyouni* * MD at time of publication
↑ Blood pressure results in the activation of neural pain receptors
Sustained or paroxysmal 2o hypertension (↑ blood pressure)
Pallor
Tachycardia (↑ heart rate), palpitations
Diaphoresis (excessive sweating)
Hyperglycemia Weight loss, fatigue
Familial Disorders (10%)
E.g., Multiple Endocrine Neoplasm 2 Syndrome (MEN2) types A and B, Neurofibromatosis 1 (NF-1), Von Hippel Lindau Syndrome (VHL), familial pheochromocytoma
Dysfunction of various tumor suppressor and/or oncogene proteins
Uncontrolled proliferation of the chromaffin cells in the medulla of the adrenal gland(s)
Adenoma formation (10% bilateral)
Over-production of epinephrine and
norepinephrine from the adrenal adenoma(s) or extra- adrenal tumour (10%)
Detectable metanephrines (epinephrine/norepinephrine breakdown products) in both plasma and urine
Sporadic DNA mutations arising from
DNA damage from exposure to mutagens, malignancy (10%), or during DNA replication
Detectable mutations on the Von Hippel Linda (VHL), (Rearranged During Transcription) RET, (Succinate Dehydrogenase) SDH, and/or other tumour suppressor or oncogenes
Visible adrenal mass on CT scan Heart attack, stroke, or death (Note: These
tumors can be fatal therefore screening is essential in patients with adrenal masses or 2o hypertension)
Episodic hyper-activity of the sympathetic nervous system
Hyper-stimulation of G protein-coupled receptors involved in catabolic metabolic processes
Headaches
↑ Vasoconstriction of peripheral blood vessels
Hyper-stimulation of adrenergic receptors on cardiac myocytes
↑ Secretion from the eccrine sweat glands
Panic, tremor, anxiety
↑ Ability to mobilize glucose into the bloodstream through enhanced lipolysis, glycogenolysis and gluconeogenesis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 20, 2014, updated June 27, 2022 on www.thecalgaryguide.com")
Epilepsy Pathogenesis

Neoplasm
Metabolic
Inborn errors of metabolism
Inherited enzyme deficiencies
Neurodegenerative
Alzheimer’s Disease
Protein-rich plaque build-up and brain atrophy
Inflammation and formation of scar tissue irritates neural tissue
Infiltration of mass, grey matter irritation
Damage to the brain and subsequent alteration of neuronal circuitry
Neurotransmitter imbalances (i.e. ↑ glutamate, ↓ GABA, ↓ serotonin, ↓ dopamine, ↓ noradrenaline)
Abbreviations:
• HSV1 – Herpes Simplex Virus 1 • VZV – Varicella Zoster Virus
↑ Inflammatory cytokines (e.g. interleukin-6, tumor necrosis factor-α)
Altered neurogenesis and gliosis
Ion channel and receptor dysfunction causes imbalance of ion channel charges
Authors: Keerthana Pasumarthi Christopher Li Reviewers: Negar Tehrani, Ephrem Zewdie, Ran (Marissa) Zhang, Carlos R. Camara-Lemarroy* * MD at time of publication
Neurons fire in burst activity (referred to as paroxysmal depolarization shift) and often in groups (hypersynchrony)
Abnormal neural activities eventually create self-reinforcing circuits and transform neural network over time
Injuries from
falls, bumps, operating heavy machinery
Involuntary contractions Loss of consciousness
Post-ictal confusion
Recurrent seizures
Sudden Unexplained Death of Epilepsy Patient (SUDEP)
Loss of airway reflexes
Aspiration of saliva or food contents
Aspiration Pneumonia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 5, 2022 on www.thecalgaryguide.com")
burn-shock-pathogenesis-complications-and-clinical-findings

Endothelial cell lining in blood vessel walls is compromised
↑ Local vessel permeability
Shift of plasma + proteins from vessel into interstitial space
Direct vascular thermal injury (within burn wound)
↑ Production of circulating inflammatory mediators (ex. IL-1, IL-6, TNF-!)
↑ Systemic vessel permeability
↑ Circulating reactive oxygen species
Damage to DNA, proteins, and lipids throughout body, including myocardium (muscle cells of the heart)
↑ Myocardial stress
Myocardial dysfunction
↓ Cardiac contractility ↓ Stroke volume ↓ Cardiac output Cardiogenic
Shock
Refer to Cardiogenic Shock:
Pathogenesis, Complications and Clinical Findings
↓ Protein concentration in vessels causes ↓ intravascular oncotic pressure
Further shift of plasma from vessel into interstitial space (↑ interstitial proteins pull plasma into interstitium)
↓ Intravascular plasma
↑ RBCs per unit volume of plasma
↑ Systemic vasoconstriction to maintain blood pressure (↑ Afterload)
↓ Circulating blood volume leads to less venous return (↓ Preload)
↑ Hematocrit
Pitting edema (burned & unburned tissue)
↓ Circulating blood volume
Hypovolemic Shock
Refer to Hypovolemic Shock: Pathogenesis, Complications and Clinical Findings
Burn Shock: A complication of large burns causing end-organ hypoperfusion with resultant organ dysfunction
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 15, 2022 on www.thecalgaryguide.com")
Ischemic Stroke: Pathogenesis
 of basal or brainstem penetrating arteries
Large artery atherosclerosis
Cholesterol plaque ↓ diameter of intra- or extracranial vessel
Cardiac embolism
Blood clot in heart breaks free, travels to brain
Other
E.g. volume loss, severe infection
Unknown
E.g. 2 or more mechanisms
Modest ↓ in O2 at penumbra (see figure)
Authors: Mizuki Lopez Andrea Kuczynski Illustrator: Mizuki Lopez Reviewers: Sina Marzoughi Usama Malik Hannah Mathew Ran (Marissa) Zhang Andrew M Demchuk* Gary M. Klein* * MD at time of publication
Significant ↓ in O2 at ischemic core (see figure)
↑ Anaerobic metabolism ↓ ATP
Production
Dysfunction of Na+/K+ ATPase pump (for 1 ATP molecule, 3 Na+ moved out of cell, 2 K+ moved into cell)
H2O influx following Na+ Cerebral edema
Compression of vessels and surrounding tissue damages blood-brain barrier
↑ Permeability of damaged blood-brain barrier
Infiltration by peripheral immune cells
Immune cells release inflammatory cytokines
↓ Cerebral Blood Flow
Penumbra Ischemic core
Metabolic demands are greater than supply of ATP
Cell death
Microglia (resident neural immune cells) activate to clean dead cell debris
Microglia release inflammatory cytokines (TNFα, IFγ, IL-1β)
Cytokines lead to astrocyte activation (support cells for neurons)
Astrocytes release more inflammatory cytokines
Inflammation of brain tissue
↑ Na+, Ca2+ influx, K+ outflux
↓ Glutamate (excitatory neurotransmitter) reuptake by astrocytes (support cells for neurons)
↑ Glutamate in extracellular fluid
Spreading depolarization from core (unclear mechanism)
Activate biochemical pathways including glutamate receptor activation
↑ Glutamate activity
Activate glutamate receptors that conduct Ca2+
↑ Ca2+ influx into neuron
Activation of catabolic proteases, lipases, nucleases in neuron
Dysfunction of neuronal protein synthesis and activity
Neuronal cell death
↑ Volume of dead (infarcted) brain tissue
Neurons depolarize and release glutamate
Reversal of Na+ Dependent Glutamate Reuptake Transporters on astrocytes (normally 3 Na++ 1 H+ + 1 glutamate into cell, for 2 K+ out)
↑ Glutamate in extracellular fluid
Stroke symptoms (e.g. weakness, slurred speech, visual field losses, autonomic dysfunction)
(see Ischemic Stroke: Impairment by Localization stroke slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 14, 2017; updated November 6, 2022 on www.thecalgaryguide.com")
Ischemic Stroke Impairment by Localization
 in respective blood vessels
Ischemia: ↓ blood flow
(See Ischemic Stroke: Pathogenesis slide)
Left hemisphere damage
Right hemisphere damage
Motor and sensory cortices of upper limb and face damage
Urinary incontinence Aphasia (inability to comprehend or produce
Ischemia in
the middle cerebral artery (MCA)
MCA divides into segments
language) (See Aphasia slide)
Left sided agnosia (visual perceptual deficits)
Contralateral hemiparesis (weakness on side of body opposite to injury) & sensory deficits, visual field deficits, aphasia, agnosia (inability to process sensory information), apraxia (motor planning deficits) & agraphia (inability to communicate by writing)
M1-MCA (sphenoidal segment)
M2-MCA (insular segment)
Ischemia in the posterior cerebral artery
Spares the lower extremity, affects the upper extremity and face
Lesion to frontal lobe (Broca area) Infarction of occipital cortex
Lesion to superior temporal gyrus of temporal lobe (Wernicke area)
No homonymous hemianopsia (one-sided visual field loss) Expressive Broca’s/motor aphasia (inability to produce language)
Contralateral homonymous hemianopsia
(visual field loss on opposite side)
Receptive Wernicke’s/sensory aphasia
(inability to comprehend language)
Sensory loss, memory loss, contralateral homonymous hemianopsia & alexia (reading difficulty)
Ischemia of the occipital lobe, posteromedial temporal lobes, midbrain & thalamus
Ischemia in the vertebral basilar artery
Ischemia in the basilar artery
Ischemia of brainstem & medulla
Ischemia of midbrain, thalami, inferior temporal & occipital lobes
Cranial nerve disorders: dysarthria (slurred/slowed speech) (IX, X), diplopia (double vision), facial numbness or paresthesia (VII), Foville’s syndrome (ipsilateral cerebellar ataxia), Horner's syndrome, (paresis of conjugate gaze and contralateral hemiparesis, facial palsy, pain & thermal hypoesthesia)
Motor deficits: Millard-Gubler syndrome (pons lesion), Raymond’s syndrome (ipsilateral abducens impairment, contralateral central facial paresis & contralateral hemiparesis), Wallenburg syndrome (sensory deficits in the contralateral limb, ipsilateral face), ataxia (abnormal gait), unilateral or bilateral sensory loss of position & vibration
Cranial nerve disorders: dysconjugate gaze (unpaired eye movements) (III, IV, VI), ipsilateral facial hypoalgesia (↓ pain sensitivity) (V), unilateral lower motor neuron face paralysis (VII), vertigo (spinning sensation), dysarthria (weak speech muscles) (IX, X)
Motor deficits: contralateral hemiparesis, quadriplegia (paralysis of all 4 limbs), contralateral limb hypoalgesia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published February 3, 2018, updated February 28, 2023 on www.thecalgaryguide.com")
Hemorrhagic Stroke
 Zhang Mao Ding Michael D Hill* Gary Klein* * MD at time of publication
Primary Intracerebral Hemorrhage (~75%)
Secondary Intracerebral Hemorrhage (~25%)
Amyloid Angiopathy
Amyloid deposits in blood vessels and weakens vessel walls
Hypertension
Lipohyalinosis (lipid and protein aggregation in arterial walls) weakens blood vessels
Unknown
Aneurysm
Dilation of a weakened blood vessel
Drugs (e.g., cocaine, crystal meth, decongestants, anticoagulants)
Vascular Malformations
Note: the pathophysiology and exact mechanism is not well known
Release of toxic blood plasma components (coagulation factors, immunoglobins)
Red blood cell lysis
Cytotoxic hemoglobin (heme, iron) release
Fenton-type free radical generation (Fe(II) + H2O2 → Fe(III) + OH− + OH•)
Oxidative damage to carbohydrates, lipids, nucleic acids, and proteins in brain
Necrosis of hypoxic brain tissue
Neurological signs: focal motor weakness, aphasia, vision loss, sensory loss, imbalance/incoordination, altered LOC
Rupture of blood vessel(s) Accumulation of blood → hematoma formation
↓ Cerebral tissue perfusion (↓ O2 availability)
↓ Mitochondrial oxidative phosphorylation (final step in aerobic glucose metabolism)
↓ Adenosine triphosphate (ATP) production
↑ Anaerobic glucose metabolism → ↑ Cerebral lactate production
Cerebral lactic acidosis Impaired cellular metabolism Death of neurons and glia
Microglia clear debris and release inflammatory markers (TNFα, IFγ, IL-1β)
↑ Endothelial cell apoptosis and ↑ blood-brain barrier permeability
Cerebral edema
Increased intracranial pressure: papilledema, sudden headache, non-reactive pupils, ↓ level of consciousness (LOC), nausea/vomiting
Astrocytes release glutamate (main excitatory neurotransmitter)
Activation of neuronal metabotropic glutamate receptors
↑ Ca2+ influx into neurons
Excitotoxicity (excess stimulation of glutamate receptors leading to neuronal death)
Dysfunction of Na+/K+ ATPase pump (moves 3 Na+ out of cell and 2 K+ into cell) on neurons
↓ Na+ efflux and ↓ K+ influx
Neuronal membrane potential becomes less negative (closer to threshold potential)
Neurons depolarize → ↑ Glutamate release
General findings: Seizures, lethargy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published June 6, 2018, updated February 28, 2023 on www.thecalgaryguide.com")
Coronary Artery Bypass Graft CABG Indications
: Indications
Author: Breanne Gordulic Reviewers: Miranda Schmidt Ben Campbell Sunawer Aujla Angela Kealey* * MD at time of publication
Symptomatic multivessel (≥ 3 vessels) coronary artery disease (MVCAD) or complex MVCAD
Acute coronary syndrome (ACS)
Left main coronary artery disease
Multivessel (≥ 3 vessels) CAD and diabetes
Cardiac surgery required for other pathology
Multivessel CAD, LV dysfunction and congestive heart failure (CHF)
Complex CAD includes stenosed vein grafts, bifurcation lesions, calcified lesions, total occlusions, ostial lesions
STEMI initial treatment is PCI/thrombolysis
CABG outcomes compared to percutaneous coronary intervention (PCI) in MVCAD include ↑ survival in diabetes, ↑ survival with LV dysfunction, ↓ repeat revascularization, ↓ myocardial infarction, ↓ stroke
↑ Risk of failure in complex CAD with PCI
Rapid reperfusion to myocardium most important in STEMI to decrease myocardial damage
CABG can be considered for residual stenoses 6-8 weeks later
NSTEMI or unstable angina (UA) with MVCAD involving at least three vessels including the proximal left anterior descending (LAD)
Left main coronary artery divides into left anterior descending (LAD) and left circumflex (LCx) which supplies 2/3 of myocardium
↑ Survival Myocardial infarction from left main artery occlusion Death
Left main stenosis
Ventricular dysrhythmias
Ongoing ischemia
LV dysfunction Hemodynamic instability
↑ risk of PCI
CABG has mortality benefit
↓ Number of operations
↑ Risk of cardiovascular disease in diabetes
Revascularization indicated along with other cardiac surgery
Multivessel CAD with >90% stenosis and CHF
LV ejection fraction <35%
↑ Risk of atherosclerosis from hyperglycemia and dyslipidemia
CABG bypasses several atherosclerotic plaques in coronary arteries
↑ Durability
↑ Complete perfusion
Valve stenosis or regurgitation Septal defect
Aortic root or arch pathology
Combination procedure
Evidence of ischemia at rest
Evidence of
impaired LV function at rest
↓ All-cause mortality in CABG vs medical management
Chronic obstructive pulmonary disease
Abbreviations:
• ACS- acute coronary syndrome. Acute reduction in
blood flow to heart muscle resulting in cell death. • CAD- coronary artery disease. Narrowing or blockage of the coronary arteries by plaque
• NSTEMI- myocardial infarction (heart attack) with no ST elevation on electrocardiogram
• PCI- percutaneous coronary intervention. A balloon tipped catheter is used to open blocked coronary arteries; a stent may be placed.
• STEMI- myocardial infarction with ST segment elevation on electrocardiogram
Consider revascularization (restore blood flow to blocked or narrowed blood vessels) of coronary arteries to increase perfusion to myocardium (heart muscle)
Coronary artery bypass graft recommended
Assess surgical risk and comorbidities with evaluation by heart team that includes both a cardiac surgeon and interventional cardiologist (SYNTAX Trial)
Individual management plan for patients with comorbidities that increase mortality
Frailty
Chronic Renal Failure
↑ Inflammation and deregulated angiogenesis affects all organ systems
↓ Physiologic reserve and ↓ ability to recover from acute stress
↑ Pneumonia
↑ Respiratory and Renal Failure
↑ Stroke
↑ In hospital mortality
↓ Survival two years after surgery
Use Society of Thoracic Surgeons Score, EuroSCORE, or SYNTAX II Score to predict patient outcome with anatomy, disease severity, and preoperative characteristics
Coronary Artery Bypass Graft
Surgery to take healthy blood vessels from the body and connect them proximally and distally to blocked coronary arteries
Cardiopulmonary bypass, fluid overload, ↑ renal vasoconstriction and ↓ renal oxygenation from rewarming
Kidney injury
↑ End stage kidney disease
Blood flow restored to
ischemic myocardium
↓ Angina
↑ Quality of life ↑ LV function ↑ Survival
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 12, 2023 on www.thecalgaryguide.com")
Approach To Dementia

Authors: Iqra Rahamatullah Mahrukh Kaimkhani
Reviewers: Yvette Ysabel Yao Mao Ding Gary Michael Klein* *MD at time of publication
1) Changes noticed?
Modest ↓cognitive performance from previous, DOES NOT interfere with daily independence
MILD COGNITIVE IMPAIRMENT
More pronounced ↓cognitive performance from previous, DOES interfere with daily independence
MILD TO MODERATE DEMENTIA
↓Cognitive performance, difficulty with ≥1 basic activities of daily living (ADL) or ≥2 instrumental ADLs
MODERATE TO SEVERE DEMENTIA
DEMENTIA
Fluctuating course, acute onset, inattention WITH either disorganized thinking or altered level of consciousness
DELIRIUM
2) Is it dementia?
Normal, age-related: ↓focus, ↓cognitive speed, ↓reaction time, ↓memory
NORMAL COGNITIVE DECLINE
3) What is the cause of the dementia? (main causes discussed here)
Loss of cognitive functioning, including memory, language, problem solving, and other thinking abilities, that interferes with independence in everyday activities
Beta-secretase cleaves beta amyloid protein
Atherosclerosis or thrombosis
Misfolded alpha- synuclein
Toxic beta amyloid plaque and tau tangle (sticky) formation
Ischemia to areas of brain (strokes)
Build ups and deposition within neurons (Lewy bodies)
Disrupted signaling, inflammation, hippocampal and cerebral impairment
Necrosis of brain tissue in areas impacted by strokes
Neuronal impairment and atrophy (especially in substantia nigra)
Neuronal atrophyàfrontal + temporal lobe atrophy
Progressive atrophy of basal ganglia and dorsal striatum + lateral ventricles expanding
Death of dopaminergic neurons in substantia nigra
Alzheimer’s Dementia
Vascular Dementia
Lewy Body Dementia
Frontotemporal Dementia
Huntington’s Disease
Parkinson’s Disease
↓Memory, ↓learning, ↓language skills, disorientation, inattention
Total debilitation, fatal infections
Findings vary depending on area
Step-wise worsening impairment
Parkinsonism, hallucinations, REM- sleep behavior disorder
Total debilitation, dependence
Personality and behavioral changes
Mental status changes
Chorea, ↓cognition, mood changes
Aspiration, dementia, suicide
Resting tremor, rigidity, anosmia
Depression, dementia, falls
Abnormal protein inclusions and tangles (usually tau) form in neurons
Autosomal dominant disease (with anticipation) with ↑CAG repeats in Huntingtin gene
Genetic mutations, environmental exposures, or idiopathic cause
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 17, 2023 on www.thecalgaryguide.com
Approach to Dementia/Major Neurocognitive Disorder (NCD)
Authors: Iqra Rahamatullah Mahrukh Kaimkhani Reviewers: Yvette Ysabel Yao
Fluctuating course, acute onset, inattention WITH either disorganized thinking or altered level of consciousness (LOC)?
DELIRIUM
1) Changes noticed?
2) Is it dementia?
Normal, age-related: ↓focus, ↓cognitive speed, ↓reaction time, ↓memory
NORMAL COGNITIVE DECLINE
Modest ↓cognitive performance from previous, DOES NOT interfere with daily independence
MILD COGNITIVE IMPAIRMENT
More pronounced ↓cognitive performance from previous, DOES interfere with daily independence
MILD TO MODERATE DEMENTIA
↓Cognitive performance, difficulty with ≥1 basic activities of daily living (ADL) or ≥2 instrumental ADLs
MODERATE TO SEVERE DEMENTIA
3) What is the cause of the dementia? (main causes discussed here)
Beta-secretase cleaves beta amyloid protein
Atherosclerosis or thrombosis
Misfolded alpha-synuclein
Toxic beta amyloid plaque and tau tangle (sticky) formation
Ischemia to areas of brain (strokes)
Build ups and deposition within neurons (Lewy bodies)
Disrupted signaling, inflammation, hippocampal and cerebral impairment
Necrosis of brain tissue in areas impacted by strokes
Neuronal impairment and atrophy (especially in substantia nigra)
Neuronal atrophyàfrontal + temporal lobe atrophy
Progressive atrophy of basal ganglia and dorsal striatum + lateral ventricles expanding
Death of dopaminergic neurons in substantia nigra
Alzheimer’s Dementia
Vascular Dementia
Lewy Body Dementia
Frontotemporal Dementia
Huntington’s Disease
Parkinson’s Disease
↓Memory, ↓learning, ↓language skills, disorientation, inattention
Total debilitation, fatal infections
Findings vary depending on area
Step-wise worsening impairment
Parkinsonism, hallucinations, REM- sleep behavior disorder
Total debilitation, dependence
Personality and behavioral changes
Mental status changes
Chorea, ↓cognition, mood changes
Aspiration, dementia, suicide
Resting tremor, rigidity, anosmia
Depression, dementia, falls
DEMENTIA
Loss of cognitive functioning, including memory, language, problem solving, and other thinking abilities, that interferes with independence in everyday activities
Abnormal protein inclusions and tangles (usually tau) form in neurons
Autosomal dominant disease (with anticipation) with ↑CAG repeats in Huntingtin gene
Genetic mutations, environmental exposures, or idiopathic cause
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 17, 2023 on www.thecalgaryguide.com")
Mitral Regurgitation Pathogenesis and clinical findings

Myocarditis
Left ventricular dilation displaces papillary muscles
Dilation of the Tethering of mitral valve annulus chordae tendineae
↑ Volume and pressure in left atrium
↑ Volume pushed back into left ventricle
Dilated left ventricle
Apical impulse on palpation and auscultation
↓ Forward flow of blood out of heart
Blood backs up into pulmonary circulation
↑ Intravascular hydrostatic pressure in pulmonary vessels
Fluid extravasates out of vessels and into the lungs
Papillary muscle rupture
Mitral valve leaflets flail
Mitral valve prolapse
Structurally abnormal valve
Connective tissue disorders
Weak valve leaflets
Rheumatic heart disease
Dilatation of the mitral valve annulus, inflammation of leaflets
Infective endocarditis
Vegetations form on valve leaflets
Mitral Regurgitation
Blood consistently flows backward throughout systole
Holosystolic murmur, radiates to axilla, ↑ with afterload (e.g. making a fist)
Backflow of blood from left ventricle to left atrium due to impaired mitral valve closure
S3 heart sound
Myocardial remodeling
↓ Muscle efficiency
↓ Left ventricle systolic function
↓ O2 saturation, tachypnea, wheeze, ↑ work of breathing, crackles, frothy sputum (if severe)
Congestive heart failure
↓ Stroke volume ejected into aorta
↓ Cardiac output
↓ Organ perfusion ↓ O2 to kidney
Activation of renin-angiotensin- aldosterone system
↑ Reabsorption of water by kidneys
↑ Intravascular hydrostatic pressure systemically
Peripheral edema
Injury to kidney parenchyma
↓ ability for kidney to clear creatinine
↑ Serum creatinine
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 3, 2018, updated Oct 15, 2023 on www.thecalgaryguide.com")
Sustained Monomorphic Ventricular Tachycardia Clinical findings
 or a ventricular ectopic focus with increased automaticity. Refer to Sustained Monomorphic Ventricular Tachycardia: Pathogenesis slide for more details.
Authors: Rahim Kanji Reviewers: Stephanie Happ, Raafi Ali, Derek Chew* * MD at time of publication
The sinoatrial node continues to depolarize the atria while the ventricles depolarize independently and more rapidly
Heart rate > 100 beats per minute
The re-entrant circuit/ectopic focus uniformly and consistently depolarizes ventricular myocytes
Occasionally, a sinoatrial impulse conducts to the ventricles
Loss of coordination between the contractions of the atria and ventricles
ECG Finding: AV Dissociation
The impulse conducts normally through the His-Purkinje pathway and coincides with abnormal ventricular depolarization
ECG Finding: Fusion beat
Patient feels a forceful and rapid heart rate
Palpitations
Right atrium periodically contracts against a closed tricuspid valve
Cannon A waves (intermittent irregular jugular venous pulsations with large amplitudes)
↓ Ventricular filling time
↓ Preload
↓ Stroke volume cardiac output
Inadequate perfusion to organs
ECG Finding: Uniform morphology of QRS complexes
Direct myocyte-to- myocyte spread of the electrical impulse proceeds slower than an impulse conducted via the His-Purkinje pathway
ECG Finding: Wide QRS complexes (≥ 120 milliseconds)
The impulse conducts normally through the His-Purkinje pathway in between abnormal ventricular depolarizations
ECG Finding: Capture beat
Muscles and other organs
General malaise
Heart
Chest pain
Brain
Presyncope/ syncope
Inability to adequately respond to increased cardiac demand
Shortness of breath
Hemodynamic collapse
Sudden cardiac arrest
Death
Hypotension
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 22, 2023 on www.thecalgaryguide.com")
Statins Mechanisms and Side Effects

↓ Coenzyme Q10 (ubiquinone)
↑ Mitochondrial superoxide
↓ Hepatic membrane stability
↓ Conversion of HMG-CoA to mevalonic acid
↑ Hepatic VLDL uptake
↓ Hepatic apolipoprotein B-100 secretion
↓ Oxidative phosphorylation
Impaired mitochondrial function
↑ Liver enzyme leakage
↓ Mitochondrial ATP production
↑ Aminotransferases enzymes in liver
↑ Clearance of
LDL cholesterol from bloodstream
Myopathy/ myalgias (muscle aches)
Hepatotoxicity
↓ Circulating LDL cholesterol
↓ LDL, ↑ HDL, ↓ TG
↓ Hepatic cholesterol synthesis
↓ VLDL synthesis
↑ Cell surface LDL receptor expression
Statins
First line therapy for treating hypercholesterolemia (↑ LDL cholesterol in blood) Common examples: rosuvastatin, atorvastatin, simvastatin, pravastatin, etc.
↑ Apolipoprotein AI production & ↑ hepatic HDL neogenesis
↓ TG
↑ HDL
↑ Vasodilation
↓ C-reactive protein
↓ Impacts of coagulation cascade
↓ Atherosclerosis (plaque along walls of blood vessels)
↓ Cardiovascular disease & mortality
Pleotropic effects (i.e. non lipid related effects)
Abbreviations:
HMG-CoA – Hydroxymethylglutaryl-CoA LDL – Low-density lipoprotein
VLDL – Very low density lipoprotein HDL – High density lipoprotein
TG – Triglycerides
Inhibition of synthesis of isoprenoid intermediates in the mevalonate pathway
↑ Nitric oxide activity ↓ Inflammation
↓ Tissue factor expression
↓ Macrophage proliferation
↓ Tissue factor (promotes macrophage mediated thrombus formation)
↑ Blood flow & endothelial function
↓ Thrombin generation
↓ Metalloproteinases expression
↑ Inhibition of metalloproteinase-1
↓ Thrombogenicity (production of blood clot/thrombus)
Plaque stabilization (↓ risk of atherosclerotic plaque rupture, myocardial infarction, and stroke)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Physiological Outcome
Published July 9, 2017, updated Nov 6, 2023 on www.thecalgaryguide.com")
Death Cardiovascular Respiratory and Neurologic Mechanisms

Hypoxemia (Type I Respiratory Failure): low dissolved oxygen in blood (PaO2)
Lungs can’t oxygenate blood fast enough
Lungs can’t rid blood of CO2 fast enough
Hypercapnia / hypercarbia (Type II Respiratory Failure): elevated dissolved CO2 in blood (PaCO2)
Cerebral vasodilation
Toxins: e.g. cyanide, pesticides, arsenic Severe anemia
Distributive problems:
Systemic inflammation (sepsis, anaphylaxis, pancreatitis), adrenal insufficiency, vasodilatory drugs
Obstructive problems: Cardiac tamponade*, tension pneumothorax* or massive pulmonary embolism*
Hypovolemic* problems (low blood volume): Hemorrhage, dehydration, widespread skin disruption or burns
Cardiac valve dysfunction
Myocardial infarction* or cardiomyopathy
Cardiac arrhythmia or heart block
Disturbed electrical activity in cardiomyocytes
Peripheral metabolic disturbances
Hypokalemia*, Hyperkalemia* Acidosis* (including renal failure) Hypothermia*
Toxins* (e.g. cocaine, beta blockers, tricyclics) Severe thyroid derangement
Inappropriate systemic vasodilation
Adjacent forces impair heart filling
Low cardiac preload
Low stroke volume (SV; depends on valves, contractility, preload)
Decreased systemic vascular resistance (SVR)
Low blood pressure (BP = CO x SVR)
Decreased cardiac output (CO = SV x HR)
Disseminated intravascular coagulationàwidespread thrombi that occlude blood flow (also causes hemorrhage, see relevant box at left)
Methemoglobinemia: some hemoglobin gets stuck in a state that can’t carry O2
Hemoglobin has reduced capacity to carry or release O2
Drugs: e.g. dapsone, nitrates
Carbon monoxide poisoning
Circulatory collapse / shock: inadequate perfusion of tissue with blood
Respiratory collapse: blood has insufficient useable O2 content
Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)
Hypoxia*: inadequate O2 delivery or utilization in tissues
Hypoxia creates metabolic disturbances that impair cardiac cells. Alternatively, any of the preceding conditions marked with (*) can directly trigger cardiac arrest first
Pulseless Electrical Activity (PEA): organized activity on ECG with no cardiac output (can be preceded or mimicked by pseudo-PEA, in which there is still some output on ultrasound)
Low atmospheric pressure or oxygen content Severe lung disease
Asthma, COPD, interstitial lung disease, congestive heart failure, pulmonary hypertension, pulmonary embolism, lung collapse / atelectasis
Acute respiratory distress syndrome
Pneumonia, aspiration pneumonitis, inhalational injury, systemic inflammation, drowning
Severe hypoventilation
Respiratory fatigue, advanced COPD, chest wall disorders, neuromuscular disorders, upper airway obstruction, toxins (e.g. opioids, botulism)
Can degenerate at any time
Asystole: no cardiac electrical activity or output
Death
Respiratory arrest: cessation of breathing
Inability to protect airway
Decreased level of consciousness
Note
This is a broad overview of the many scenarios that can result in death. For detailed explanations of the various disease mechanisms, refer to the corresponding slides.
* = reversible causes of cardiac arrest (Hs and Ts)
Author:
Ben Campbell
Reviewers:
Yan Yu*
Huma Ali*
* MD at time of publication
Bradycardia
(low heart rate, HR)
Unopposed parasympathetic stimulation of heart (can also cause vasodilation, see Distributive problems)
Disruption of spinal cord sympathetic control
Injury to cervical or upper thoracic spinal cord
Irreversible cessation of cardiac, respiratory, and brain function
Prolonged seizure initially causes increased cardiovascular activity, until the system fatigues
Disruption of respiratory control center in medulla
Expanding skull contents squeeze brainstem (herniation)
Increased intracranial pressure
Edema from intracranial hemorrhage, trauma, brain mass
Edema, inflammation, hypoxia and/or metabolic derangements cause diffuse neuron dysfunction
Central nervous system infection
Dementia, particularly with delirium
Massive ischemic stroke
Seizure
activity prevents or alters breathing
Metabolic disturbances that affect the central nervous system Hypoglycemia Hypocalcemia, hypercalcemia Hyponatremia, hypernatremia Uremia
Acute liver failure (hyperNH4) Many drugs / toxins Withdrawal (e.g. EtOH)
Status epilepticus
Brainstem lesion (e.g. stroke, neoplasm, inflammatory)
Nervous System Insult
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 11, 2023 on www.thecalgaryguide.com
Respiratory System Insult
Cardiovascular System Insult Cardiogenic problems")
Complication of MI - Acute Mitral Regurgitation
 commonly in the posterior descending artery
Plaque ruptures
Exposed plaque contentsàPlatelet adhesion and aggregation
Artery becomes partially or completely occluded
Mitral Regurgitation**
(Back flow of blood from left ventricle to left atrium during systole)
↑ Left atrial pressure
Blood from left atrium backs up into pulmonary venous system
↑ Pulmonary venous pressure
↑ Hydrostatic pressure in alveolar capillaries
↑ Fluid leak from alveolar capillaries to interstitium (pulmonary edema**)
↓ Gas exchange
Attempt at
physiologic compensation à ↑ Respiratory rate
Tachypnea
Holosystolic murmur
Heard loudest over the mitral valve (5th intercostal space, mid-clavicular line), with radiation to the axilla
↑ Volume of blood to left ventricle during diastole
↓ Blood supply to the portion of the ventricle that supports the papillary muscle à↓ Muscle movement
Left ventricle dysfunction
↓ Blood supply to the posterior medial papillary muscle
Cell death (myocardial infarction)
Papillary muscle ischemia (muscle is intact but cannot contract)
↑ Blood in right atriumà↑ Blood in superior vena cava
↑ Blood in internal jugular vein
↑ Jugular venous pressure (JVP)
Redistribution of interstitial fluid when lying flat (reduced effect of gravity)
↓ Forward blood flow from left ventricle to aorta
↓ Stroke volume (SV)
↓ Cardiac output (CO) CO = SV x HR (heart rate)
Sympathetic nervous system attempts to physiologically compensate
↑ Heart rate
Tachycardia
↓ Blood pressure (BP) because BP = CO X SVR (systemic vascular resistance)
Cardiogenic shock**
Papillary muscle rupture
Papillary muscle unable to provide adequate tension on mitral valve
Mitral valve unable to stay closed during systole
Orthopnea
Difficulty breathing
Dyspnea
Paroxysmal nocturnal dyspnea
**See corresponding Calgary Guide slides for more details
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com")
Aspiration Pneumonia
 (e.g. stroke)
Altered level of consciousness and impaired cough/clearance
Tube Poor Alcohol and Substance Medications Neurologic diseases
Esophageal and gastric motility disorders
Impaired swallowing
Chronic obstructive pulmonary disorder
feeding oral health
Bacteria adhere to epithelial surfaces and ↑ risk of airway and lung bacterial colonization
Aspirated oropharyngeal and gastric contents can also contain bacteria
↓ Elimination and clearance of foreign bacteria from airway and lung
Macroaspiration (large volume aspiration) of oropharyngeal bacteria, during eating and drinking
Bacteria and fluid fill bronchi and alveolar space
Aspiration Pneumonia
Alterations to lung microbial flora
An infectious lung process caused by inhalation of foreign bacterial and oropharyngeal and gastric contents
Aspiration of acidic fluid and pneumonia causative pathogen (typically anaerobes or bacteria in normal oral flora) with resultant inflammation
Infiltrate develops in a gravity-dependent pattern in patches around bronchi segments.
Produces proinflammatory cytokines, (e.g. tumor necrosis factor-alpha, and interleukin-1)
Hypothalamic production of prostaglandin E2 results in thermogenesis
Fever
Authors: Luiza Radu
Reviewers: Mao Ding, *Yan Yu, *Jonathan Liu *MD at time of publication
Aspiration to the right lung more common due to large diameter and more vertical orientation of the right main bronchus
Crackles and ↑ lung vibrations (fremitus) on auscultation
Productive Cough
Impaired alveolar gas exchange
Chemoreceptor detection of ↓ pO2 triggers
↑ ventilation
Hypoxemia
Dyspnea
Consolidation in lower lobes (particularly superior segments) and posterior segments of upper lobes
If untreated, a
pus-filled lung cavity develops (e.g. abscess)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 11, 2024 on www.thecalgaryguide.com")
Cranial Nerve IV Palsy

Dysgenesis (defective development) of CN IV
Microvascular Disease (e.g. Stroke)
Damage or occlusion (complete or partial blockage) to the blood vessels supplying CN IV
Trauma
Temporary or permanent damage to the nerve fibers
Neoplasm
Metastasis (e.g. Leptomeningeal)
Compression of the nerve fibers along the nerve tract
Primary (e.g. Schwannoma)
Tumor develops new blood vessels that redirect blood flow to the malignancy, away from the nerve
Ischemia of CN IV
Infection (a rare cause) (e.g. Ehrlichia chaffeensis, Tuberculosis meningitis)
Infectious process in the subarachnoid space
Damage to axons of CN IV
Cranial Nerve (CN) IV Palsy
Superior oblique musculature weakness due to CN IV dysfunction
Lesion to the fascicle of CN IV (extending from midbrain to cavernous sinus)
Impaired ability to conduct motor commands from nucleus to superior oblique muscle in the eye
Weak superior oblique innervation
Difficult abduction and intorsion of the eye
Contralateral superior
oblique weakness
Lesion to the nucleus of CN IV (located in the midbrain)
Disturbed signal production occurring prior to demarcation of fibers to contralateral side
The pathophysiology above can cause damage to structures surrounding CN IV in the midbrain
Impacting ipsilateral sympathetic chain descending from the
hypothalamus prior to reaching the superior cervical ganglion
Authors:
Shahab Marzoughi Reviewers:
Sunawer Aujla
Yvette Ysabel Yao
Yan Yu*
Gary Michael Klein*
* MD at time of publication
Vertical/oblique Diplopia (double vision)
Hypertropia (one eye is deviated upward compared to the other)
Perinaud’s Syndrome (upgaze palsy, convergence retraction nystagmus, and pupillary hyporeflexia)
See relevant Calgary Guide slide on Parinaud’s Syndrome
Loss of eye muscle movement coordination and function of other structures relating to gait
Ataxia
Ipsilateral Primary Horner’s Syndrome (miosis, anhidrosis, ptosis)
See relevant Calgary Guide slide on Horner Syndrome
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 16, 2024 on www.thecalgaryguide.com")
Eisenmenger Syndrome

↑ Shear stress and circumferential stress on the pulmonary arteries and arterioles
Atrioventricular septal defect
Truncus arteriosus (Only one common artery arises from the heart rather aorta and pulmonary artery)
Long-standing “right-to-left” shunt with too much pulmonary blood flow
Structural changes occur in pulmonary arteries and arterioles to adapt to ↑ flow and pressure
Hypertrophy of the smooth muscles (media) of pulmonary arteries and arterioles Thickening of the intima (innermost layer) of pulmonary arteries and arterioles
↑ Pulmonary vascular resistance (pressure in the pulmonary arteries)
Pressure within the right ventricle gradually ↑
Right ventricular pressure is equal to, or exceeds left ventricular pressure
Shunt changes from left-to-right to right-to-left “Right-to-Left” Shunt
De-oxygenated blood originating from the right ventricle bypasses the lungs and goes into systemic circulation ↓ Oxygen delivery to tissue across the body
Pulmonary hypertension
(mean pulmonary artery pressure at rest ≥ 25mmHg)
Right ventricular hypertrophy (enlarging)
Hypertrophied right ventricle cannot contract effectively
Right ventricle loses ability to pump blood efficiently
Right heart failure
Megakaryocytes (platelet precursors) are shunted away from the capillary beds of the lungs, where they usually get fragmented into platelets
Chronic central cyanosis (generalized bluish discoloration)
Induction of vascular endothelial growth factor (VEGF) in fingers
Terminal digit clubbing (uniform swelling of the fingers and toes)
Hypoxemia (<90% O2 saturation)
Thrombocytopenia (↓ platelet count) Spontaneous bleeding events
Body tries to compensate for ↓ O2 by ↑ oxygen-carrying capacity of the blood
Polycythemia (↑ in red cell count) and ↑ hemoglobin concentration
↑ blood viscosity Hypercoagulable and prothrombotic state
Not enough O2 to meet the body’s demands
Fatigue
Epistaxis (nose bleeds)
Minor (non-life-threatening)
Major (life-threatening)
Pulmonary hemorrhage
Dental bleeds
Menorrhagia (heavy periods)
Pulmonary Embolism (clot in pulmonary vessels) Stroke Deep vein thrombosis (clot in deep veins)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 5, 2024 on www.thecalgaryguide.com")
Circle of Willis Anatomy and Physiology

Anterior Cerebral Artery (ACA)
Ischemic stroke (brain damage due to ischemia)
Inadequate blood flow & oxygenation of brain tissue
Occlusion or narrowing
Supplies midbrain, thalamus, & occipital lobe
Posterior Cerebral Artery (PCA) Vertebral Arteries (VA)
Inadequate blood flow & oxygenation of brain tissue
Occlusion or narrowing
Supplies lateral portions of frontal, temporal & parietal lobes (upper extremity & facial regions of motor/sensory cortices)
Middle Cerebral Artery (MCA) P2 segment
A1 segment
Supplies the MCA & ACA
A2 segment
Collateral circulation redistributes blood flow to maintain continuous blood supply
Occlusion or narrowing of vessels within the Circle of Willis
Anterior Communicating Artery (Acomm)
Weakness in the blood vessel walls
Aneurysm formation causes mass effect (displacement) on nearby structures
Supplies BA & PCA, lateral medulla & cerebellum via posterior inferior cerebellar artery (PICA), & upper spinal cord via anterior spinal artery (ASA)
Basilar Artery (BA)
Supplies occipital lobe, cerebellum & brainstem
Thromboembolism (blood clot obstruction)
Inadequate blood flow & oxygenation of brain tissue
Ischemic stroke
Damage to the ventral pons
Locked-in syndrome (quadriplegia, loss of voluntary breathing & speaking, intact cognition & blinking)
Internal Carotid Arteries (ICA)
Posterior Communicating Artery (Pcomm)
Weakness in the blood vessel walls
Aneurysm formation causes mass effect (displacement) on nearby structures
Oculomotor nerve (cranial nerve III): double vision & absent pupil response to light
Legend:
Pathophysiology
Mechanism Sign/Symptom/Lab Finding Complications Published Nov 5, 2018, updated Apr 29, 2024 on www.thecalgaryguide.com
P1 segment
Ruptured aneurysm: subarachnoid hemorrhage
Inadequate blood flow & oxygenation of brain tissue
Hemorrhagic stroke (brain damage due to bleeding)
Optic nerve (cranial nerve II): ↓ visual acuity
Frontal lobe: headache & psychological changes
Authors: Josh Kariath, Rafael Sanguinetti Reviewers: Andrea Kuczynski, Luiza Radu Gary Klein* * MD at time of publication")
Sickle Cell Disease Pathogenesis Clinical Findings and Complications
 Liu Priyanka Grewal Reviewers: Alexander Arnold Luiza Radu JoyAnne Krupa Yan Yu* Lynn Savoie* * MD at time of publication
Hemoglobin S (HbS) variant formed instead of normal Hemoglobin A (HbA)
Hb electrophoresis shows approximately 45% HbS, 52% HbA (ααββ), 2% HbA
Hb electrophoresis shows approximately 90% HbS, 8% HbF, & 2% HbA .
No HbA present
(ααδδ), & 1% HbF (ααγγ;2 fetal hemoglobin)
Heterozygous: point mutation in one of the two chromosomes (Hb AS)
Sickle cell trait
(asymptomatic unless severely hypoxic)
Homozygous: point mutation in both chromosomes (Hb SS)
Sickle cell disease
An inherited blood disorder characterized by defective hemoglobin that leads to red blood cells sickling
2
Dehydration Hypoxemia
Acidosis
↓ Volume of RBC cytoplasm
↓ O2 Saturation of Hb
O morereadily 2
released from Hb in low pH environment
↑ Concentration of deoxygenated HbSinred blood cells (RBCs)
Hydrophilic glutamate→ hydrophobic valine substitution makes HbS less soluble in the cytoplasm & more prone to polymerization & precipitation in its deoxygenated state
↑ Concentration of deoxygenated Hb in RBC leads to ↑ polymerization rate Polymerized & precipitated HbS forms long needle-like fibers
RBC shape becomes sickled
Sickle cells on peripheral blood smear
Vaso-occlusion
(sickled RBCs lodge in small vessels, blocking bloodflow to organs & tissues)
Blockage of venous outflow
Occlusion of vessels in lungs ↑ pulmonary blood pressure
Fluid extravasates into interstitial tissue leading to pulmonary edema
Acute chest syndrome (chest pain, hypoxemia (↓blood oxygen), etc.)**
to the penis:
to the spleen:
Priapism (persistent, painful erection)
Splenic Sequestration (blood pools in spleenà splenomegaly & hypotension)
Extravascular hemolysis (macrophages in the spleen phagocytose sickled RBCs)
Normocytic anemia
↑Marrow erythropoiesis (RBC production) to compensate for hemolysis
Infarction of bone
Pain crises
If occurring in hands
Dactylitis (inflammation of digits)
Blockage of arteries ↓ oxygenation of organs & tissues
Vaso-occlusion of the splenic artery
Splenic infarction (↓ blood supply leads to tissue death)
RBC inclusions (structures found in RBCs) not removed by spleen
Howell-Jolly bodies (RBC DNA remnants) on blood smear
Vaso-occlusion of other arteries (cranial, renal, etc)
Stroke, renal failure
↑ RBC breakdown
↑ Unconjugated bilirubin released from RBC breakdown
RBC precursors (reticulocytes) are released into the blood stream
Reticulocytosis (increased number of immature red blood cells) on peripheral blood smear
Patient’s RBC level becomes dependent on increased marrow activity
Bone marrow infarction or viral infections (i.e. Parvovirus B19) suppresses bone marrow activity
Aplastic crises (profound anemia)
** See corresponding Calgary Guide slide(s)
↑ Serum level of unconjugated bilirubin
Some of the circulating unconjugated bilirubin deposits in the skin
Jaundice (yellowing of skin)
↑ Conjugation of bilirubin in liver
↑Amounts of conjugated bilirubin released into bile
Gallstone formation
Cholelithiasis (presence of gallstones in the gallbladder)
Spleen releases invasive encapsulated bacteria (eg. Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis) into circulation, which causes infections
Meningitis
Sepsis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 16, 2013, updated Apr 29, 2024 on www.thecalgaryguide.com")
Anesthetic Considerations in Pregnancy

↑ Progesterone serum levels
↓ Esophageal tone & sphincter pressure
↑ Aspiration risk >20 weeks gestation & during labor
Aspiration prophylaxis
Rapid sequence induction
Nonparticulate antacid prophylaxis (e.g., sodium citrate, famotidine)
Pre-operative fasting & gastric ultrasound to assess volume
Breathing
↑ Minute ventilation
↓ PaCO2 at baseline
Uterine artery vasoconstriction with maternal PCO2 levels exceeding 32 mmHg
Impaired uteroplacental perfusion
Maintain physiologic alkalosis, avoid maternal hypercapnia
Maintain
maternal arterial PCO2 28–32 mmHg
Avoid permissive hypercapnia
↑ Progesterone serum levels
Disproportionate ↑ in plasma volume
↓ Serum colloid osmotic pressure
Drug-specific alterations in absorption, distribution, metabolism & excretion (e.g. ↑ distribution of acidic drugs due to ↓ albumin; ↑ clearance of renally- metabolized drugs)
Optimize anesthetic dosing for altered pharmacokinetics
Adjust dosages based on drug recommendations
Circulation
↑ Maternal blood volume
Peripheral vasodilation
↓In systemic vascular resistance by 25–30%
↓ Blood pressure
↑Abdominal pressure
Compression of the aorta & inferior vena cava
Supine hypotension
Impaired uteroplacental perfusion
Fetal ischemia
Optimize
placental blood flow
Position patient on left side to maintain uterine displacement
Diaphragmatic elevation & lung compression
↓ Functional residual capacity
↑ Risk of rapid desaturation
Fetal hypoxemia
Maintain maternal & fetal oxygenation
Optimize positioning (e.g., patient on left side to maintain uterine displacement)
& supplement oxygen as needed
Heart rate ↑ 15-25%
↑ Cardiac output
Manifestations of significant blood loss are delayed
Avoid hypotension
↑ Stroke volume
Avoid fluid overload
Treat abnormal variation in blood pressure at lower values
Fetus
Requirement to assess & treat two patients
Achieve optimal anesthetic dosing for mother while maintaining fetus safety
Maintain oxygenation of both mother & fetus & ensure adequate uteroplacental perfusion
Consider fetal-drug transfer & adjust agent & dose accordingly
Monitor maternal vital sign & fetal heart rate
Utilize a multidisciplinary team (e.g., pharmacy, nursing, physical & occupational therapy)
Legend:
Pathophysiology
Mechanism
Goal
Management
Published July 5, 2024 on www.thecalgaryguide.com")
AVC Isquemico Patogenese

Epilepsy in Older Adults
, primarily ischemic stroke, intracerebral hemorrhage, subarachnoid hemorrhage
Ischemic and hemorrhagic injuries cause inflammation and nerve cell degeneration
Glial cells (astrocytes and oligodendrocytes) proliferate around the lesion area to repair the damaged tissue
Glial scar formation impedes neuronal reconnection and growth
Alzheimer’s or Vascular Dementia
Central nervous system disease (e.g. traumatic brain injury, prior meningitis, mass)
Medications associated with hyponatremia (e.g. diuretics, antidepressants, antipsychotics, etc.)
Cerebral edema
Increased intracranial pressure
Compression on structures and blood vessels
Sleep deprivation
Tau or amyloid deposition (abnormal protein aggregates in brain)
Small vessel disease
Increased delta wave activity
Heightened neural excitability
Decreased seizure threshold
Elevated stress hormones (e.g. cortisol)
Increased neuronal excitability and decreased inhibition
Areas of tissue death, white matter changes & cortical irritability
Structural and electrical brain changes
Epilepsy: Neurological disorder characterized by increased susceptibility to recurrent unprovoked seizures
Excessive, hypersynchronous & oscillatory network function Imbalance between excitatory and inhibitory activity
Resultant seizure activity
Atypical Seizure pattern; e.g. seem confused, stare into space, wander, make unusual movements, inability to answer questions
Often atypical location in brain (limbic or neocortical)
Focal seizures are more common than generalized
Postictal paresis can last for days & disorientation, hyperactivity, wandering and incontinence may persist for 1 week
Neurotransmitter dysregulation, neural network disruption, genetic factors, psychosocial factors
Psychiatric comorbidities
Authors: Anna Crone
Reviewers: Anika Zaman,
Rachel Carson, Raafi Ali, Luiza Radu, Gary Michael K Klein*
* MD at time of publication
Widespread structural changes and hippocampal atrophy
Dementia
Sub-optimal treatment results in ongoing and more frequent epileptic seizures
Status epilepticus (higher mortality among older adults)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")
Pulsus Paradoxus

Thoracic cavity expands
Lungs expand and intrathoracic pressure ↓
Physiologic:
↑ Venous return to right (R) heart
↑ R heart preload (volume of blood inside the ventricle right before it contracts)
↑ Blood pools in the right side of the heart
Obstructive lung diseases (e.g., COPD**, asthma**)
Hyperinflated lungs
↑ Stretching of pulmonary vessels at rest
On inspiration, ↑↑ stretching of pulmonary vessels
↑↑ Blood pools within pulmonary vasculature
↓↓ Flow to L heart
Pathologic: Constrictive pathologies (e.g., cardiac
tamponade**, constrictive pericarditis**) Decreased pericardial compliance
Constriction of ventricles
On inspiration, ↑ venous return to R heart (normal)
R ventricle unable to fully expand due to ↓ compliance
Septum bows into L ventricle
L ventricle unable to fully expand ↓↓ Filling of L heart
↓↓ L ventricular end diastolic volume
↓↓ L heart stroke volume ↓↓ Cardiac output Pulsus Paradoxus
Exaggerated ↓in systolic BP on inspiration (>10mmHg)
Air flows into the lungs
Pulmonary vessels are physically stretched/pulled
↑ Blood pools in pulmonary vessels
↓ Return of blood to left (L) heart
↓ L heart preload
↓ L heart stroke volume
↓ Cardiac output
Obstruction of superior or inferior vena cava (e.g., clot)
↓↓ Venous return to R heart at rest
↓↓ Right heart filling
↓↓ Blood flow to pulmonary arteries
Pulmonary embolism**
Clot occludes pulmonary arteries/ arterioles
↓↓ Flow to pulmonary veins
At rest, ↓↓ flow to L heart
On inspiration, ↓↓↓ flow to L heart
↓ Systolic blood pressure (BP) of < 10mmHg on inspiration
BP = cardiac output x systemic vascular resistance
**See corresponding Calgary Guide slides
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 21, 2013; updated Dec 3, 2024 on www.thecalgaryguide.com")
Polycythemia Vera Complications
: Complications
High numbers of cells & platelets ↑ blood viscosity
Polycythemia Vera
Hematological disorder in which JAK2 mutations in hematopoietic cells result in increased RBC production. See corresponding Calgary Guide slide “Polycythemia Vera: Pathogenesis”
↑ Blood cell volume
Presence of increased numbers of platelets creates a hypercoagulable and prothrombotic state
↑ Risk of venous & arterial thrombosis
↑ Systemic vascular resistance Impaired/“sluggish” blood flow
↓ Perfusion to small vessels and ↓ oxygen delivery to throughout body
Arterial clots in arms
and legs or in vessels leading to brain prevent oxygen delivery to cells
Systemic hypertension
↑ Turnover of hematopoietic cells (RBCs, WBCs, platelets)
Fatigue
Transient visual disturbances
Neurological symptoms (e.g. headache, dizziness, tinnitus, concentration problems)
Breakdown of nucleic acids during cell turnover ↑ uric acid levels in blood
Lysing cells release lactate dehydrogenase (LDH) into bloodstream
↑ Spleen activity to filter and dispose of old blood cells
Splenomegaly
Authors: Caitlin Bittman Noriyah Al Awadhi Yan Yu Peter Duggan* Reviewers: Maharshi Gandhi Kevin Zhan Michelle J. Chen Paul Ratti Merna Adly Crystal Liu Kareem Jamani* Man-Chiu Poon* Lynn Savoie* * MD at time of publication
Extramedullary hematopoiesis
Pancytopenia
Clots in the
portal vein, splenic vein, & mesenteric vein are unusual & highly suggestive of PV
Clots in cardiac arteries prevent O2 delivery to cardiac tissue
Myocardial infarction
Venous blood moves more slowly and is less pressurized compared to arterial blood. Combined with hypercoagulable state, clots are likely to form in deep veins (usually of the legs)
Deep vein thrombosis
Clot breaks off and
travels through the inferior vena cava & right heart into the pulmonary arteries
Pulmonary embolism
Stimulation fibroblasts in the bone marrow
Uric acid accumulates & precipitates in blood
Hyperuricemia
↑ Serum LDH
Limb ischemia
Ischemic stroke & transient ischemic attacks
Erythromelalgias (burning pain in the extremities and erythema due to poor perfusion and transient microvascular occlusion)
Compensatory vasodilation in the capillaries of the skin
Plethora/rusted or “ruddy” complexion, particularly noticeable on the face, palms, nailbeds, & mucous membranes
Gout
Uric acid stones
Advanced Disease Progression
Abnormal blood cells produced in PV release various growth factors and cytokines
Production of excess collagen and other fibrous materials
Hematopoietic cells in bone marrow replaced with fibrous tissue over time
Bone marrow increasingly unable to produce healthy blood cells
Myelofibrosis (rare type of chronic blood cancer; considered late-stage progression of PV characterized by bone marrow fibrosis)
Bone marrow failure
Chronic bone marrow hyperactivity leads to exhaustion and/or damage of hematopoietic cells
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 7, 2012, updated Feb 22, 2025 on www.thecalgaryguide.com")
Polymyalgia Rheumatica
 is s9ll poorly understood. PMR is a rheuma9c condi9on characterized
Author: Anna Bobyn Reviewers: Anika Zaman, Kevin Zhan Luiza Radu, Emily J. Doucette Glen Hazlewood* *MD at time of publication
by pain and s9ffness around the neck, shoulder, and pelvic girdle.
Non-Modifiable factors
Assigned female at birth:
3♀ : 1♂
Environmental factors
Age-Related Changes: PMR almost exclusively affects people >50
Polymorphisms:
(eg. HLA-DR1, Interleukin (IL)-1, IL-6, TNF⍺)
Infectious Triggers: Epstein-Barr virus, Mycoplasma pneumoniae, parvovirus
Link to Vaccina=ons:
COVID-19, influenza, respiratory syncy=al virus
Innate immunity involvement: Macrophages & dendri=c cells recognize & respond to unknown an=gen
Immune cells ↑ production of cytokines (IL-6, IFN-γ, TNF-α)
Adap=ve immunity involvement: No strong evidence of autoan=body role
Early CD4+ T cell ac=va=on & infiltra=on of T cells into vascular =ssue
Subclinical vascular inflammation, particularly of medium & large arteries
↑ Vascular Endothelial Growth Factor & micro-vasculariza=on
Vascular dysfunction, ischemia, edema, & sensitization of pain receptors
Systemic inflamma=on
Local inflamma=on of synovial membrane, joint bursae, & tendon sheaths
B cell dysregula=on (↓ naïve B cells, ↑ memory B cells)
↑ Serum inflammatory
markers (CRP & ESR)
↑ Risk of cardiovascular
events (heart attack, stroke)
Low-grade fever (37.2- 38°C)
↓ Passive & ac>ve range of mo>on
Bilateral morning stiffness lasting >30 minutes
Fa>gue & malaise
Muscle pain in proximal joints
(shoulder & pelvic girdle)
Development of Giant Cell Arteri>s**
(15-20% of PMR pa>ents)
**See corresponding Calgary Guide slide
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complica=ons
Published Mar 23, 2025 on www.thecalgaryguide.com")
Heparin-Induced Thrombocytopenia

Platelets aggregate
within the bloodstream
↓ Free unbound
platelets in bloodstream
Mild Thrombocytopenia:
platelet count between
100 x 109/L - 150 x 109/L
Fewer platelets
available for thrombosis
(formation of a
pathological blood clot)
Self limiting with
no thrombotic risk
Legend: Heparin-Induced Thrombocytopenia (HIT): Pathogenesis and clinical findings
Obesity Hypertension Macrovascular disease Hyperlipidemia
Heparin (often unfractionated)
complexes with platelet factor 4 (PF4)
on the platelet surface, due to
heparin’s negative charge & PF4’s
affinity for long-chain polysaccharides
Immune-Mediated:
Type 2 (within 5-15 days
of heparin administration)
Anti-heparin/PF4
Immunoglobulin G
antibodies binds to
the heparin-PF4
complex in the blood
Splenic macrophages
remove platelet-
immunoglobulin G
complexes in the spleen
Thrombocytopenia:
Platelet count < 100 x
109/L (though < 20 x
109/L should prompt
consideration of
other diagnoses)
↑ Vascular inflammation & endothelial
dysfunction activate platelets
Authors:
Kelle Edgar, Hadi Hassan
Sergio F. Sharif
Reviewers:
Haotian Wang, Jessica Asgarpour
Yan Yu*, Lynn Savoie*
Kareem Jamani*
* MD at time of publication
Activated platelets
release PF4
Anti-heparin/PF4
antibodies activate
adjacent platelets
Activated
platelets release
inflammatory
mediators
Circulating anti-
heparin/PF4 antibodies
bind adjacent cellular
targets
Anti-heparin/PF4
antibodies bind
endogenous heparan
sulfate on endothelium
Activated
endothelium
releases
procoagulants
thrombin &
tissue factor
Activated
platelets release
procoagulants
(factors
promoting blood
clotting)
Free platelets are
consumed from
formation of thrombi
Hypercoagulable state
(↑ risk of thrombosis)
↓ Platelets available
to clot at different
area of the body
Thrombosis in
coronary, peripheral
or cerebral arteries
Bleeding (rare)
Myocardial
infarction
Acute
ischemia
Stroke
Inflammatory
mediators disrupt
hypothalamic body
thermoregulation
Fever/
chills
Inflammatory mediators
promote vasodilation of
arterioles under the skin
↑ Blood to
surface of skin
Flushing of skin
Venous thrombosis
in lower leg or lung
Deep vein
thrombosis
Pulmonary
embolism
Microthrombi occlude
vessels surrounding
injection site, limiting
nutrient supply
Necrosis (tissue death)
at heparin injection site
Published Aug 29, 2014; updated Jun 16, 2025 on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications")
Volatile Gases
: Physiology & clinical findings
Volatile agent (gas) delivered to the lungs
Mean alveolar concentration of gas increases
Gas enters the bloodstream via alveolar gas exchange
Gas dissolves into lipid membranes within the central nervous system
↓ Pre-synaptic release
of excitatory
neurotransmitters (N-
methyl-D-aspartate
(NMDA), acetylcholine,
serotonin, &
glutamate)
Inhibition of post-
synaptic excitatory
neurotransmitter
receptors (NMDA,
acetylcholine,
serotonin, &
glutamate)
Distortion of
electrophysiology of
post-synaptic sodium
channels
Activation of post-
synaptic potassium
channels
↑ Presynaptic
release of
gamma-
aminobutyric
Post-synaptic cell
acid (GABA)
hyperpolarization
Impaired neuronal
depolarization
↓ Excitatory post-
synaptic input
↑ Inhibitory post-
synaptic input
Disruption of synaptic transmission in
cerebral cortex, basolateral amygdala,
hippocampus, etc.
Cerebral vasodilation & ↑ cerebral
blood flow
Authors:
Punit Bhatt
Billy Sun
Reviewers:
Priyanka Grewal
Luiza Radu
Melinda Davis*
*MD at time of publication
↓ Pre-synaptic
reuptake of
GABA
Activation
of post-
synaptic
GABA
receptors
Amnesia Loss of
consciousness
↑ Intracranial pressure
Compression of brainstem
resulting in stimulation of
the vomiting region
Nausea & Vomiting
Legend: Disruption of potassium
signaling in cerebral &
systemic vasculature
Decreased systemic
vascular resistance
Disruption of
calcium signaling in
cardiac myocytes
Induction of Anesthesia
Impaired smooth
muscle contractility
Negative
inotropic effect
Hypotension
↓ Stroke volume &
consequently decreased
cardiac output
Tachycardia
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Disruption of synaptic transmission
in medullary, respiratory, &
phrenic motor neurons
Neuromuscular
blockade
QT
Prolongation
Torsades de
Pointes
(Polymorphic
Ventricular
Tachycardia)
Respiratory
depression
Hypercapnia
(Elevated CO2
concentration
in the blood)
Muscle
relaxation
Unregulated release
of calcium in
susceptible patients
Malignant hyperthermia (a
life-threatening reaction to
certain anesthetics)**
** See malignant hyperthermia slide
Published Aug 12, 2025 on www.thecalgaryguide.com")
Obstructive Shock

↓ Right ventricle stroke volume
(blood volume ejected per beat)
↓ Blood return to left atrium
Underfilled left ventricle
Obstructive shock
↓ systemic blood flow due to a physical
obstruction of the heart’s pumping function
Insufficient
organ
perfusion
Tension pneumothorax**
↑ Pressure in the pleural cavity
Intrathoracic pressure exceeds
venous filling pressures &
compresses heart chambers
↓ Venous return to right
atrium & left atrium
Author:
Ryan Dion
Sergio F. Sharif
Dean Percy
Reviewers:
Yan Yu
Tristan Jones
Jason Waechter*
* MD at time of publication
** See corresponding
Calgary Guide slides
↓ Preload (degree of left ventricular filling)
as left ventricle receives low levels of blood
↓ Cardiac output (volume of
blood ejected from the
↓ Blood pressure (BP)
heart/min)
Baroreceptors in carotid sinus & aortic
arch detect low blood pressure
Skin
Reflexive release of catecholamines
via sympathetic nervous system
Blood supply diverted
away from peripheral
tissues to vital organs
Tachycardia
Hypotension
Cold
extremities
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Brain
↓ Cerebral blood
flow causes
cerebral hypoxia
Altered consciousness
Heart
↓ Coronary
artery
perfusion
Myocardial
ischemia**
Complications
Blood backs up into
venous system
Kidneys
↓ Blood flow
to kidneys
Prerenal acute kidney
injury **
↑ Pressure distends
veins
↑ Jugular
venous
pressure
Pressurized fluid leaks
out of veins into
tissue
Fluid enters
pulmonary
perivascular spaces
Fluid impedes normal gas
exchange in lungs
Tachypnea (↑
respiratory rate)
Dyspnea
Published July 7, 2013; updated Sept 28, 2025 on www.thecalgaryguide.com")
Sturge-Weber Syndrome
: Pathogenesis, mechanisms & clinical findings
Somatic mosaic mutations
(embryonic development
mutations producing
multiple cell lines) occur in
the GNAQ gene
Abnormal regulation
of intracellular
signaling pathways
during early
embryogenesis
Mechanism unclear. Attributed to primary defect(s) in a subset of angioblasts (precursor embryonic
cells for the endothelial cells lining blood vessels) or in other cells supporting vascular function
Authors:
Dylan Hollman*
Reviewers:
Mina Youakim
Jessica Revington
Fatemeh Jafarian*
* MD at time of publication
**See corresponding Calgary Guide slide
Localized abnormal vasculogenesis (initial creation of blood
vessels during embryonic development) & vascular function
Facial vascular malformations Intracranial vascular malformations Ocular vascular malformations
Nevus flammeus (port-wine stain birthmark)
along skin in the distribution of the trigeminal
nerve (ophthalmic/maxillary branches)
Leptomeningeal capillary-venous malformation
(abnormal blood vessel cluster in the brain/spinal covering)
Heterochromia
(different
colored eyes)
Episcleral &
conjunctival VMs
(abnormal blood
vessels on the
eye surface)
Corresponding
overgrowth of cutaneous
(skin) vasculature
Corresponding overgrowth
of underlying soft tissues
& facial bones
Impaired venous drainage ↓ normal blood
flow in the brain & ↑ overall venous
pressure, causing venous hypertension
Mechanism unclear.
Associated with disruption of
the hypothalamic-pituitary axis
Choroidal
hemangioma
(benign
blood vessel
tumor in the
choroid layer
of the eye)
Growth
hormone
deficiency
Nodularity (nodule
growths on skin)
↑ Venous pressure & ↓ venous
blood flow cause venous stasis
(blood pooling in veins)
↑ Accumulation of
coagulation factors in the
veins contributes to an ↑ risk
of thrombosis (blood clots)
↑ Venous pressure in
the episclera (outer
layer of the eye)
contributes to ↑
intraocular pressure
Hypothyroidism**
↓ Venous blood flow
impairs overall circulation
& ↓ tissue oxygenation
(chronic tissue ischemia)
Thrombi (blood clots) travel
through vasculature & can
further ↓ or block blood flow
↑ Intraocular
pressure gradually
damages the optic
nerve & contributes
to vision loss
Stroke-like events
Glaucoma
Interruption of blood flow & oxygen delivery
to the brain damages key areas of brain
tissue & ↓ clearance of waste products
Hemiparesis
(weakness on one
side of the body)
Cerebral hemiatrophy
(loss of tissue or shrinkage
of one side of the brain)
↑ Risk of focal cortical dysplasia (abnormal
organization of brain cells in specific brain locations)
↑ Risk of
brain atrophy
↑ Intraparenchymal calcification
(calcium deposits in brain tissue)
Chronic damage to brain tissue & continued impairment of key neurological functions
Visual field defects
Seizures
Intellectual disability Behavioral problems
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published October 20, 2025 on www.thecalgaryguide.com
Gingival/palatal
angiomatosis
(abnormal blood
vessel growth in
gum tissue &
palate)
Gingival
hyperplasia
(overgrowth
of gum
tissue)
Legend:
Sturge-Weber syndrome (SWS): Pathogenesis and clinical findings
Somatic mosaic mutations in the GNAQ gene
Authors:
Dylan Hollman*
Reviewers:
Mina Youakim
Fatemeh Jafarian*
* MD at time of publication
Abnormal regulation of intracellular signalling pathway in early embryogenesis
Unclear mechanism → Primary defect in subset of angioblasts or other vascular supporting cells
Facial vascular
malformations (VMs)
Localized abnormal vasculogenesis & vascular function
Ocular vascular
malformations (VMs)
Port-wine stain
(flat, red or purple birthmark caused by
dilated blood vessels) → commonly affects
trigeminal nerve (ophthalmic/maxillary)
Intracranial vascular
malformations (VMs)
Choroidal
Heterochromi
Episcleral &
hemangioma
a
conjunctival VMs
(benign tumor
(different
(abnormal blood
Leptomeningeal
of blood vessels
colored eyes)
vessels on the
capillary-venous
in the choroid
eye's surface)
Overgrowth of
Overgrowth of
malformation
layer of the eye)
underlying soft
cutaneous
(abnormal blood
tissue & bone
vasculature
vessel cluster in the
↑ episcleral
brain/spinal
(eye’s outer
Nodularity
Gingival/palatal
covering)
layer) venous
angiomatosis
pressure
(abnormal blood
Gingival
Glaucoma
vessel growth in
hyperplasia
Venous hypertension
gum tissue &
(overgrowth of gum
palate)
tissue)
Chronic tissue ischemia
Thrombosis
Hemiparesis
(weakness on one
side of body)
Venous
stasis
Unclear mechanism
→ disruption of
hypothalamic-pituitary axis
Focal cortical dysplasia
(abnormal brain tissue in
specific areas)
Intraparenchymal
calcification (calcium
deposits in brain tissue)
Stroke-like events
Hemiatrophy
(loss of tissue or
shrinkage on one
side of body) Hypothyroidism Growth hormone
deficiency
Seizures
Visual field defects
Intellectual disability Behavioral problems
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Brain
atrophy")
Fecal Incontinence

Rectal or
genital
prolapse**
Pelvic surgery
Local neuronal damage
Direct
impairment of
internal anal
sphincter
which controls
approximately
70% of anal
resting tone
Pelvic trauma
Impaired motor control
of pelvic muscles & the
external anal sphincter
Direct impairment of
external anal sphincter
↓ Resting tone in
internal anal sphincter
Voluntary external anal sphincter contraction
is no longer sufficient to close the anus
Continence (voluntary ability to control
release of stool) mechanisms are impaired
↓ Control over an essential bodily function
↑ Assistance required with
toileting & basic hygiene
Colon inflammation
(e.g., ulcerative colitis,
radiation proctitis)
↓ Stretch capacity of
rectal smooth muscle
↓ Stool storage
capacity in rectum
↑ Defecation
urgency
Internal anal sphincter
reflex relaxes
↑ Caretaker burden
↑ Perception of & exposure to
various social stigmas associated
with poor hygiene practices
↑ Feelings of shame or
significant embarrassment
↑ Stress &
anxiety
↓ Confidence &
sense of agency
↓ Engagement in social
activities or work
Complications
Sign/Symptom/Lab Finding Diarrhea-
predominant
irritable bowel
syndrome
Movement
disorders
(e.g., arthritis,
Parkinson’s)
Age-related ↓
in mobility
Sensory
neuropathy
(e.g., diabetic
neuropathy)
Conditions
altering mental
status (e.g.,
stroke, dementia)
Chronic
constipation
Chronic diarrhea
Solid & immobile
mass of stool builds
up in the rectum
Laxatives
↓ Mobility can impact
timely toileting access
& habits
Rectal hyposensitivity
(↓ perception of rectal distension)
↑ Stool volume
↑ Loose stools
Loose stool is more prone to
escape through the anal canal,
compared to solid stool
Failure to sense
rectal fullness
leads to voluntary
relaxation of the
external anal
sphincter
Loose stool can
flow around
impacted stool
mass & exit the
anal canal
(overflow
diarrhea)
Continence mechanisms are intact. Mechanisms
are subsequently overwhelmed or bypassed
Fecal Incontinence
Unintentional loss of solid or liquid stool
↑ Prolonged skin contact with an irritant (stool)
Prolonged skin exposure to digestive enzymes
(e.g., proteases, lipases) in stool
↑ Skin pH, repeated mechanical abrasion (wiping) & excessive
moisture degrade built-in protective barriers in the skin
↑ Skin inflammation
↑ Skin
erythema
(redness)
Incontinence-associated
dermatitis (degradation & loss of
protective skin layers)
↑ Pain & skin irritation
Bacteria from residual stool can
colonize eroded & damaged tissue
↑ Risk of skin infection
↓ Help-seeking
behaviours
↓ Access to &
pursuit of treatment
Published May 2, 2020; updated October 19, 2025 on www.thecalgaryguide.com")
Hypothyroidism

Iodine
deficiency
Infiltrative disease affecting
thyroid gland cells
Iatrogenic or medication-
related thyroid dysfunction
Hypothyroid phase of thyroiditis
(inflammation of the thyroid)
Pituitary gland dysfunction
(central hypothyroidism)
Progressive autoimmune
destruction of thyroid gland cells
↓ T3/T4 levels
activate the
hypothalamus-
pituitary-thyroid
axis & ↑ TSH
release by the
pituitary gland
Primary
hypothyroidism
(↑ TSH and ↓
T3/T4)
↓ T3/T4 levels
cause ↓ expression
of TH-dependent
myocardial enzymes
essential for cardiac
contractility
Cardiac myocytes
(cardiac muscle
cells) experience ↓
contractility
↓ Heart rate
↑ Bleeding
Impaired function of the thyroid gland & ↓ thyroid hormone (TH) secretion
Pituitary gland secretes ↓ levels of
thyroid stimulating hormone (TSH)
Hypothyroidism
Low or significantly ↓ secretion of triiodothyronine (T3) & thyroxine (T4) from the thyroid gland
↓ T3/T4 levels ↓
production of nitric oxide
(vasodilator) & cause
systemic vasoconstriction
of blood vessels
Systemic vaso-
constriction ↑
systemic
vascular
resistance
↑ Systemic vascular
resistance à ↑
intrarenal vascular
resistance & contributes
to ↓ renal perfusion
↓ T3/T4 levels reduce the rate of metabolic reactions in the body
including ↓ rates of carbohydrate, fat, & protein metabolism
↓ T3 levels allow fibroblasts
(connective tissue cells) to synthesize ↑
glycosaminoglycans (GAGs – structural
cell molecules capable of attracting
large amounts of water)
↓ Basal metabolic rate (base energy
required to sustain bodily functions)
↑ Diastolic blood pressure
(diastolic hypertension)
↓ Renal blood
flow à ↓
glomerular
filtration rate
(GFR)
↓ GFR
impairs renal
clearance of
excess GAGs
↑ GAG deposits
& water retention
in body tissues
↓ Energy to support physiological function
Narrowed pulse
pressure (↓
difference
between systolic
& diastolic blood
pressure)
Compensatory
mechanisms to
manage blood
volume &
circulation during
↓ T3/T4 levels
are overwhelmed
in the presence
of an infection or
systemic trauma
(e.g., heart
attack, stroke)
↓ GFR impairs
removal of excess free
water from the blood
volume by the kidneys
↑ GAG
deposits &
swelling in
skin tissue
↑ GAG deposits
in the larynx
swell & stiffen
vocal cords
↓ Skin gland
activity & ↓
sebum (oil) &
sweat
production
↑
Fatigue
↓ Motility of the
gastrointestinal
(GI) tract causes
↓ movement of
digested food &
↓ rate of waste
excretion
↓ TH levels & ↓
metabolic rate
impair neurologic
function (e.g.,
neurotransmitter
signaling & neuron
functioning)
Thickened skin
Hoarse speech
Dry skin
↑ Sodium (Na+) & water
retention in blood volume
↓ Perspiration
(sweating)
Constipation
Neurologic
symptoms (e.g.
depression,
somnolence)
Abnormally heavy menses
Excessive water retention
dilutes serum Na+ levels in
severe hypothyroidism
↓ Caloric expenditure at rest & with activity
↑ Risk of infertility
Myxedema coma**
(extreme manifestation
of hypothyroidism)
Hyponatremia
(↓ Na+)
↑ Fluid
retention in
body tissues
Weight gain
Musculoskeletal
symptoms (e.g.,
muscle cramps,
joint pain & ↓
muscle tone)
Published June 19, 2013, revised November 23, 2025 on www.thecalgaryguide.com
Normal or ↓
TSH levels
when T3/T4
levels are low
Authors:
Sophia Khan, Ayden Hansen, Jessica
Revington, Rupali Manek, Jaye
Platnich
Reviewers:
Shahab Marzoughi, Gurreet
Bhandal, Raafi Ali, Matthew
Harding, Mark Elliott, Hanan
Bassyouni*, Breanna McSweeney*
* MD at time of publication
**See corresponding Calgary Guide
slides
↓ T3 levels lead to
↓ lipoprotein lipase
(lipid metabolism
enzyme) activity
↑ Triglyceride
levels in blood
↓ TH levels & ↓
metabolic rate
impair cold
tolerance &
thermogenesis
(heat production)
mechanisms
Cold
extremities
(e.g. hands,
feet)
↓ Cold
tolerance
↓ Activation
of the T3-
mediated low-
density
lipoprotein
(LDL) receptor
gene
↓ LDL
receptor
expression
for LDL
clearance
↑ LDL
cholesterol
levels in
the blood
↓ T3/T4 levels ↓
coagulation factor
synthesis by the liver
↓ T3/T4 levels disrupt
the menstrual cycle &
cause anovulation
(absence of ovulation)
Legend: Hyperlipidemia
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications")
Heart Transplant Indications and Benefits

Used as bridge to transplant
Failure of treatment with
conventional heart failure
therapies
Cardiac transplant recommended
Major systemic diseases,
including cancer
Assess surgical readiness and
comorbidities with evaluation by
cardiac surgeon & cardiologist
Psychological Instability
Active or recent
substance abuse
Bridge to transplant with
inotropes or mechanical
circulatory support devices
(VAD, ECMO, IABP)
Cardiac Transplant
Surgery to replace dysfunctional
heart with a functional donor heart
**See corresponding Calgary Guide slide(s)
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Heart Transplant: Indications & Benefits Indications
Kate Fougere
Authors:
Reviewers:
Emily Kuervers
Sergio F. Sharif
Dr. Robert Miller*
Severe cardiomyopathy
Myocardial dysfunction
* MD at time of publication
Disease of the cardiac
Pump Failure
↓ Stroke volume (SV),
muscle (Dilated,
↓ Forward flow,
↓ cardiac output (CO),
hypertrophic, restrictive
backup into lungs
↓ blood pressure (BP)
cardiomyopathies**)
Acyanotic heart
disease
Normal concentration
of oxygenated Hb
↓ Perfusion
of organs with
↑ pulmonary
congestion
Congenital Heart Disease**
Disruption of normal cardiac
formation that is
unsuccessfully treated with
surgical repair
Cyanotic heart disease
↑ Concentration of
deoxygenated
hemoglobin (Hb)
Cyanosis
(dusky, blue
skin
discoloration)
Cardiac Allograph
Vasculopathy (CAV)
Diffuse concentric narrowing
of coronary arteries
Antibody mediated graft rejection &
fibrosis
Symptoms of
heart failure **
Cardiovascular risk factors exacerbated
by immunosuppressive drugs
↓ BP
Reduced SV with
no response to
medical therapy
Pump Failure
↓ Forward flow,
backup into lungs
↓ Perfusion of organs
↓ Level of consciousness
End organ damage
Abnormal electrical activity does not respond to
pharmacological agents, cardiac ablation or
electrophysiological interventions (ICD)
Refractory arrythmias (ventricular
tachycardia, ventricular fibrillation) &
subsequent cardiac death
Device complications arise
while awaiting
transplantation
Device infection
Clotting or bleeding complications
(stroke or hemorrhage)
Abbreviations:
• ICD - Implantable cardioverter defibrillators
• ECMO- Extracorporeal membrane oxygenation
• IABP - Intra-aortic balloon pump
Low survival benefit from transplant
↓ Capacity to manage post transplant
requirements
Graft rejection
↑ Potential for relapse after transplant
↓ Symptoms of heart failure**
Restoration of cardiac output &
normalization of volume status
↑ Life expectancy
↑ Quality of life
Published Nov 23, 2025 on www.thecalgaryguide.com")
Ventricular Septal Defect
: Pathogenesis and clinical findings
Variants in genes involved in
cardiac development (e.g., GATA4)
DiGeorge syndrome**
(deletion on chromosome 22q11)
Holt-Oram syndrome
(TBX5 mutations)
Down syndrome** (Trisomy
21) (more commonly AVSD)
CHARGE
syndrome
Infection
Medication (e.g.,
isoretinoin)
Uncontrolled metabolic
conditions (e.g., diabetes**)
Environmental
exposures (e.g.,
alcohol)
Genetic factors that
↑ susceptibility
Complex interplay between genetic
susceptibility & environmental factors
Maternal factors during
pregnancy that ↑ risk
Disruption in formation of interventricular septum during fetal heart development
Ventricular Septal Defect (VSD)
Defect in interventricular septum that allows blood to shunt from the left ventricle (LV) to the right ventricle (RV)
LV pumps against high systemic vascular resistance (SVR) & RV pumps against lower pulmonary vascular resistance (↓ after birth)
Blood flows through VSD from LV to RV during systole (left-to-right shunt)
Small defect (<4 mm)
between ventricles
Moderate (4-6 mm) to large defect
(>6 mm) between ventricles
Narrow (restrictive) defect
between ventricles provides
intrinsic resistance to flow
Wide (unrestrictive) defect between ventricles offers little resistance to blood flow
↑ Volume of blood in pulmonary circulation
↑ Turbulent blood flow
through small defect
↓ Turbulent blood
through large defect
Pulmonary arterial hypertension (PAH)**
↑ Pulmonary venous return to left heart
Grade 3 to 5/6 harsh
holosystolic murmur
Grade 1 to 2/6, mid-frequency,
holosystolic murmur
Loud pulmonic S2
on auscultation
↑ Pulmonary vascular
markings on x-ray
LV undergoes eccentric hypertrophy
to accommodate chronic ↑ volume
↑ Left atrial
pressure
Dilation of
tricuspid annulus
LV dilation & myocardial stretch
impairs contractile function
Lateral displacement of
cardiac apex on x-ray
Mitral regurgitation
Impaired ejection (systolic
dysfunction) results in ↓ stroke
volume & ejection fraction
↑ LV end-diastolic
pressure
↑ Pulmonary
venous pressure
Mid-diastolic
murmur
↓ Cardiac output (CO) Left heart failure**
Pulmonary edema (fluid
accumulation in pulmonary
interstitium & alveoli)
Sympathetic nervous
system is activated
Systemic venous
congestion
Renin-angiotensin aldosterone
system** is activated
↑ Work of breathing
Diaphoresis
Pallor ↑ Heart
(excessive
rate
sweating)
Peripheral
edema
Hepatomegaly
Na+ & fluid
retention
Shortness
of breath
↑ Respiratory
rate
**See corresponding Calgary Guide slide
Complications
Published Oct 17, 2015; updated Dec 7, 2025 on www.thecalgaryguide.com
Prolonged PAH drives reactive constriction &
permanent remodeling of pulmonary vessels
Chronic ↑ RV afterload
Irreversible PAH
RV hypertrophy & dilation
to overcome ↑ afterload
Dilation ↑ RV wall stress
↑ RV stretch impairs
ability to eject blood
↑ RV end-diastolic pressure
RV pressure > LV pressure
Right heart
failure**
Eisenmenger syndrome** (shunt
reversal, right-to-left shunt)
Pathophysiology Mechanism
Sign/Symptom/Lab Finding")
Necrosis versus Apoptosis

Hypoxia
(↓ Oxygen
delivered to tissues)
Physical agents
(extreme temperatures,
trauma, radiation)
Bacterial, viral, or
fungal infections
&/or microbe toxins
Necrosis
Uncontrolled & pathologic cell death
Harmful stimuli trigger ↓ ATP (cellular energy)
↓ ATP leads to ion pump failure & ↑ cell permeability (“leakiness”)
↑ Cellular ion influx causes cell to swell & lyse (rupture its plasma membrane)
Intracellular contents spill into the extracellular space
Intracellular contents activate inflammasomes (cytoplasmic multiprotein complexes)
Pro-inflammatory cytokine interleukin-1β is secreted & activates the immune system
Excessive cytokine release provokes a large inflammatory response
Inflammation damages surrounding healthy tissues & organs
Ischemia (↓ Blood
flow) to organs
except brain
↓ Oxygen denatures
enzymes à dead cell
skeletons cannot breakdown
Cells remain
“coagulated”
(firm) for days
Coagulative
necrosis
↓ Blood flow to limb(s)
+/- bacterial invasion
Gangrenous
necrosis
↑ Pain or ↓ feeling in affected limb(s)
Skin color changes (red, purple, black)
Damaged adipocytes (fat cells) release
triglyceride (fat) contents that group into oil cysts
Scars form &
calcify (harden)
Fat necrosis
Damaged endothelium (blood
vessel wall) becomes leaky
Fibrin (blood protein) deposits in
endothelium with immune complexes
Fibrinoid
necrosis
Brain ischemia &/or
infection kills cells
Digestive enzymes transform dead
tissue into creamy liquid pus
Liquefactive necrosis
Coagulative + liquefactive necrosis mechanisms à granular debris
Caseous necrosis
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
-----------------------------------------------------------------------------------------------------
Authors:
Tyra Fernandes
Catherine R Jarvis
Reviewers:
Mitchell Chorney
Sarah Smith*
* MD at time of publication
Apoptosis
Programmed cell death via an energy-dependent process
Extrinsic pathway: cellular stress or
damage signals in the extracellular
environment trigger apoptosis
Intrinsic pathway: internal
cellular stressors (damage from
chemotherapy, UV radiation,
drugs) trigger apoptosis
Ligands such as TNF-α (tumor
necrosis factor-alpha, produced by
macrophages) & FasL (Fas ligand,
produced by T cells) bind to apoptotic
receptors on the cell’s surface
Pro-apoptotic factors recognize
cellular stressors
Cytochrome C releases from the
intermembrane space of the
mitochondria to the cytoplasm
Ligand binding activates initiator
caspases (protease (protein
breakdown)-like enzymes) 2, 8, 9, 10
Cytochrome C activates Caspase-9
Initiator caspases activate
effector caspases 3, 6, 7
Caspase-9 activates
effector caspases 3 & 7
Effector caspases begin execution pathway
Caspases degrade the cell’s nuclear envelope & DNA
à DNA repair is inhibited & cell shrinks
Cellular shrinkage forms apoptotic bodies
Phagocytes engulf apoptotic bodies to prevent inflammation
Ineffective phagocytosis à inflammation
Published Feb 8, 2026 on www.thecalgaryguide.com
Final Slide is 1st
Necrosis vs Apoptosis: Pathogenesis and clinical findings
Toxic chemicals
(poisons, drug
toxicities)
Hypoxia
(↓ Oxygen
delivered to tissues)
Physical agents
(extreme temperatures,
trauma, radiation)
Toxin release
from bacteria,
viruses, or fungi
Necrosis
Uncontrolled & pathologic cell death
Harmful stimuli trigger ↓ ATP (cellular energy)
↓ ATP leads to ion pump failure & ↑ cell permeability
↑ Cellular ion influx causes cell to swell & lyse (rupture its plasma membrane)
Intracellular contents spill into the extracellular space
Intracellular contents activate inflammasomes (cytoplasmic multiprotein complexes)
Pro-inflammatory cytokine interleukin-1β is secreted and activates the immune system
Excessive cytokine release provokes a large inflammatory response
Inflammation damages surrounding healthy tissues & organs
Ischemia (↓ Blood
flow) to organs
except brain
↓ Oxygen denatures
enzymes à cell skeleton
cannot be broken down
Cell is preserved
in “coagulated”
state for days
Coagulative
necrosis
↓ Blood flow to limbs
+/- bacterial invasion
Gangrenous
necrosis
↑ Pain or ↓ feeling in limb
Skin color changes (red, purple, black)
Damaged adipocytes (fat cells) release
triglycerides (fat) contents that group into oil cysts
Scars form &
calcify (harden)
Fat necrosis
Damaged endothelium (blood
vessel wall) becomes leaky
Fibrin (blood protein) deposits in
endothelium with immune complexes
Fibrinoid
necrosis
Brain ischemia &/or
infection kills cells
Digestive enzymes transform dead
tissue into creamy liquid pus
Liquefactive necrosis
Coagulative & liquefactive necrosis mixture à granular debris
Caseous necrosis
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding -----------------------------------------------------------------------------------------------------
Complications
Authors:
Tyra Fernandes
Catherine R Jarvis
Reviewers:
Mitchell Chorney
Sarah Smith*
* MD at time of publication
Apoptosis
Programmed cell death via an energy-dependent process
Extrinsic pathway: cellular stress or
damage signals in the extracellular
environment trigger apoptosis
Intrinsic pathway: internal
cellular stressors (chemotherapy,
UV radiation, drugs, misfolded
proteins) trigger apoptosis
Ligands such as TNF-α (tumor
necrosis factor-alpha, produced by
macrophages) & FasL (Fas ligand,
produced by T cells) bind to apoptotic
receptors on the cell’s surface
Pro-apoptotic factors recognize
cellular stressors
Cytochrome C releases from the
intermembrane space of the
mitochondria to the cytoplasm
Ligand binding activates initiator
caspases (protease (protein
breakdown)-like enzymes) 2, 8, 9, 10
Cytochrome C activates Caspase-9
Initiator caspases activate
effector caspases 3, 6, 7
Caspase-9 activates
effector caspases 3 & 7
Effector caspases begin execution pathway
Caspases degrade the cell’s nuclear envelope & DNA
à DNA repair is inhibited & cell shrinks
Cellular shrinkage forms apoptotic bodies
Phagocytes engulf apoptotic bodies to prevent inflammation
Ineffective phagocytosis à inflammation
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Necrosis vs Apoptosis
Toxic chemicals
(poisons, drug
toxicities)
Hypoxia
(↓ Oxygen
delivered to tissues)
Physical agents
(extreme temperatures,
trauma, radiation)
Biological agents
(bacteria,
viruses, fungi)
Necrosis
Non-physiologic & uncontrolled cell death
Noxious (harmful) stimuli trigger increased cell permeability and ion pump failure
Cell swells & ruptures its plasma membrane à cell lysis (breakdown)
Intracellular contents spill into the extracellular space
Intracellular contents activate inflammasomes (cytoplasmic multiprotein complexes)
Pro-inflammatory cytokine interleukin-1β is secreted and activates the immune system
Excessive cytokine release provokes a large inflammatory response
Inflammation damages surrounding healthy tissues & organs
Acute tubular
necrosis
(damaged kidney
tubule cells)
Gangrene
(body tissue death)
Myocardial infarction
(heart attack)
Steatohepatitis
(progressive
liver disease)
↓ Blood flow to a
Myocardium (heart
portion of the body
muscle) is deprived
Necrotic renal
(usually limbs)
of oxygen &
(kidney) tubular
becomes damaged
epithelial cells
deteriorate &
slough off
↑ Extracellular
matrix proteins
(especially
collagen) are
produced and
deposit in liver
Granular casts
on urine
microscopy
↑ Pain
or
↓ Feeling
Skin
color
change
(red,
purple,
black)
↑ Blood
troponin
levels
↓ Heart
function
Liver fibrosis
(scarring)
Legend: Authors:
Tyra Fernandes
Catherine R Jarvis
Reviewers:
-----------------------------------------------------------------------------------------------------
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Mitchell Chorney
Name Name*
* MD at time of publication
Apoptosis
Programmed cell death via an energy-dependent process
Extrinsic Pathway: Apoptotic signals
from other cells cause initiation
Intrinsic Pathway: Internal cellular
stressors (chemotherapy, UV
radiation, drugs, misfolded
proteins) cause initiation
Ligands such as TNF-α (tumor necrosis
factor-alpha, produced by
macrophages) & FasL (Fas ligand,
produced by T cells) bind to apoptotic
receptors on the cell’s surface
Pro-apoptotic factors recognize
cellular stressors
Cytochrome P releases from the
intermembrane space of the
Ligand binding activates initiator
mitochondria to the cytoplasm
caspases (protease (protein
breakdown)-like enzymes) 2, 8, 9, 10
Cytochrome P activates Caspase-9
Initiator caspases activate
effector caspases 3, 6, 7
Caspase-9 activates caspases
3 & 7
Execution Pathway
Caspases degrade the cell’s nuclear envelope & DNA
à DNA repair is inhibited & cell shrinks
Cellular shrinkage forms apoptotic bodies
Phagocytes engulf apoptotic bodies to prevent inflammation
Ineffective phagocytosis à inflammation
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Necrosis vs Apoptosis
Hypoxia
Chemical agents
Physical agents Biological agents
Necrosis
Non-physiologic & uncontrolled
cell death
Oncolysis (ion pump failure and
increased cell permeability
cause cell swelling) occurs due
to noxious stimuli
Plasma membrane ruptures and
cell is lysed (broken down)
Intracellular contents spill into
the extracellular space
Authors:
Tyra Fernandes
Reviewers:
Mitchell Chorney
Catherine R Jarvis
Name Name*
* MD at time of publication
Renal tubule is damaged due to
reduced oxygen supply and toxicity
Granular casts on urine microscopy
Acute tubular necrosis (kidney
disorder of the tubule cells
Extracellular matrix proteins accumulate
in liver causing collagen deposition
Liver fibrosis
Steatohepatitis
(progressive liver disease)
Intracellular contents activate
inflammasomes (cytoplasmic
multiprotein complexes)
Myocardium (heart muscle) is
deprived of oxygen
↑ Blood troponin levels
Myocardial infarction
-----------------------------------------------------------------------------------------------------
Apoptosis
Programmed cell death via an
energy-dependent process
Extrinsic Pathway: Apoptotic signals
from other cells cause initiation
Ligands such as TNF-α (tumor necrosis
factor-alpha, produced by
macrophages) and FasL (Fas ligand,
produced by T cells) bind to apoptotic
receptors on the cell’s surface
Ligand binding activates initiator
caspases (protease-like
enzymes) 2, 8, 9, 10
Initiator caspases activate
effector caspases 3, 6, 7
Intrinsic Pathway: Internal cellular
stressors (chemotherapy, UV
radiation, drugs, & misfolded
proteins) cause initiation
Pro-apoptotic factors recognize
cellular stressors
Cytochrome P releases from the
intermembrane space of the
mitochondria to the cytoplasm
Cytochrome P activates Caspase-9
Caspase-9 activates caspases
3 & 7
Pro-inflammatory cytokine
interleukin-1β is secreted and
activates the immune system
Excessive cytokine release
provokes a large inflammatory
response
Legend: Inflammatory
damage to the
surrounding
healthy tissues
Microscopic
Effects:
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Execution Pathway
Caspases degrade the cell’s nuclear envelope. DNA
fragments inhibit DNA repair, which shrinks the cell
Cellular shrinkage forms apoptotic bodies
Phagocytes engulf apoptotic bodies to prevent inflammation
Ineffective phagocytosis à inflammation
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Necrosis vs Apoptosis
Authors:
Tyra Fernandes
Reviewers:
Mitchell Chorney
Catherine R Jarvis
Hypoxia, physical agents,
chemical agents, biologic agents
Necrosis (Non-physiologic
& uncontrolled cell death)
Oncolysis (cell swelling due to
the failure of ion pumps and
increased cell permeability)
occurs due to noxious stimuli
Plasma membranes rupture
leading to cell lysis
Intracellular contents spill into
the extracellular space
Inflammasomes (cytoplasmic
multiprotein complexes) are
activated
Pro-inflammatory cytokine
interleukin-1β is secreted and
activates the immune system
Excessive cytokine release
provokes a large inflammatory
response
Legend: Microscopic Effects:
Steatohepatitis
Collagen deposition due
to the accumulation of
extracellular matrix
proteins
Liver fibrosis
Myocardial
Infarction
Ischemic or toxic
injury to the renal
tubule
Granular casts on
urine microscopy
Acute tubular
necrosis
Oxygen supply
deprivation to the
myocardium
Elevated blood
troponin levels
-----------------------------------------------------------------------------------------------------
Extrinsic Pathway: Apoptotic Signals
from other cells cause initiation
Ligands such as TNF-α (tumor necrosis
factor-alpha, produced by
macrophages) and FasL (Fas ligand,
produced by T cells) bind to apoptotic
receptors on the cell’s surface
Ligand binding activates initiator
caspases (protease-like
enzymes) 2, 8, 9, 10
Initiator caspases activate
effector caspases 3, 6, 7
Apoptosis (Programmed
cell death via an energy-
dependent process)
Name Name*
* MD at time of publication
Intrinsic Pathway: Internal cellular
stressors chemotherapy, UV
radiation, drugs, & misfolded
proteins) cause initiation
Pro-apoptotic factors recognize
cellular stressors
Cytochrome P releases from the
intermembrane space of the
mitochondria to the cytoplasm
Cytochrome P activates Caspase-9
Caspase-9 activates caspases 3 and
7
Execution Pathway
Cellular shrinkage
forms apoptotic
bodies
Inflammatory damage to
surrounding healthy tissues à
potential organ failure
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
The nuclear envelope
degrades and DNA
fragments which
inhibits DNA repair
which shrinks the cell
Phagocytes engulf
apoptotic bodies to
prevent inflammation
Ineffective phagocytosis
à inflammation
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Authors:
Necrosis vs Apoptosis
Tyra Fernandes
Reviewers:
Mitchell Chorney
Necrosis Apoptosis
Catherine R Jarvis
Hypoxia: ischemia, respiratory
insufficiency
Physical agents: trauma, radiation,
Non-physiologic &
temperature, electrical shock
uncontrolled cell death
Biological agents: bacteria, viruses, fungi
Chemical agents: poisons, drugs,
Cell swelling (oncosis) due to
occupational exposures
the failure of ion pumps and
increased cell permeability
Collagen deposition leading
to liver fibrosis
Cell lysis due to the rupture of
the plasma membrane
Steatohepatitis
Microscopic
Spillage of intracellular contents
Effects:
into the extracellular space
Acute tubular
Myocardial
Activation of cytoplasmic
necrosis
Infarction
multiprotein complexes, known
as inflammasomes
Ischemic or toxic
Oxygen supply
injury to the renal
deprivation to the
tubule
myocardium
Secretion of pro-inflammatory
cytokine interleukin-1β, which
-----------------------------------------------------------------------------------------------------
Name Name*
* MD at time of publication
Programmed cell death via
an energy-dependent
process
Extrinsic pathway Intrinsic pathway
The cell receives apoptotic signals
Initiated by internal cellular
from other cells
stressors such as chemotherapy
drugs, UV radiation, and misfolded
Apoptosis is activated via ligands
proteins
binding to apoptotic receptors on
the cell surface
Pro-apoptotic factors recognize
cellular stressors
Ligand binding activates initiator
caspases (2, 8, 9, 10), which are
Cytochrome P releases from the
protease-like enzymes
intermembrane space of the
mitochondria to the cytoplasm
Examples of ligands include: TNF-α
(produced by macrophages) and
Caspase-9 is activated
FasL (produced by T cells)
Activation of downstream effector
Effector caspases (3, 6, 7) are
caspases 3 and 7
activated
activates the immune system
Excessive cytokine release
provokes a large inflammatory
response
Legend: Granular casts on
urine microscopy
Elevated blood
troponin levels
Damage to surrounding
healthy tissues may lead to
organ failure
Prevention of
inflammation
Execution pathway
The nuclear envelope
degrades and DNA fragments
which inhibits DNA repair
Cellular shrinkage
forms apoptotic
bodies
Phagocy
engulfment of
apoptotic bodies
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Necrosis versus apoptosis
Necrosis
Non-physiologic &
uncontrolled cell death due
to noxious stimuli
Cell swelling (oncosis) à cell
lysisà spillage of
intracellular contents à
tissue damage
Inflammatory response,
leading to inflammasome
activation and the secretion of
pro-inflammatory cytokine
interleukin-1β
Macroscopic
Effects:
Hypoxia: ischemia, respiratory insufficency
Physical agents: trauma, radiation,
temperature, electrical shock
Biological agents: bacteria, viruses, fungi
Chemical agents: poisons, drugs,
occupational exposures
Acute tubular
necrosis due to
chemical agents
Myocardial
infarction due to
hypoxia
Microscopic
Effects:
Stroke due to
hypoxia in the brain
Gangrene due to
hypoxia of the limbs
Steatohepatitis due
to chemical agents
-----------------------------------------------------------------------------------------------------
Apoptosis
Programmed cell death via
an energy-dependent
process
Execution phase: pro-& anti-
apoptotic proteins mediate
cell breakdown by caspases
Caspase activity blocks DNA
repair à leading to
fragmented DNA and cell
shrinkage
Apoptosis is
inhibited in cancer
the overexpression
of anti-apoptotic
proteins
Authors:
Tyra Fernandes
Reviewers:
Mitchell Chorney
Name Name*
* MD at time of publication
Extrinsic pathway: immune cell activation
activates executioner caspases; ligands such
as TNF-α & FasL bind to receptors on the cell
membrane
Intrinsic pathway: internal cellular factors
cause pro-apoptotic factors to increase
mitochondrial membrane permeability.
Cytochrome c is released from the inner
mitochondrial membrane, which ultimately
activates caspases
Cellular fragments are
engulfed by immune cells
which prevents an
inflammatory response
Organism death via
necrosis
Menstruation Embryogenesis
Endometrial
shedding of the
inner lining of
the uterus is an
apoptotic
mechanism
The tissue
between the
fingers and toes
degrades via
apoptosis in
utero à
separation of
the digits
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Abbreviations:
• IL-1β– interleukin-1β
• TNF-α– tumour necrosis factor - alpha
• FasL– CD95 ligand; mediates apoptosis
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Complications
References
• https://next.amboss.com/us/article/VP0GdT?q=apoptosis#Y0d79977cce8fc2c548ac720f8060d667
• https://www.ncbi.nlm.nih.gov/books/NBK557627/
• https://www.ncbi.nlm.nih.gov/books/NBK499821/
• https://pmc.ncbi.nlm.nih.gov/articles/PMC5855670/
• https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/oncosis
• https://www.nature.com/articles/s41421-020-0167-x
• https://pmc.ncbi.nlm.nih.gov/articles/PMC3714593/
• https://www.ncbi.nlm.nih.gov/books/NBK537076/
Hypoxia
Physical agents
Biological agents
Chemical agents")
Cryoglobulinemia

(↑ Lymphocyte
(blood) cancers
infection (HCV)
attacking) conditions
cerebral
Cerebral
threshold
production) conditions
(brain)
vasculitis Ischemic stroke (clot blocks
Inflamed vasculature
arteries
↓ cerebral blood flow
cerebral blood flow)
Acute ↑ B cell activity ↑
Chronic B cell activation ↑
Deposits in
Retinal
Retinal artery hemorrhage (severe bleeding)
immunoglobulin (Ig) production
immunoglobulin (Ig) production
retinal arteries
vasculitis Retinal artery infarct (↓ oxygenation à tissue death)
of eyes
Tingling
Type II:
Type III:
Deposits damage & narrow walls of
↓ Blood flow
monoclonal (recognize 1
polyclonal
tiny blood vessels supplying
to nerve cells Numbness
Type I:
site on antigen) IgM, IgG or
(recognize >1
nutrients to peripheral nerves
Weakness
monoclonal (recognize 1
IgA & polyclonal (recognize
site on antigen)
site on antigen) IgM or IgG
>1 site on antigen) Igs
IgG & IgM
Deposits in
Alveolar
alveolar (lung air
capillaries are
sacs) capillaries
destroyed
Exposure to temperatures <37°C
Immune complexes deposit & form cryoglobulin
(abnormal protein) in small/medium-sized vessels
Cryoglobulins activate complement (factors that
enhance innate (first-line) immune system responses)
Deposits in
cardiac (heart)
tissue
Deposits obstruct
mesenteric (abdominal)
vasculature
Myocardial (heart muscle)
inflammation, necrosis &
fibrosis (scarring)
Mesenteric
vasculitis
Alveolar
Dyspnea (short of breath)
hemorrhage
(severe bleeding) Hemoptysis (coughing blood)
Hypoxia (↓ Tissue oxygenation)
Myocarditis (inflamed myocardium)**
Inflamed vasculature
Gastrointestinal
à ↑ rupture risk
bleed
Mesenteric ischemia (↓
↓ Mesenteric
blood flow
oxygen to intestines) à
scars & narrows intestines
Complement factors are
consumed (activated &
used)
Immune complexes
(primarily type I)
occlude vessels
Immune complexes (primarily
types II & III) deposit in vessels à
endothelial (vessel wall) damage &
vasculitis (inflammation)
Abdominal pain
Abdominal cramps
Bowel obstruction
Deposits damage glomeruli
(kidney capillary clusters) à
triggers inflammation
↑ Permeability
(“leakiness”) in
damaged capillaries
Hematuria (blood in urine)
Proteinuria (protein in urine)
↓ Complement
factors C3 & C4
Blood in obstructed
vessel areas becomes
hyper-viscous (thick)
Hyperviscosity
syndrome
Inflammation ↑ proliferation
of glomerular basement
Blood stasis &
vascular congestion
↓ Oxygen
delivered to skin
Local hypoxia (↓
oxygen delivery)
Visual disturbances
Confusion
Headache
Membranoproliferative glomerulonephritis
(immune-mediated kidney inflammation)
Joint swelling
Joint stiffness
↑ Hydrostatic
pressure ruptures
capillaries
Livedo reticularis
(reddish-blue patchy
skin discolouration)
Reactive
vasoconstriction
(narrowed vessels)
Deposits in synovial (joint
connective tissue) membrane Deposits
damage post-
capillary
venules in
dermis (skin)
Red blood
cells leak
into
surrounding
tissue
Mucosal (moist lining of
Raynaud phenomena (extremities
exposed tissues) bleeding
become white & numb
Vasoconstriction
obstructs blood vessels
Ischemia (restricted
blood supply to tissues)
Synovial edema (swelling) & thickening
Non-blanchable
(non-color-
fading) purpura
(palpable purple
skin spots)
Necrosis (cell &
tissue death)**
Authors:
Julia Fox, Catherine R Jarvis
Reviewers:
Navdeep Goraya, Glen Hazlewood*
* MD at time of publication
**See corresponding Calgary Guide slide(s)
Legend: Pathophysiology Mechanism
Complications
Published Mar 1, 2026 on www.thecalgaryguide.com
↓ Blood
flow
Sign/Symptom/Lab Finding")
Restrictive Cardiomyopathy
: Pathogenesis and clinical findings Amyloidosis
(abnormal deposition of
amyloid protein in organs)
Sarcoidosis**
(granulomas form
within organs)
Hemochromatosis**
(genetic mutation leading
to ↑ iron absorption)
Amyloid protein deposits
between myocardial cells
Granulomatous inflammation
infiltrates the myocardium
Iron deposits as
haemosiderin in the heart
Infiltration of myocardium by
pathological proteins or fibrosis
Scarring & fibrosis of
the conduction system
↑ Myocardial stiffness reduces
ventricular wall compliance
Impaired passive ventricular filling
during diastole
↓ Stroke volume (SV)
Blood accumulating in a stiffer
ventricle ↑ left ventricular diastolic
pressure above normal
↓ Cardiac output
(CO = SV X HR )
Low tissue perfusion
↓ oxygen delivery
↑ Stimulus
to breathe
Fatigue
Tachypnea
(abnormally
rapid breathing)
↑ Jugular
venous pressure
Endomyocardial fibrosis
(idiopathic fibrotic thickening
of endocardium & myocardium
found in tropical regions)
Authors:
Tristan Jones
Alexander Arnold
Alexandre Bedard
Reviewers:
Sean Spence
Nicholas Samuelson
Yan Yu*
Sarah Weeks*
* MD at time of publication
** See corresponding Calgary
Guide slide(s)
Arrhythmia
(abnormal heartbeat)
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding ↑ Reliance on atrial
contraction for
ventricular filling
Strong atrial contraction forces
blood into stiff ventricle,
audible via stethoscope
S4 heart
sound
↑ Pressure propagates
backwards to left atrium &
pulmonary veins
↑ Pulmonary capillary
pressure causes fluid
accumulation in lungs
Dyspnea
(shortness of
breath)
↑ Pressure propagates backward to right heart
Pleural
Effusion
↑ Systemic venous pressure
Backed up blood accumulates
in the internal jugular veins
↑ Venous hydrostatic
pressure causes flow of
fluid out of capillaries &
into interstitium
Backed up blood
accumulates in
the liver & spleen
(see Calgary Guide slide on
“JVP: Kussmaul’s Sign
explained” for full mechanism)
Kussmaul’s sign
(paradoxical ↑ in JVP
on inspiration)
Peripheral
Edema
(excess fluid in
extremities)
Ascites
(excess fluid
in abdomen)
Hepatosplenomegaly
(enlarged liver &
spleen)
Published Feb 21, 2014; updated May 5, 2026 on www.thecalgaryguide.com
Complications")
Takotsubo Cardiomyopathy

Acute emotional
distress (primary cause:
~90% of incidence)
Critical disease
decompensation
Neurogenic events (e.g.,
ischemic stroke,
subarachnoid hemorrhage)
Surgical or
procedural
stress
Brain-heart
axis causing
abnormalities
Other (no
identifiable cause)
Acute stressors activate sympathetic nervous system
Author:
Tony Gu
Ryan Rahimi
Reviewers:
Luke Gagnon
Emily Ryznar
Catherine R Jarvis
Jason Waechter*
Mannat Dhillon*
*MD at time of publication
**See corresponding
Calgary Guide slide(s)
↑ Catecholamine release (epinephrine & norepinephrine)
Apex of the heart has
the highest")
Hypertrophic Cardiomyopathy
: Pathogenesis and clinical findings Autosomal dominant mutations in
genes encoding cardiac sarcomere
proteins (e.g., troponin, myosin)
Dysfunctional sarcomeres contract
inefficiently causing myocardial
hypertrophy (abnormal & excessive
growth of heart muscle)
Hypertrophic Cardiomyopathy (HCM)
(a genetic condition characterized by
thickening, stiffening & disarray of left
ventricular myocardium)
Unknown or
undefined
genetic causes
Septal myocardial thickening
(narrows the left ventricular
outflow tract
In early systole, the left ventricle
ejects blood normally into the aorta
As systole progresses, blood flows
faster through the narrowed
outflow tract causing turbulent flow
Faster blood flow ↓ pressure
(Venturi effect) & “pulls” the
mitral valve into the outflow tract
The mitral valve partially
obstructs blood flow to the aorta
In late systole, the ventricle starts
to relax → ↓ contractility &
pressure → ↓ mitral valve systolic
anterior motion (SAM) → forward
aortic blood flow is restored
“Bifid” pulse (double-tap due to
normal blood flow, transient
obstruction, then ↑ blood flow)
felt on palpation
Legend: Hypertrophic Obstructive
Cardiomyopathy (HOCM)
(a subtype of HCM in
which a thickened
interventricular septum
dynamically obstructs
blood flow leaving the
left ventricle)
Cardiac stiffening limits left-ventricular
expansion during diastole & impairs filling
of the heart in most patients
Systolic murmur
heard with
stethoscope
The displaced mitral
valve does not close
properly, allowing
blood to leak
backward into the
left atrium
Mitral
regurgitation
(mitral valve is
leaky)
Disorganized
myocytes (heart cells)
disrupt signal
conduction
Ventricular
arrhythmias
↓ Left ventricular expansion
↑ left heart pressure causing
pressure to back up into
pulmonary veins
↓ Stroke volume
(volume of blood
pumped per heartbeat)
Irregular
myocardial
contraction
significantly ↓
cardiac output
↑ Hydrostatic forces in
pulmonary capillaries
cause fluid movement into
interstitial tissue & alveoli
↓ Cardiac output (volume
of blood pumped by the
heart per minute)
Sudden
cardiac death
Fluid-filled alveoli
have ↑ resistance,
requiring greater
air pressure to
inflate the lungs
Dyspnea
(shortness of
breath)
Tristan Jones
Authors:
Alexander Arnold
Ryan Dion
Nicholas Samuelson
Reviewers:
Sean Spence
Yan Yu
Sarah Weeks*
* MD at time of publication
Audible sound as
atrium “kicks” blood
into stiff ventricle (if
in sinus rhythm)
S4 heart sound
heard with
stethoscope
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Diffuse crackles
heard over the
lungs with
stethoscope
Pulmonary
edema
(fluid in
lungs)
Hypertrophic myocytes
↑ oxygen demand
while myocardial
oxygen supply falls
Anginal
chest pain
Re-Published May 26, 2026 on www.thecalgaryguide.com
↓ Oxygen delivery
to peripheral tissues
(e.g., muscles)
Exercise
intolerance")