SEARCH RESULTS FOR: renal
Nephrotic Syndrome: Pathogenesis and Clinical Findings
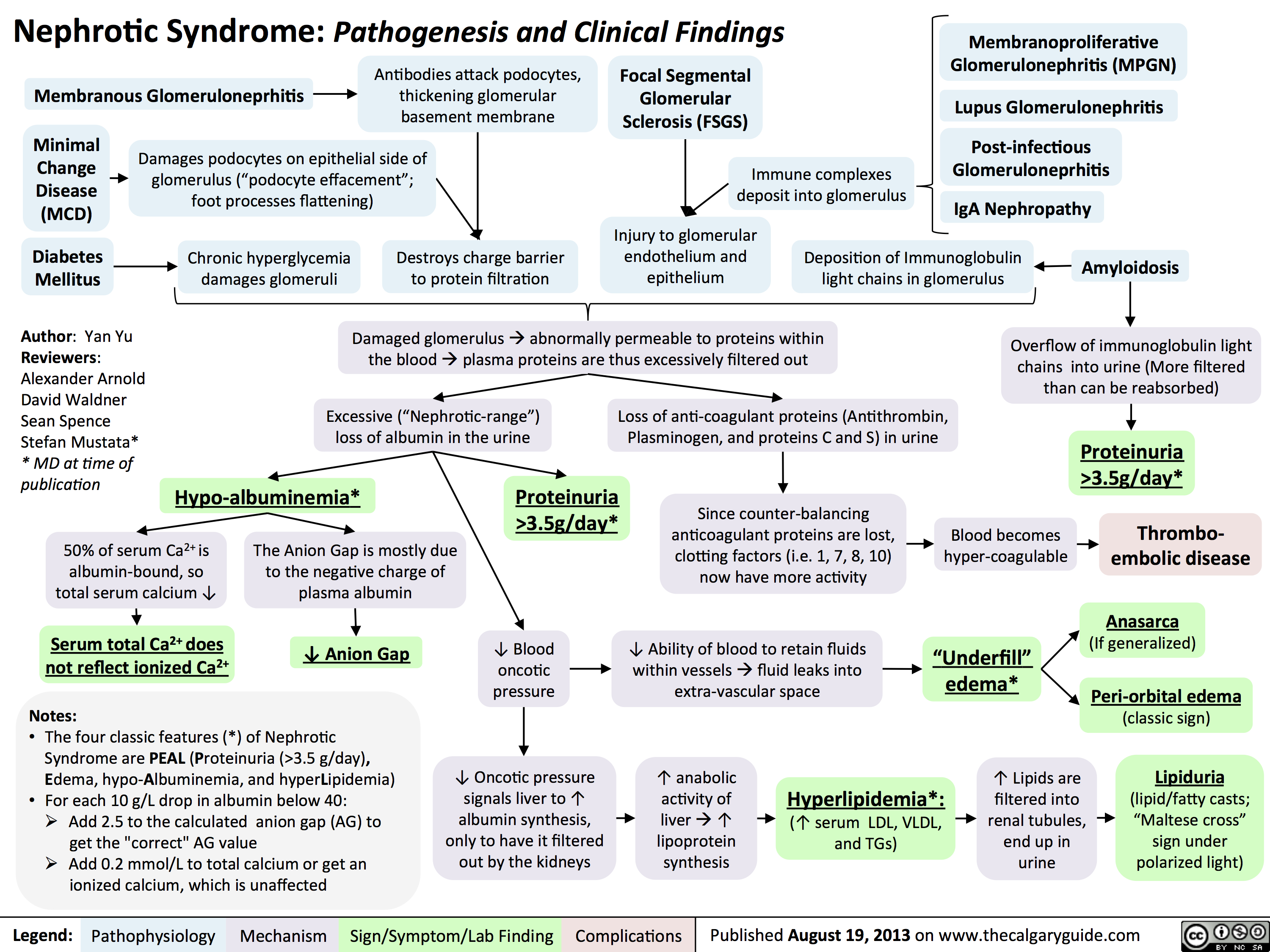 3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
Upper Urinary Tract infection (UUTI): Pathogenesis and Clinical Findings

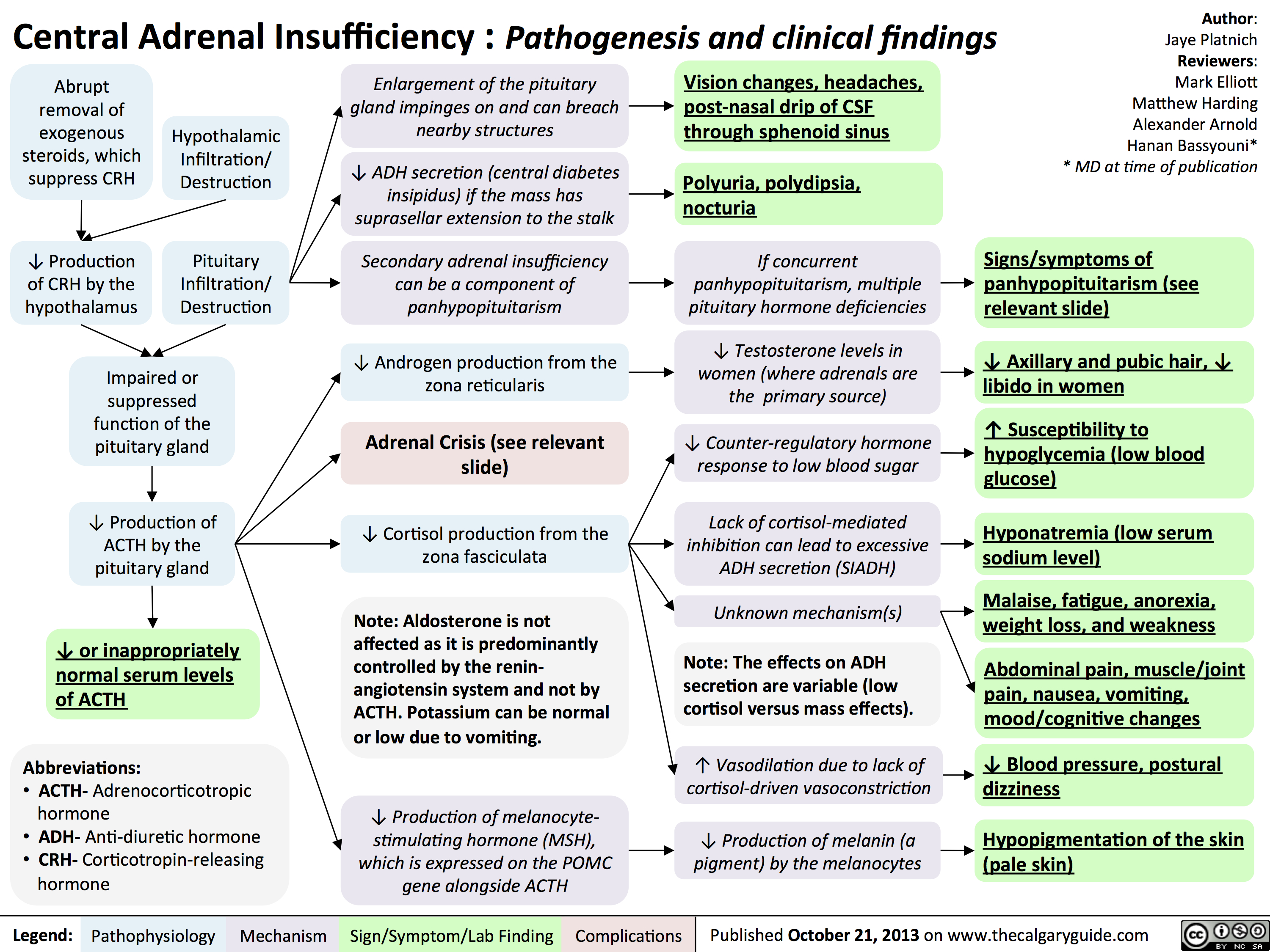
Central Adrenal Insufficiency - Pathogenesis and Clinical Findings
Hypercalcemia - Clinical Findings
![Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hypercalcemia-Clinical-Findings.jpg "Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be")
Pathogenesis of Anxiety Disorders
Sense of foreboding or apprehensionActivation of hypothalamus-pituitary-adrenal cortex axisPredisposition to anxiety: Imbalance and/or abnormal functioning of norepinephrine, serotonin, dopamine, and gamma-aminobutyric acid (GABA) Female gender (may be related to hormonal factors, less internal locus of control, greater reporting rates)Other biological theories (under investigation)Prefrontal Cortex modulation of amygdala impairedUnpleasant tensionAmygdala maladaptively activates fear response? Cortisol releaseChronic activation of stress hormones over time causes death of neurons in the hippocampusAnxiety Disorders:A maladaptive emotional state causing fear, worry, and excessive stress, characterized by:Perceived environmental threatHippocampus and Cingulate Gyrus abnormally process threatActivation of autonomic nervous system and adrenal medulla? Epinephrine releaseHippocampus shrinks in sizeAbility of hippocampus to normally integrate environmental stimuli is further compromisedMood dysregulationMemory impairmentStrong association between anxiety disorders and depressionMeasurable ? in Brain-Derived Neurotrophic factor (BDNF)BDNF value correlates with the degree of neuronal loss in the hippocampus
97 kB / 173 words")
Pre-Renal Acute Kidney Injury Pathogenesis

Hyperosmolar Hyperglycemic State
![Hyperosmolar Hyperglycemic State (HHS)
Note: HHS is only seen in Type II DM patients!
Note: In patients with either DKA or HHS, always look for an underlying cause (i.e. an infection)
Author: Yan Yu Reviewers:
Peter Vetere
Gill Goobie
Hanan Bassyouni* * MD at time of publication
Alters total body water & ion osmosis
Inadequate insulin production, insulin resistance, non- adherence to insulin Tx
Relative Insulin deficit
Stresses that ↑ Insulin demand: infections, pneumonia, MI, pancreatitis, etc)
Hyperglycemia
(Very high blood [glucose], higher than in DKA)
When blood [glucose] > 12mmol/L, glucose filtration > reabsorption, ↑ urine [glucose]
Glucosuria
Glucose in filtrate promotes osmotic diuresis: large- volume urine output
Polyuria
Dehydration
(↓ JVP, orthostasis: postural hypotension/ postural tachycardia, ↑ resting HR)
Some insulin still present, but not enoughsome glucose is utilized by muscle/fat cells, some remain in the blood
Cells not “starved”, but still need more energy
↑ release of Catabolic hormones: Glucagon, Epinephrine, Cortisol, GH
Body tries to ↑ blood [glucose], to hopefully ↑ cell glucose absorption
Hypothalamic cells sense low intra-cellular glucose, triggering feelings of hunger
Polyphagia
Note: the presence of some insulin directly inhibits lipolysis; thus, in HHS there is no ketone body production, and no subsequent metabolic acidosis and ketouria (unlike in DKA). If ketones are detected in an HHS patient it’s likely secondary to starvation or other mechanisms.
↓ ECF volume, ↑ ECF osmolarity (i.e. hypernatremia)
↑ Gluconeogenesis ↑ Glycogenolysis (in liver)
↓ Protein synthesis, ↑ proteolysis
(in muscle)
↑ Gluconeogenic substrates for liver If the patient doesn’t drink enough
water to replenish lost blood volume If pt is alert and
Electrolyte imbalance
water is accessible
Water osmotically leaves neurons, shrinking them
Neural damage: delirium, lethargy, seizure, stupor, coma
↓ renal perfusion, ↓ GFR
Renal Failure
(pre-renal cause; see relevant slides)
Polydipsia Note: in HHS, body K+ is lost via osmotic diuresis. But diffusion of K+ out of cells
may cause serum [K+] to be falsely normal/elevated. To prevent hypokalemia, give IV KCl along with IV insulin as soon as serum K+ <5.0mmol/L. But ensure patient has good renal function/urine output first, to avoid iatrogenic hyperkalemia!
Note: Electrolyte imbalances (i.e. hyperkalemia, hypernatremia) are worsened by the acute renal failure commonly coexisting with DKA/HHS
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 3, 2016 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hyperosmolar-Hyperglycemic-State-HHS.jpg "Hyperosmolar Hyperglycemic State (HHS)
Note: HHS is only seen in Type II DM patients!
Note: In patients with either DKA or HHS, always look for an underlying cause (i.e. an infection)
Author: Yan Yu Reviewers:
Peter Vetere
Gill Goobie
Hanan Bassyouni* * MD at time of publication
Alters total body water & ion osmosis
Inadequate insulin production, insulin resistance, non- adherence to insulin Tx
Relative Insulin deficit
Stresses that ↑ Insulin demand: infections, pneumonia, MI, pancreatitis, etc)
Hyperglycemia
(Very high blood [glucose], higher than in DKA)
When blood [glucose] > 12mmol/L, glucose filtration > reabsorption, ↑ urine [glucose]
Glucosuria
Glucose in filtrate promotes osmotic diuresis: large- volume urine output
Polyuria
Dehydration
(↓ JVP, orthostasis: postural hypotension/ postural tachycardia, ↑ resting HR)
Some insulin still present, but not enoughsome glucose is utilized by muscle/fat cells, some remain in the blood
Cells not “starved”, but still need more energy
↑ release of Catabolic hormones: Glucagon, Epinephrine, Cortisol, GH
Body tries to ↑ blood [glucose], to hopefully ↑ cell glucose absorption
Hypothalamic cells sense low intra-cellular glucose, triggering feelings of hunger
Polyphagia
Note: the presence of some insulin directly inhibits lipolysis; thus, in HHS there is no ketone body production, and no subsequent metabolic acidosis and ketouria (unlike in DKA). If ketones are detected in an HHS patient it’s likely secondary to starvation or other mechanisms.
↓ ECF volume, ↑ ECF osmolarity (i.e. hypernatremia)
↑ Gluconeogenesis ↑ Glycogenolysis (in liver)
↓ Protein synthesis, ↑ proteolysis
(in muscle)
↑ Gluconeogenic substrates for liver If the patient doesn’t drink enough
water to replenish lost blood volume If pt is alert and
Electrolyte imbalance
water is accessible
Water osmotically leaves neurons, shrinking them
Neural damage: delirium, lethargy, seizure, stupor, coma
↓ renal perfusion, ↓ GFR
Renal Failure
(pre-renal cause; see relevant slides)
Polydipsia Note: in HHS, body K+ is lost via osmotic diuresis. But diffusion of K+ out of cells
may cause serum [K+] to be falsely normal/elevated. To prevent hypokalemia, give IV KCl along with IV insulin as soon as serum K+ <5.0mmol/L. But ensure patient has good renal function/urine output first, to avoid iatrogenic hyperkalemia!
Note: Electrolyte imbalances (i.e. hyperkalemia, hypernatremia) are worsened by the acute renal failure commonly coexisting with DKA/HHS
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 3, 2016 on www.thecalgaryguide.com")
chronic-hypertensive-retinopathy-pathogenesis-and-clinical-findings
 • 1° HTN
Retinal Detachment
Vitreous Hemorrhage
Central/Branch Retinal Artery/Vein Occlusions
Risk Factors for 2° HTN (ex. Hyperaldosterone, Cushing's, Acromegaly, Chronic Kidney Disease, Obstructive Sleep Apnea, Diabetes Mellitus, Hypo/Hyper-thyroid, Adrenal Hyperplasia, Renal Artery Stenosis)
2° HTN
Ophthalmic Artery Hypertension ,17
Stage 1: Mild/vasoconstrictive
Stage 2: Moderate/sclerotic
Stage 3: Severe/exudative
Stage 4: Malignant
Abbreviations: • HTN — Hypertension • BRB — Blood-retinal barrier • RPE — Retinal pigment epithelium
Legend:
Pathophysiology
Mechanism
Acute and chronic vasospasm
Authors: Graeme Prosperi-Porta Reviewers: Stephanie Cote Usama Malik Johnathan Wong* * MD at time of publication
Diffuse and focal arterial narrowing and vascular tortuosity
Atherosclerosis and hyalinization causes arteriolar wall thickening resulting in a diffuse light reflex appearing red-brown coloured
Thickening of the arteriolar wall and/or sclerotic thickening at the arteriole/venule crossing compresses the underlying venule
BRB breakdown causes dot/blot hemorrhages in the inner retina and flame hemorrhages in the nerve fiber layer
Serum proteins and lipids leakage from damaged BRB appears as white or yellow areas with sharp margins
Occlusion of the terminal retinal arterioles causes fluffy white ischemic lesions in the inner retinal nerve fiber layer
Hyper-pigmented patches surrounded by a hypo-pigmented ring due to RPE clumping around atrophic areas in the choroid
Sign/Symptom/Lab Finding
lschemia of optic disc arterioles causes optic nerve swelling and blurred disc margins. Leakage of optic disc arterioles causes hemorrhage and disc edema.
Complications
Copper Wiring
AV nicking
Retinal Hemorrhages
Yellow Hard Exudates
Cotton-wool Spots
Elschnig's Spots
Papilledema")
Serotonin Syndrome Pathogenesis and Clinical Findings
, opioids, antiemetic agents, triptans, weight loss agents, drugs of abuse (e.g. cocaine, amphetamines)
Therapeutic drug use
• Drug interactions (esp. combo of serotonergic agents) Serotonin Syndrome Variable combination of mental status changes, autonomic instability, and neuromuscular hyperactivity ranging from mild to life-threatening with an abrupt onset (within minutes to hours) after medication ingestion and most cases resolving within 24 hours of cessation of offending medication
Intentional self-poisoning
Excessive serotonergic activity at 5-HT receptors centrally (brainstem) and peripherally
serotonin synthesis and release
serotonin reuptake and metabolism
IN receptor agonism and sensitivity
4,
Drug-induced changes in the relative ratio of non-serotonergic neurotransmitters (e.g. increase in noradrenaline)
Altered Mental Status
Anxiety, confusion, agitation, hypervigilance, pressured speech, delirium, coma
Autonomic Instability
Shivering, diaphoresis, fever, diarrhea, tachycardia, mydriasis, hypertension
Authors: Preeti Kar Reviewers: Erika Russell Usama Malik Aaron Mackie* * MD at time of publication
Notes: The Hunter Serotonin Toxicity Criteria is used to make a clinical diagnosis • History of serotonergic agent taken within past 5 weeks + any of the following clinical features: • Spontaneous clonus • Inducible clonus and either agitation or diaphoresis • Ocular clonus and either agitation or diaphoresis • Tremor and hyperreflexia • Hypertonia, temperature > 38 °C, and either ocular clonus or inducible clonus
Neuromuscular Hyperactivity
Hyperreflexia, muscle rigidity (esp. lower extremities), myoclonus, tremor, incoordination, trismus*, opisthotonus*, ocular clonus*, seizures
*Notes: • Trismus or lockjaw, is the reduced opening of the jaw • Opisthotonus is an abnormal body position where the person is usually rigid and arches their back, with their head thrown backwards • Ocular Clonus is rhythmic or equal movements of both eyes; should be distinguished from nystagmus which has a fast and slow component
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Abbreviations: • 5-HT = serotonin • SSRI = selective serotonin reuptake inhibitors • SNRI = selective noradrenaline reuptake inhibitors • MOAI = monoamine oxidase inhibitors • TCA = tricyclic antidepressants")
2nd gen antipsychotics (Slovenian translation) - FINAL VERSION
: primeri: klozapin, olanzapin, kvetiapin, risperidon, paliperidon itd.
antagonisti dopaminskih D2 receptorjev zavirajo delovanje DA na D2 receptorjih po celotnih mo2ganih
antagonisti serotoninskih 2A receptorjev zavirajo delovanje 5-HT na 5-HT2A receptorjih po celotnih mo2ganih
antagonisti serotoninskih 2C receptorjev klozapin, olanzapin, kvetiapin
antagonisti ACh M1 receptorjev zavirajo delovanje ACh po telesu (v ustih, prebavilih, o6eh, mo2ganih)
antagonisti aradrenoceptorjev v oiilju dilatacija gladkih migic v stenah arteriol
antagonisti histaminskih H1 receptorjev zavirajo delovanje histamina po telesu
sano-presnovni kink' mehanizem neznan
Legenda:
patofiziologija mehanizem
Pomni: posledica velikih razlik v afiniteti za receptorska vezavna mesta so svojevrstni terapevtski in varnostni profili atipicnih a nti psi hoti kov. Kloza pi n med vsemi velja za najud nkovitejSega, a i ma tudi najve6 neZelenih uC'inkov, vkljUuja agranulocitozo (0,5-2 %). Tako predstavlja terapijo drugega izbora, potrebno je red no spremljanje bolnikove krvne slike.
mezolimbiEna pot DA blokada > 5-HT blokado
nigrostriatna pot 5-HT blokada > DA blokado
4, pozitivnih simptomov terapevtski ueinek
blokada 5-HT vodi v sprokanje DA v striatumu
tubero- blokada 5-HT zavre sprokanje infundibularna pot prolaktina v adenohipofizi
mezokortikalna pot
blokada 5-HT2c receptorjev stimulira sprokanje DA in NA v prefrontalni skorji
zamegljen vid
kognitivna upolasnjenost
sposobnost vzdrievanja krvnega tlaka
omotica
apetit
T tel. tee
ortostatska hipotenzija
tveganje za debelost
trigliceridi na tee
inzulinska odpornost —■ diabetes tipa 2
znak/simptom/laboratorijska najdba
4, halucinacii
blodeni
avtorica: Sara Meunier pregledala: Yan Yu, Aaron Mackie*
* dr. med. ob objavi
prevedel in priredil: Jan KejZar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
4, ekstrapiramidnih simptomov (EPS)*
4, hiperprolaktinemije*
prokognitivni in antidepresivni ainki
4, kognitivnih simptomov* 4, negativnih simptomov*
* Glede na anti-psihotike prve generacije, glej ustreznogradivo!
okrajgave: 5-HT - serotonin DA - dopamin NA - noradrenalin ACh - acetilholin
visoko presnovno tveganje: klozapin, olanzapin zmerno presnovno tveganje: risperidon, kvetiapin nizko presnovnotveganje:antipsihotikitretjegeneracije
1 tveganje za diabeti6no ketoacidozo pri bolnikih z visokim tveganjem tveganje za srbo-iilne dogodke tveganje za prezgodnjo smrt
zaplet Objavljeno 15. junija 2017 na www.thecalgaryguide.com.")
BMR (Slovenian translation) - FINAL VERSION
 )
Pomni: • Bipolar motnja tipa 1: maniba epizoda in/ali depresivna epizoda: priblrino 10 epizod manije in depresije v 2ivljenju bolnika v primeru nezdravljene bolezni • Bipolar motnja tipa 2: hipomaniba epizoda in depresivna epizoda • hipomaniba epizoda predstavlja bla2jo obliko manije, tj. brez funkcionalne okrnjenosti, brez psihotibih simptomov, brez hospitalizacije in v trajanju vsaj 4 zaporednih dni
znak/simptom/laboratorijska najdba
avtorici: Briana Cassetta, Sara Meunier pregledali: Yan Yu, Alexander Arnold, Philip Stokes*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
depresivna epizoda najmanj 2 tedna
depresivno razpoloienje
socialnega urriika
obEutkov krivde, tesnobe
brezupa
samomorilnih misli in vedenja
anhedonija
teiave s pozornostjo
A v spanju, utrujenost
A tel. teie, apetita
psihomotorna agitira nost ali upolasnjenost
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.")
Bupropion (Slovenian translation) - FINAL VERSION
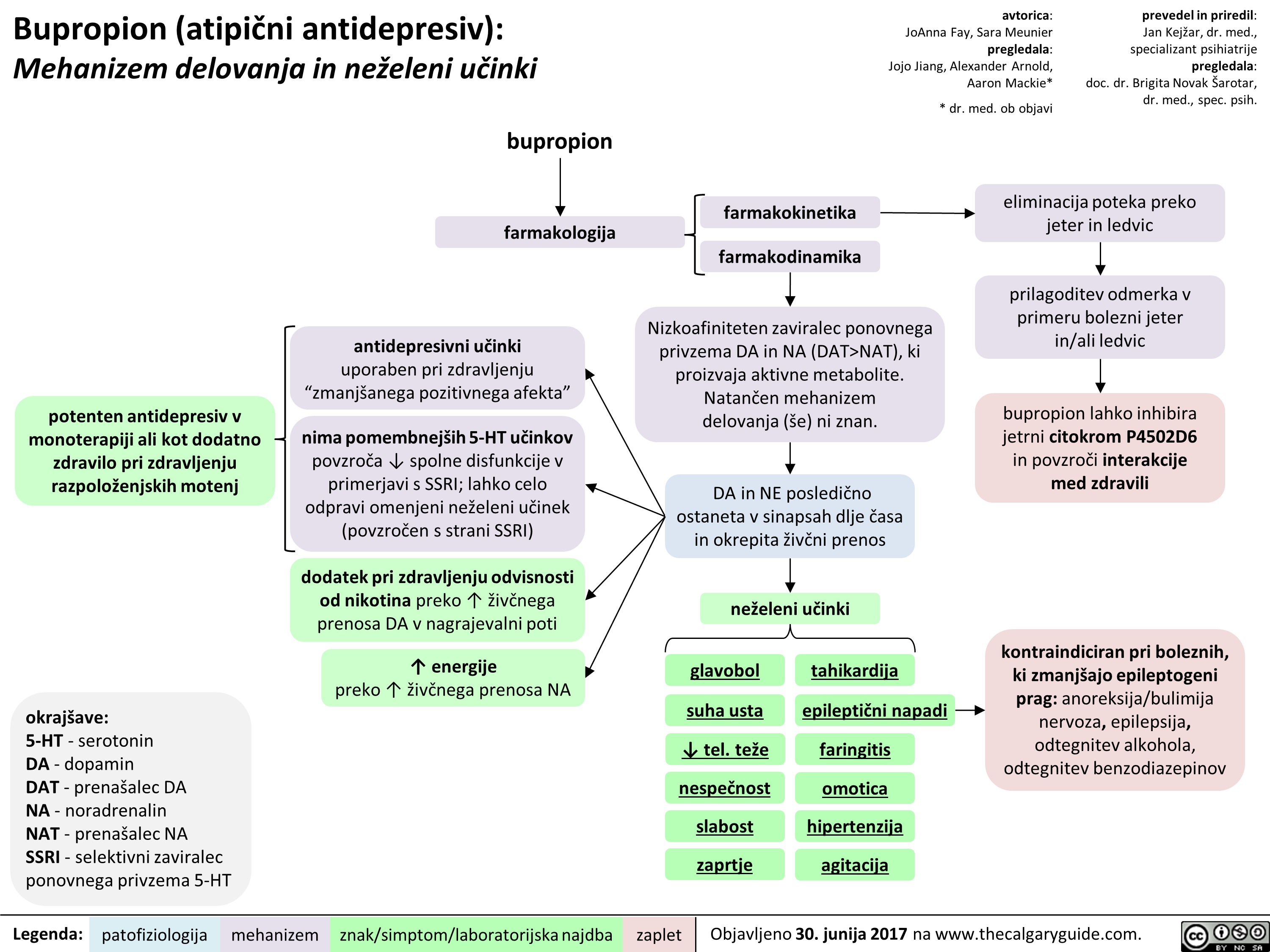 NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" title="Bupropion (atipiEni antidepresiv): Mehanizem delovanja in neieleni utinki
potenten antidepresiv v monoterapiji all kot dodatno zdravilo pri zdravljenju razpoloienjskih motenj
okrajgave: 5-HT - serotonin DA - dopamin DAT - prenagalec DA NA - noradrenalin NAT - prenagalec NA SSRI - selektivni zaviralec ponovnega privzema 5-HT
Legenda:
bupropion
farmakologija
antidepresivni udnki uporaben pri zdravljenju "zmaniganega pozitivnega afekta"
nima pomembnelgih 5-HT udnkov povzraa spolne disfunkcije v primerjavi s SSRI; lahko celo odpravi omenjeni neieleni udnek (povzraen s strani SSRI)
dodatek pri zdravljenju odvisnosti od nikotina preko T iive'nega prenosa DA v nagrajevalni poti
energije preko T 2ivbega prenosa NA
patofiziologija mehanizem
farmakokinetika
farmakodinamika
avtorica: JoAnna Fay, Sara Meunier pregledala: Jojo Jiang, Alexander Arnold, Aaron Mackie*
* dr. med. ob objavi
Nizkoafiniteten zaviralec ponovnega privzema DA in NA (DAT>NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" />
NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" title="Bupropion (atipiEni antidepresiv): Mehanizem delovanja in neieleni utinki
potenten antidepresiv v monoterapiji all kot dodatno zdravilo pri zdravljenju razpoloienjskih motenj
okrajgave: 5-HT - serotonin DA - dopamin DAT - prenagalec DA NA - noradrenalin NAT - prenagalec NA SSRI - selektivni zaviralec ponovnega privzema 5-HT
Legenda:
bupropion
farmakologija
antidepresivni udnki uporaben pri zdravljenju "zmaniganega pozitivnega afekta"
nima pomembnelgih 5-HT udnkov povzraa spolne disfunkcije v primerjavi s SSRI; lahko celo odpravi omenjeni neieleni udnek (povzraen s strani SSRI)
dodatek pri zdravljenju odvisnosti od nikotina preko T iive'nega prenosa DA v nagrajevalni poti
energije preko T 2ivbega prenosa NA
patofiziologija mehanizem
farmakokinetika
farmakodinamika
avtorica: JoAnna Fay, Sara Meunier pregledala: Jojo Jiang, Alexander Arnold, Aaron Mackie*
* dr. med. ob objavi
Nizkoafiniteten zaviralec ponovnega privzema DA in NA (DAT>NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" />
Left Heart Failure: Pathophysiology (Neurohormonal Activation)

Frank Starling Mechanism • The Frank Starling mechanism of the heart represents the relationship between preload (EDV) and SV • As preload (EDV) increases, SV increases, because higher volumes of blood in the ventricles stretch the cardiac fibers and increases cardiac contraction during systole. However, volume overload causes reduced SV.
Myocardial Dysfunction: • Left ventricular Compensatory 4, SV 4A, CO 4 Mechanisms
4, BP
Important equations: • BP = CO x SVR • CO = SV x HR Cardiac hemodynamics: • Stroke volume is affected by three factors 1) Preload (end-diastolic volume (EDV)) 2) Afterload (resistance to LV ejection) 3) Contractility (inherent strength of contraction of LV myocytes) Definition of heart failure: • Myocardial dysfunction (systolic or diastolic) results in decreased CO, such that the heart cannot meet the body's metabolic demands or can only do so at elevated filling pressures
Anti-diuretic hormone (ADH) activation: Arginine 4, BP 4 carotid sinus Vasopressin --• and aortic arch (V2) receptor baroceptors activation activation 4 I` ADH release
RAAS System: 4, BP 4 t release of renin from the juxtaglomerular kidney cells due to renal hypoperfusion
SNS System: In response to CO, 4 SNS t release of (catecholamines) norepinephrine and epinephrine
Adrenal Glands: Aldosterone release
Angiotensin II Type 1 receptor activation
al receptor activation
13, receptor activation
—•
Renal Collecting Ducts: t H2O retention
Renal Distal —• Tubules: t Na+ & H2O retention
Heart: Activation of fibroblasts 4 collagen synthesis and hypertrophy
Blood Vessels: Peripheral vasoconstriction 4 SVR
Heart: Chronic p, receptor activation 4 Ca2+ overload myocyte apoptosis
Heart: Increase HR to maintain normal CO
Maladaptive Response: t preload (EDV), —• volume overload
Abbreviations: • SV — Stroke volume • CO — Cardiac output • SVR — Systemic vascular resistance • BP — Blood pressure • RAAS — Renin-Angiotensin-Aldosterone System • SNS — Sympathetic nervous system
tin systemic and pulmonary congestion via the Frank-Starling Mechanism
Maladaptive 1` resistance Response: t BP, —• against LV afterload ejection 4 4, SV
Maladaptive Response: Adverse LV remodelling
Maladaptive Response: t myocardial oxygen demand and 4, diastolic time
4, contractility —• of the heart
4, coronary blood flow 4 myocardial ischemia
Physical signs and symptoms of congestive heart failure (see relevant slide)
Authors: Sunny Fong Reviewers: —• I Jack Fu Usama Malik Dr. Jason Waechter* *MD at time of publication")
Anksiozne motnje: patogeneza tesnobe

Depresivna epizoda/motnja: patogeneza in klinične najdbe

pomanjkanje tesnih, zaupnih odnosov
druibeni dejavniki
Prevalenca 10-15 % pri 2enskah in 5-12 % pri mogkih. Razmerje med 2enskami in mc&imi 2:1. Pogosteja pri razvezanih, laenih in samskih ter tistih z nizkim druThenoekonomskim stanjem.
depresivna epizoda/motnja simptomi (po DSM 5 merilih) prisotni tekom istega dvotedenskega obdobja in pomenijo odklon od premorbidne ravni funkcioniranja drugi simptomi pomanjkanje libida tesnoba razpolo2enje '6ez dan niha (ang. diurnal variation) huje pozimi (sezonska depresivna motnja) halucinacije (psihotiCna depresija) blodnje (psihotiena depresija) anhedonija (izguba zanimanj/u2itkov) depresivno razpolo2enje nejeknost ali povaan apetit s pridrdienimi spremembami telesne te2e (4, ali 1`) anergija (utrujenost) nespanost ali preva spanja okrajgave: 5-HT - serotonin NA - noradrenalin nastop v mesecu po porodu (poporodna depresija) obC'utki niC'vrednosti ali pretirane krivde psihomotorit'na upaasnjenost ali agitiranost upad spoznavnih sposobnosti (zlasti motnje pozornosti) ponavljajae se misli na smrt/samomor")
Serotoninski sindrom: patogeneza in klinične najdbe
, opioidi, antiemetiki, triptani, zdravila za izgubo tel. te2e, ilegalne psihoaktivne snovi (npr. kokain, amfetamini)
terapevtska raba
1
interakcije (se posebej pri kombinacijah serotoninergikov) namerna samozastrupitev
serotoninski sindrom raznolika kombinacija sprememb v psihiZnem stanju, vegetativne nestabilnosti in iivZnomigiZne hiperaktivnosti, ki sega od blage do iivljenje ogroiajoL'e z nenadnim nastopom (v nekaj minutah do urah) po administraciji zdravil(a), v vecini primerov pa se razregi v <24 urah po prekinitvi jemanja odgovorne snovi
prekomerna serotoninergitha aktivnost 5-HT receptorjev centralno (v moiganskem deblu) in periferno
sinteza in privzem in T receptorski agonizem sprogEanje 5-HT presnova 5-HT in ok'utljivost
z zdravili povzraene spremembe v relativnem razmerju ne-serotoninergithih nevrotransmitorjev (npr. pove6anje konc. noradrenalina)
spremenjeno psihreno stanje
tesnoba, zmedenost, agitacija, hipervigilnost, dolgoveznost, delirij, koma
vegetativna nestabilnost
mrzlica/drgetanje, 6ezmerno potenje, vraina, driska, tahikardija, ra8irjene zenice, hipertenzija
avtorica: Preeti Kar pregledali: Erika Russell, Usama Malik, Aaron Mackie*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
Pomni: za klinicno postavitev diagnoze uporabljamo Hunterjeva merila serotoninske toksiZnosti: - zgodovina jemanja serotoninergithih snovi v preteklih 5 tednih + kateri koli od naslednjih pogojev: • spontani klonus • inducirani klonus in bodisi agitacija bodisi L'ezmerno potenje • aesni klonus in bodisi agitacija bodisi L'ezmerno potenje • tremor in hiperrefleksija • hipertonija, tel. temperatura >38 °C in bodisi aesni klonus bodisi inducirani klonus
ihgnomigiZna hiperaktivnost
hiperrefleksija, mR")
Zaviralci privzema serotonina in noradrenalina (SNRI): mehanizem delovanja in neželeni učinki
: mehanizem delovanja in neieleni utinki
zaviralci privzema serotonina in noradrenalina predstavnika: venlafaksin, duloksetin
konc. 5-HT in NA v 02S/P2S
farmakologija
farmakokinetika farmakodinamika
nenadna prekinitev jemanja zdravila ali vnos
avtorici: JoAnna Fay, Sara Meunier pregledali: Jojo Jiang, Alexander Arnold, Jessica Asgarpour, Aaron Mackie*
iz krvnega obtoka jih odstranijo jetra
zavirajo prenagalec za privzem NA (NET) in prenaalec za privzem 5-HT (SERT)
5-HT in NA ostaneta v sinapsah dlje in podaVata oz. okrepita iiv6ni prenos
odtegnitev namerno predoziranje nenamerno povzrocene interakcije nepri6akovan odziv na terapevtski odmerek prekometna v aktivnost 02S/P2S sindrom 1` 5-HT omotica 5-HT serotoninski omotica driska nejegZnost nespeEnost nespanost slabost utrujenost glavobol vegetativna * iivEnomiKiEne kognitivne hiperaktivnost nepravilnosti spremembe vrtoglavica potencialno iivljenje ogroiajoE spolne hipertenzija olesni klonus agitacija motn'e porast tahikardija tremor akatizra tel. tee raigir-ene hiperrefleksija zenice migiEni klonus
Legenda: patofiziologija
mehanizem
znak/simptom/laboratorijska najdba
1` NA
slabost
Zezmerno potenie
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
v primeru ietrnih bolezni in/ali saasne rabe zaviralcev/sproncev CYPD26 ie potrebna prilagoditev odmerka
izboljganje depresivne in anksiozne simptomatike 1 blokada ponovnega privzema 5-HT in NA v sinapsah pa u6inka SNRI ne pojasni v celoti
posredno SNRI povzro6ijo sproManja nevrozaMitnih proteinov, denimo BDNF, ki bi naj imel po podatkih §tudij protivnetno delovanje
za dosego kliniEnega uZinka ie potrebnih 3-8 tednov all veZ zdravlienia
okralgave in opombe: 5-HT— serotonin NA— noradrenalin BDNF — mo2ganski nevrotrofiEni faktor 025 — osrednji 2ivEni sistem P2S — periferni 2ivEni sistem *vegetativen — nanagajoE se na avtonomni 2ivEni sistem")
Socialna anksiozna motnja: patogeneza in klinične najdbe

Impetigo Pathogenesis and clinical findings

Fisiologi sistem Renin-Angiotensin-Aldosteron (RAAS)

Hipoperfusi Ginjal
Regangan baroreseptor pada dinding arteriol aferen
Hipotensi/ Hipovolemia
9 Pengiriman NaCI ke Makula Densa
9 Tekanan dirasakan oleh Baroreseptor Jantung & Arteri
Katekolamin di sirkulasi
Aktivitas saraf simpatis pada arteriol aferen
Stimulasi reseptorn-adrenergik pada arteriol aferen
Keseimbangan Glomerulotubuler (Mekanisme intrinsik ginjal diluar RAAS) *Hanya sebagian dari mekanisme tersebut
Angiotensin II 4 konstriksi arteriol eferen
01% Tekanan hidrostatik glomerulus
Jumlah cairan yang disaring
+ Konsentrasi sisa protein darah di glomerulus
Darah kental bergerak dari glomerulus menuju kapiler peritubuler
it pada kapiler peritubuler
9 Tekanan hidrostatik peritubular
Legenda:
Patofisiologi Mekanisme
Pelepasan Renin oleh sel-sel Jukstaglomerular pada arteriol aferen 4 berujung pada T Angiotensin II
Sekresi aldosterone dari korteks adrenal
1
Insersi KNaE pada Sel Prinsipal di DK
■
Aktivitas transporter NHE3 di dalam PCT
Reabsorpsi Na ke dalam darah, menarik H2O ke dalam darah melalui osmosis
Reabsorpsi H2O langsung ke dalam sirkulasi darah (via aliran gradien tekanan onkotik dan hidrostatik H2O)
Tanda/Gejala/Penunjang
Komplikasi
Author: David Waldner Reviewers: Yan Yu Sean Spence Sophia Chou* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Hati secara normal mensintesis angiotensinogen dengan laju basal, melepaskannya ke dalam sirkulasi darah:
Vasokonstri ksi arteri sistemik
Tekanan darah
Daftar singkatan: • ACE: Angiotensin Converting Enzyme (disintesis oleh Ginjal dan Paru) • DK: Duktus Kolektivus • PCT: Tubulus Konturtus Proksimal • NHE3: Sodium Hydrogen Exchanger (Antiport) 3 • KNaE: Kanal Natrium (Sodium) Epitel • n:Tekanan onkotik")
Acetylcholinesterase Inhibitors
 effects
Salivation
Peristalsis
► Bradycardia
Bronchoconstriction
Bronchial Secretions
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
non-depolarizing-neuromuscular-blocks-ndnmbs
 Eg. pancuronium, rocuronium, atracurium, vecuronium
Abbreviations NDNMBs — Non-Depolarizing Neuromuscular Blockers ACh — Acetylcholine
Quick Facts 1° Indication = Skeletal muscle paralysis to facilitate tracheal intubation, and used during indicated surgeries or mechanical ventilation
Route of Administration = IV
Metabolism & Excretion = Redistribution, hepatic clearance/renal excretion (extent varies greatly by drug). NOT degraded by acetylcholinesterase or pseudocholinesterase
See Acetylcholinesterase Inhibitors slide for reversal of NDN M Bs
Competitive antagonism at post-synaptic nicotinic receptors on muscles
Competitive antagonism at the pre-synaptic nicotinic receptors on neurons
Vagolytic effect (esp. pancuronium)
Anaphylactic/ anaphylactoid reactions
4, Binding sites for ACh at post-synaptic nicotinic receptors on muscles
4, Binding sites for ACh at pre-synaptic nicotinic receptors on neurons
Blockage of vagal muscarinic receptors in sinoatrial nodes
IgE antibodies attach to ammonium ion components of NDNMBs Non-immunologic mast cell degranulation (esp. atracurium)
4, Muscle cell depolarization
4, Positive feedback for continued ACh ► release in response to high frequency stimulation
Skeletal muscle paralysis
Tetanic fade, Train-of-Four fade
4, —• Parasympathetic Tachycardia effects on heart
Release of histamine from mast cells and basophils
Bronchospasm
Hypotension
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Propofol

4, Cerebral metabolic rate CNS —÷ 4, Cerebral oxygen consumption 4, Intra-cranial pressure
4, Systemic vascular resistance Hypotension ► Cardiovascular --■ —■ (with no change 4, Preload in heart rate) 4, Contractility
Respiratory /
♦ Hypercapnia 4, Hypoxic and --■ hypercapnic Hypoxia respiratory drive ♦ Apnea
4, Upper airway reflexes
Complications I Published MARCH 3, 2018 on www.thecalgaryguide.com
Lac.).T2")
non-depolarizing-neuromuscular-blocks-ndnmbs
 Eg. pancuronium, rocuronium, atracurium, vecuronium
Abbreviations NDNMBs — Non-Depolarizing Neuromuscular Blockers ACh — Acetylcholine
Quick Facts 1° Indication = Skeletal muscle paralysis to facilitate tracheal intubation, and used during indicated surgeries or mechanical ventilation
Route of Administration = IV
Metabolism & Excretion = Redistribution, hepatic clearance/renal excretion (extent varies greatly by drug). NOT degraded by acetylcholinesterase or pseudocholinesterase
See Acetylcholinesterase Inhibitors slide for reversal of NDN M Bs
Competitive antagonism at post-synaptic nicotinic receptors on muscles
Competitive antagonism at the pre-synaptic nicotinic receptors on neurons
Vagolytic effect (esp. pancuronium)
Anaphylactic/ anaphylactoid reactions
4, Binding sites for ACh at post-synaptic nicotinic receptors on muscles
4, Binding sites for ACh at pre-synaptic nicotinic receptors on neurons
Blockage of vagal muscarinic receptors in sinoatrial nodes
IgE antibodies attach to ammonium ion components of NDNMBs Non-immunologic mast cell degranulation (esp. atracurium)
4, Muscle cell depolarization
4, Positive feedback for continued ACh ► release in response to high frequency stimulation
Skeletal muscle paralysis
Tetanic fade, Train-of-Four fade
4, —• Parasympathetic Tachycardia effects on heart
Release of histamine from mast cells and basophils
Bronchospasm
Hypotension
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Celiac Disease: Pathogenesis and clinical findings

Genetic predisposition -■ (Northern European, Down's syndrome, Associated with HLA DQ 2,8)
Note: *The anti-TTG antibody is an IgA anti-body, therefore if the patient is IgA-deficient, absence of anti-TTG does not rule out celiac
Anti-TTG in serum*
Anti-TTG reacts with TTG in skin
Deposition of anti-TTG in renal glomeruli
Dermatitis herpetiformis
Chronic Kidney Disease
Small Bowel Biopsy: Crypts of bowel become enlarged (hyperplasia) with architectural change, villous shortening
Legend: Pathophysiology
Mechanism
Exposure to prolamins (proteins found in wheat, rye, oats, barley)
TTG alters prolamin Altered protein fits more easily into HLA
HLA activates adaptive immunity
IgA generated against prolamin-TTG
Wheat prolamin (gliandin) interacts with and activates zonulin signalling
Gut epithelium becomes more porous
Large dietary proteins in epithelium disrupt tight junctions
Author: Matthew Harding Yan Yu Peter Bishay Reviewers: Dean Percy Jason Baserman Usama Malik Kerri Novak* * MD at time of publication
Inflammation of Intestinal epithelium Inflammation disrupts structure of bowel mucosa Mechanism Unknown Lymphocytes migrate to site of inflammation Extraintestinal Complications: Arthropathy Ataxia (gluten associated) Infertility Mild Hepatitis Villi of intestine atrophy Risk of Microscopic Colitis (50x) Malabsorption Extraintestinal manifestations: Chronic watery Fatigue Failure to thrive, weight loss Anemia (Fe, B12, folate) Peripheral neuropathy (B12, Ca) Ataxia (Ca) Dysrhythmia (Ca, K) Osteoporosis (Vit D, Ca) diarrhea + Intestinal manifestations steatorrhea: Pale, foul-smelling Abdominal bloating Steatorrhea (fat in stool) Diarrhea")
Kallmann Syndrome and Normosmotic Idiopathic Hypogonadotropism: Pathogenesis and Clinical Findings
 and Normosmic Idiopathic Hypogonadotropic Hypogonadism (nIHH): Pathogenesis and clinical findings
Authors: Danielle Lynch Reviewers: Nicola Adderley Josephine Ho* * MD at time of publication
Abbreviations:
GnRH – gonadotropin- releasing hormone
LH – luteinizing hormone FSH - follicle stimulating hormone
Notes:
• 4 male : 1 female
• KS, nIHH, and isolated
anosmia exist on a
spectrum
• KS has X-linked recessive,
autosomal dominant, autosomal recessive,
oligogenic, and idiopathic
forms
• KS and nIHH are also
associated with gene- specific features such as
cleft lip/palate, oculomotor synkinesis, hearing loss, and unilateral renal aplasia
• Diagnosis typically occurs around pubertal age, but may be earlier in males if micropenis and cryptorchidism are present at birth
Mutations in KAL1, NELF, and PROKR2
Abnormal olfactory bulb development
Mutations in FGFR1, FGF8, PROK2, PROKR2, HS6ST1, CHD7, WRD11, and SEMA3A or idiopathic
Mutations in
GNRH1, KISS1, KISS1R, TAC3, TACR3
Impaired migration of olfactory neurons from olfactory bulb to hypothalamus
Impaired migration of GnRH neurons from olfactory bulb to hypothalamus
Impaired GnRH neuron activity
Kallmann syndrome
(idiopathic hypogonadotropic hypogonadism with anosmia)
Normosmic idiopathic hypogonadotropic hypogonadism
Anosmia
Olfactory bulb aplasia
Abnormal /absent olfactory bulb on MRI
↓ GnRH ↓LH and ↓FSH
Delayed or absent puberty
Infertility
↓estrogen
In males: ↓testosterone
Cryptorchidism
Delayed epiphyseal plate closure
Micropenis (5-10%)
Uninhibited long bone growth
↑ length hands, arms, legs
Delayed bone age (hand/wrist x-ray)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 29, 2018 on www.thecalgaryguide.com")
Feedback Loop: Adrenocorticotropic Hormone (ACTH)

Authors: Rhiannon Brett Reviewers: Andrea Kuczynski Bernard Corenblum* * MD at time of publication
Posterior Pituitary Gland
ADH
-
-
-
Hypothalamus
CRH
+
Anterior Pituitary Gland
ACTH, MSH, other hormones produced from POMC
ACTH
+
Adrenal Cortex
Activate ACTHR
Activate cAMP Activate PKA Activate Zona Fasciculata
Cortisol
Abbreviations:
CRH: Corticotropin Releasing Hormone
ADH: Anti-diuretic Hormone
ACTH: Adrenocorticotropic Hormone
MSH: Melanocyte Stimulating Hormone
POMC: Pro-Opiomelanocortin
ACTHR: ACTH Receptor
cAMP: Cyclic Adenosine Monophosphate
PKA: Protein Kinase A
DHEA(S): Dehydroepiandrosterone (sulfonated form) F: Female
M: Male
Excess: hirsutism, acne, oily skin, oligo- or amenorrhea, virilization in F
Deficiency: symptoms not typically seen due to gonadal production
Note:
Activate Zona Reticularis Activate Zona Glomerulosa
(minor effect)
Excess: central obesity, hirsutism, violaceous striae, weakness
Deficiency: weight loss, fatigue, weakness, nausea/vomiting, diarrhea
DHEA(S) Aldosterone
Specific to primary adrenal insufficiency: ↑ pigmentation, hyperkalemia
• Virilization is a red flag for an androgen- secreting tumor
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 2, 2018 on www.thecalgaryguide.com")
intrauterine-growth-restriction-iugr-pathogenesis
: Pathogenesis
Authors: Ricki Hagen Reviewers: Jaimie Bird Sarah McQuillan* * MD at time of publication
Abbreviations:
• DM: diabetes mellitus
• HTN: hypertension • IUGR: intrauterine growth restriction
• SGA: small for gestational age
• SLE: systemic lupus erythematosus
• TORCH: Toxoplasmosis, Others, Rubella, CMV, HSV
Maternal Factors
Maternal-Fetal Factors Placental malformations
(Ex. previa, accreta, infarction, abnormal implantation, ischemia)
Gestational HTN/ Preeclampsia
Multiple gestation Gestational DM
Fetal Factors Structural anomalies
(often comorbid with cytogenetic disorders)
Congenital infections
(Ex. TORCH)
Inborn errors of metabolism
Chromosomal disorders/ genetic syndromes
Multiple unclear intrinsic fetal mechanisms
Note:
Teratogenic medications (Ex. Warafin, Valproic Acid, Folic Acid Antagonists)
High altitude living
Smoking, ETOH and/or drug use
Malnutrition/ Low pre-gestational weight
Multiple unclear extrinsic fetal mechanisms
Medical conditions
(Ex: chronic HTN, cyanotic heart disease, severe chronic anemia, kidney disease)
Autoimmune conditions (Ex. Type 1 DM, SLE)
Decreased uteroplacental blood flow
Nutrient supply to fetus compromised
Reduction of total body mass, bone
mineral content, and muscle mass
Blood flow redirected away from vital organs to brain, placenta, heart and adrenal glands
Reduction of overall fetal size to increase survival
IUGR
Failure to reach genetically determined growth potential
• IUGR is not synonymous with SGA • Constitutional SGA is due to
paternal and maternal factors such as height, weight, ethnicity, and parity; it is not associated with increased risk for infant mortality or morbidity
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October, 30, 2018 on www.thecalgaryguide.com")
fetal-alcohol-spectrum-disorder-pathogenesis-and-clinical-findings

Maternal alcohol consumption during pregnancy (greatest risk with binge drinking and daily/chronic intake)
Prenatal alcohol exposure to fetus via placenta-umbilical transport
Notes:
Fetal Alcohol Spectrum Disorder with Sentinel Facial Features (confirmed or unknown PAE)
Fetal Alcohol Spectrum Disorder without Sentinel Facial Features
• There is no known safe amount of prenatal alcohol exposure
(PAE). Although PAE below the threshold of >7 drinks/week or > 2 binge episodes (one binge episode is >4 drinks in one sitting) has not been associated with neurodevelopmental effects, there is insufficient objective evidence to deem this level of alcohol exposure safe.
Sentinel Facial Features
(confirmed PAE) Alcohol exposure between Alcohol acts directly as a teratogen
Vasoconstriction of placental-umbilical unit ̄ blood flow and ̄ oxygen delivery to fetus
Notes (continued):
• A multidisciplinary team is necessary for an accurate and comprehensive diagnosis and subsequent recommendations. Canadian Guidelines for diagnosis, 4-digit code, the APP Toolkit, University of Washington Lip- Philtrum Guide are different methods of assessing and diagnosing patients.
• While not specific to FASD, congenital abnormalities (e.g. heart defects, renal problems, auditory/visual impairments, skeletal defects) and growth deficits (prenatal and/or postnatal height or weight ≤ 10th percentile) are often associated with this disorder.
Smooth philtrum
Thin upper lip
day 15 and 22 of & indirectly via its metabolites pregnancy (most often)
Neuronal cell death & disruption of migration & proliferation Altered signaling, neurotransmitter imbalance, & neural connectivity Evidence of impairment in 3+ neurodevelopmental domains
Small palpebral fissures
(≥2 SDs below the mean for age & sex or < 3rd percentile)
Language Memory Attention Motor skills Cognition Affect regulation
Academic achievement
Executive function (including hyperactivity & impulsivity)
Neuroanatomy/ Neurophysiology (e.g. seizure disorder, abnormal brain structure as seen on brain imaging, microcephaly (head circumference ≤ 10th percentile))
Adaptive behavior, social skills, or social communication
Failure to reach age-appropriate milestones, challenges at school, aggression, delinquency, mental health challenges, substance use disorders
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 30, 2018 on www.thecalgaryguide.com")
Vesicoureteric reflux (VUR): Pathogenesis and clinical findings
: Pathogenesis and clinical findings
Authors: Nicola Adderley Reviewers: Emily Ryznar *Lindsay Long * MD at time of publication
Abnormal function
Abnormal anatomy
Neurogenic bladder (e.g. cerebral palsy, constipation, spinal injury, iatrogenic)
Non-neurogenic bladder (neuropsychological)
Lower urinary tract abnormality (posterior urethral valves, meatal stenosis)
Bladder outlet obstruction
↑ pressure distorts UVJ
Upper urinary tract abnormality (ureters)
UVJ abnormality
Incomplete closure of UVJ during bladder contraction
Abbreviations
• UVJ - ureterovesicular junction • UTI – urinary tract infection
Failure of bladder sphincter to relax during bladder contraction
Vesicoureteric reflux (VUR):
Back flow of urine from the bladder into one or both ureters +/- kidneys
Migration of lower urinary tract bacteria to kidneys
Bacterial invasion of renal parenchyma
Upper UTI (pyelonephritis)
Incomplete emptying of bladder during Abnormal
↑ pressure in bladder
Bladder dilates
Dilated bladder on U/S
urination
Bacteria in bladder are not cleared during urination
voiding habits
↑ bladder capacity
Renal scarring
↓ functional renal tissue
*Chronic kidney disease (↓ GFR,
hypertension, proteinuria)
Flank tenderness
Fever, dysuria, urgency, frequency
Lower UTI (cystitis) Urinary stasis
Cloudy, foul- smelling urine
Urethral stricture
Notes
Urgency, dysuria, frequency
• First febrile UTI in an infant should trigger a work-up for VUR
• High likelihood of spontaneous resolution • *Late complication of severe VUR
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com")
Anticonvulsants as Mood Stabilizers: Mechanism and Side-effect
, thrombocytopenia
Abbreviations: • VSSCs: Voltage-Sensitive Sodium Channels")
Microangiopathic Hemolytic Anemia: Pathogenesis and clinical findings

↓ Inhibition of complement
Immune inflammatory
↑ Pressure in
↑ Extrinsic clotting pathway activation
TTP
(See TTP-HUS Slide)
Disruption of
endothelial cell
activation perfusion/ischemia response metabolism vasculature ↑Thrombin Deficient
Placental under-
renal afferent
↑ Complement pathway activation
MAC-mediated cell lysis
Cytokine release
Endothelial injury
Shear stress on endothelium
production
↑ Fibrin clot production and deposition in small vessels
ADAMTS13 protease enzyme
↓ Cleavage and ↑ accumulation of VWF multimers
Abbreviations:
• HELLP - Hemolysis, Elevated Liver Enzymes, Low Platelets • HUS - Hemolytic-Uremic Syndrome
• DIC - Disseminated Intravascular Coagulation
• TTP - Thrombotic Thrombocytopenic Purpura
• MAC - Membrane Attack Complex
• STEC - Shiga Toxin-Producing Escherichia coli
• VWF - Von Willebrand Factor
Pro-thrombotic Environment (see Virchow’s Triad Slide)
Platelet aggregation Mechanical obstruction of the vessel lumen
Hypercoagulable state
Thrombocytopenia
↑ RBC production in bone marrow
↑ Reticulocytes
Hemoglobin released from damaged RBCs Shearing of RBCs Anemia
Binds to haptoglobin Conversion to bilirubin in liver
↓ Free haptoglobin ↑Indirect bilirubin
Shistocytes Jaundice
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 13, 2018 on www.thecalgaryguide.com")
Hypernatremia Physiology
![Hypernatremia: Physiology Unreplaced H2O loss
Hypodipsia
H2O shift into cells
Severe exercise, electroshock induced seizures
Transient ↑ cell osmolality
Na+ overload
Inappropriate IV hypertonic solution, salt poisoning
Abbreviations:
H2O: Water
GI: Gastrointestinal
DM: Diabetes Mellitus
DI: Diabetes Insipidus
Na+: Sodium ion
IV: Intravenous
ADH: Antidiuretic Hormone LOC: Level of Consciousness
Skin
Sweat, burns
GI
Vomiting, bleeding, osmotic diarrhea
Fluid [Na+] < serum [Na+]
↑ H2O loss compared to Na+ loss
Renal
DM, Mannitol, Diuretics
Absent thirst mechanism
Hypothalamic lesion impairs normal drive for H2O intake
Nephrogenic
↑ renal resistance to ADH
H2O Deprivation Test + no AVP response
↓ access to H2O
DI
Central
↓ ADH secretion
H2O Deprivation Test + AVP response
↑ [Na+] 10- 15 mEq/L within a few minutes
Weakness, irritability, seizures, coma
↑ thirst, ↓ urinary frequency and volume
Note:
Hypernatremia
Serum [Na+] > 145 mmol/L
Intracranial hemorrhage
Headache, vomiting, ↓ LOC
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Effects on plasma [Na+] of IV fluids or loss of bodily fluids is determined by the tonicity of the fluid, not the osmolality.
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/01/Hypernatremia-Physiology-.jpg "Hypernatremia: Physiology Unreplaced H2O loss
Hypodipsia
H2O shift into cells
Severe exercise, electroshock induced seizures
Transient ↑ cell osmolality
Na+ overload
Inappropriate IV hypertonic solution, salt poisoning
Abbreviations:
H2O: Water
GI: Gastrointestinal
DM: Diabetes Mellitus
DI: Diabetes Insipidus
Na+: Sodium ion
IV: Intravenous
ADH: Antidiuretic Hormone LOC: Level of Consciousness
Skin
Sweat, burns
GI
Vomiting, bleeding, osmotic diarrhea
Fluid [Na+] < serum [Na+]
↑ H2O loss compared to Na+ loss
Renal
DM, Mannitol, Diuretics
Absent thirst mechanism
Hypothalamic lesion impairs normal drive for H2O intake
Nephrogenic
↑ renal resistance to ADH
H2O Deprivation Test + no AVP response
↓ access to H2O
DI
Central
↓ ADH secretion
H2O Deprivation Test + AVP response
↑ [Na+] 10- 15 mEq/L within a few minutes
Weakness, irritability, seizures, coma
↑ thirst, ↓ urinary frequency and volume
Note:
Hypernatremia
Serum [Na+] > 145 mmol/L
Intracranial hemorrhage
Headache, vomiting, ↓ LOC
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Effects on plasma [Na+] of IV fluids or loss of bodily fluids is determined by the tonicity of the fluid, not the osmolality.
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com")
Hyponatremia- Physiology
![Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/01/Hyponatremia-Physiology-.jpg "Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com")
adrenergic-agonists-for-treating-hypotensionlow-blood-pressure
 β1-receptor
activation on
cardiac
myocytes
↑ contractility
α1-receptor
activation on
the smooth
muscle of blood
vessel walls
↑ intra-cellular Ca2+
in these cells, ↑
their contraction
Ephedrine
Direct
effect
Indirect
effect
↑ release of endogenous norepinephrine
from the adrenal medulla (see above)
Mimics epinephrine
(see above)
Primary
Indications:
anaphylaxis,
cardiac arrest
Primary
Indications:
Hypovolemic states
(e.g. blood loss),
Low systemic
vascular resistance
states (e.g. sepsis,
Anesthesia-induced
hypotension)
Primary
Indications:
mainly used in
Anesthesiainduced
hypotension
↑ intracellular
Ca2+ ↑ rate of
myocyte
contraction
Phenylephrine
↑ Cardiac
Output
↑ heart rate
↑ strength
of myocyte
contraction
↑ arterial
wall tone
↑
stroke
volume
Pushes more
blood to flow
back to heart
(↑ preload)
↑ systemic vascular
resistance (SVR)
More blood in
ventricles stretch
myocytes more
optimally for ↑
contractility
(Frank Starling
Law)
↑ venous
wall tone
↑ Blood
Pressure
Nonspecific activation of α and β receptors on other areas of the body
(e.g. on the autonomic nervous system) as well as on cardiac myocytes
Hypertension
Cardiac Dysrythmias: e.g.
palpitations, ventricular fibrillation
Tremors Cardiac
arrest
All four
drugs")
Hyperkalemia- Physiology
![Hyperkalemia: Physiology ↓ Renal Excretion
↑ Intake
↓ Intracellular Shift
Acute and chronic kidney disease; CHF
Principal Cell Dysfunction (TTKG < 7)
ACEi/ARB; AI; heparin
Hypovolemia (TTKG > 7)
↓ EABV
↓ distal flow of Na+ and H2O
Urine [Na+] < 20 mmol/L
Cell lysis
↑ osmolarity H2O efflux
Solvent drag
β2 inhibition α1 stimulation
Digoxin ↓ A
NAGMA ↓ insulin
↓ NHE1 activity
Diabetic nephropathy; NSAIDs
↓ A: ↓ R
K+ sparing diuretics; voltage- dependent RTA
↓ Na+/K+ ATPase activity
↓ GFR
↓ A: ↑ R ↑ A: ↑ R
↓ CCD K+ secretion
↑ K+ availability
↑ K+ release
↓ intracellular K+ influx
Chronic: Desensitize voltage- gated Na+ channels and ↓ membrane excitability
ECG: Peaked T-waves, ↑ PR interval, flat/absent P-wave, ↑ QRS, QRST “sine wave”
Hyperkalemia
Serum [K+] > 5.1 mmol/L
Acute: ↑ extracellular [K+] makes the RMP less (-)
Abbreviations:
A: Aldosterone
AI: Adrenal Insufficiency
CCD: Cortical Collecting Duct
CHF: Congestive Heart Failure
EABV: Effective Arterial Blood Volume H+: Hydrogen ion
K+: Potassium ion
Na+: Sodium ion
NAGMA: Normal Anion Gap Metabolic Acidosis
NSAIDs: Non-steroidal anti-inflammatory drugs Note:
Muscle weakness or paralysis, ↓ urinary acid excretion
R: Renin
RTA: Renal Tubular Acidosis
RMP: Resting Membrane Potential TTKG: Transtubular Potassium Gradient
• Pseudohyperkalemia should always be excluded; can be caused by thrombocytosis, leukocytosis or improper blood withdrawal technique.
Authors: Mannat Dhillon Joshua Low Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/03/Hyperkalemia-Physiology-.jpg "Hyperkalemia: Physiology ↓ Renal Excretion
↑ Intake
↓ Intracellular Shift
Acute and chronic kidney disease; CHF
Principal Cell Dysfunction (TTKG < 7)
ACEi/ARB; AI; heparin
Hypovolemia (TTKG > 7)
↓ EABV
↓ distal flow of Na+ and H2O
Urine [Na+] < 20 mmol/L
Cell lysis
↑ osmolarity H2O efflux
Solvent drag
β2 inhibition α1 stimulation
Digoxin ↓ A
NAGMA ↓ insulin
↓ NHE1 activity
Diabetic nephropathy; NSAIDs
↓ A: ↓ R
K+ sparing diuretics; voltage- dependent RTA
↓ Na+/K+ ATPase activity
↓ GFR
↓ A: ↑ R ↑ A: ↑ R
↓ CCD K+ secretion
↑ K+ availability
↑ K+ release
↓ intracellular K+ influx
Chronic: Desensitize voltage- gated Na+ channels and ↓ membrane excitability
ECG: Peaked T-waves, ↑ PR interval, flat/absent P-wave, ↑ QRS, QRST “sine wave”
Hyperkalemia
Serum [K+] > 5.1 mmol/L
Acute: ↑ extracellular [K+] makes the RMP less (-)
Abbreviations:
A: Aldosterone
AI: Adrenal Insufficiency
CCD: Cortical Collecting Duct
CHF: Congestive Heart Failure
EABV: Effective Arterial Blood Volume H+: Hydrogen ion
K+: Potassium ion
Na+: Sodium ion
NAGMA: Normal Anion Gap Metabolic Acidosis
NSAIDs: Non-steroidal anti-inflammatory drugs Note:
Muscle weakness or paralysis, ↓ urinary acid excretion
R: Renin
RTA: Renal Tubular Acidosis
RMP: Resting Membrane Potential TTKG: Transtubular Potassium Gradient
• Pseudohyperkalemia should always be excluded; can be caused by thrombocytosis, leukocytosis or improper blood withdrawal technique.
Authors: Mannat Dhillon Joshua Low Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com")
autosomal-dominant-polycystic-kidney-disease-adpkd
:
Pathogenesis,
Clinical Findings,
and Complications
Author:
Yan Yu*
Reviewers:
David Waldner*
Sean Spence*
Andrew Wade*
* MD at time of
publication
Legend: Published April 14, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
One theory (mechanism unclear): these mutations in the polycystin
gene result in dysfunctional Ca2+ channels on epithelial cells
PKD1 mutation
(~78%)
Abnormal Ca2+ entry disrupts intracellular Ca2+ signaling
In the Kidney: all segments of the nephron develop cysts: sacs of flattened epithelium
filled with proteinaceous fluid, replacing normal parenchyma with dysfunctional tissue
PKD2 mutation
(~15%)
Expansive cell
proliferation
Low urine
Osmolality
(< 500
mmol/kg)
Abnormally expandable
basement membranes
PKD3 mutation
(rare)
↑ fluid
secretion
95% inherited, autosomal dominant mutations
5% spontaneous mutations
In adults, the same pathophysiology occurs
in epithelial tissue throughout the body
When pH of urine <5.5, uric acid is in
its protonated form & is less soluble
àprecipitates uric acid stones
Nephrolithiasis
Urine accumulates within cysts Cyst growth
Pyelonephritis
Damaged
tubules
leak
proteins
into filtrate
Proteinuria
Flank pain
Inability to
concentrate
urine
Low urine
specific
gravity
(<1.010)
¯ NH3 production,
↑ acidity of renal
tubule (¯ pH)
Activates
nociceptors Cyst hemorrhage
Urine stasis à
precipitation of
CaOxalate stones
within cysts
Multiple Renal Cysts
(bilaterally, in cortex and
medulla, on Ultrasound)
In the Brain:
expansion &
weakening of
cerebral
arterial walls
“Berry
Aneurysms” 9-
12%
(ask about this
on Family Hx!)
In many organs:
epithelial tissue
expansion &
fluid secretion
In the Heart:
abnormal valve
collagen matrix
Valve prolapse
& regurgitation
Liver (90%),
spleen/pancreas
(5-10%), thyroid
(rare) cysts
In seminal vesicles:
Cyst formation disrupts
sperm motility
Infertility
In GI tract: Cyst
formation
Herniations,
diverticuli
Dysfunctional
collecting ducts
Abdominal mass
(enlarged kidneys)
(may be palpable)
Blood leaks into
renal tubules
Hematuria (isomorphic)
Bacteria
accumulate
in the static
urine
Dysfunctional
proximal tubules
Unknown
mechanisms à
¯ urine citrate
àmore urine
Ca2+ binds to
oxalate than to
citrate à↑ Ca-
Oxalate stones
Note: PKD1 mutations have
more severe prognosis than
PKD2 mutations (earlier
disease onset, larger cysts)
Vessels
tear
more
easily
Stretches
renal
capsule
Cysts compress renal vasculature
¯ Glomerular perfusion
To ↑ perfusion à
kidneys activate RAAS
Hypertension")
Rickets and Osteomalacia: Pathogenesis and Clinical Findings

Shear forces
bend the
osteopenic
bone
Short stature
Diffuse skeletal pain
(bone tenderness)
Osteopenia
reduces bone
density and
cause fractures
with minimal
force applied
If hypophosphatemic,
production of ATP and
other high energy
molecules declines
Unequally
distributed
forces and
muscle/tendon
tension
stimulate
nociceptors
Legend: Published November 26, 2012 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Calcification inhibitors
(excess exposure to Al,
Fluoride, etidronate)
Lack, or reduced
function, of
mineralization
enzymes (like ALP)
Lack of bone mineral components:
1. Phosphate: renal tubule disorders, vit D
or Phosphate deficiency, ↑FGF23
2. Calcium: severe deficiency (infants)
Rickets: Occurs before
epiphyseal closure
Epiphyseal
plates do not
fuse, impairing
bone growth
Bowed legs
Cartilage in epiphyseal
plates cannot become
ossified
Disruption in
calcium ion
homeostasis
↓ GI
absorption of
Ca2+ into
blood
↓ Kidney
reabsorption
of Ca2+ into
blood
↓ energy available
to muscle
Author:
Payam Pournazari
Reviewers:
Yan Yu
Spencer Montgomery
David Hanley*
* MD at time of
publication")
Polyarteritis Nodosa (PAN): Pathogenesis and Clinical Findings
: Pathogenesis and clinical findings
Environmental triggers
Infectious/viral agents (commonly Hepatitis B)
Medical Comorbidities Malignancies (most commonly hairy-cell leukemia)
Immunogenetic Predisposition: patient is genetically predisposed to a dysregulated immune response
Fever
↑ ESR and CRP
Postulate 1
Viral antigen-antibody complexes deposit in vasculature, causing lesions and activating cellular inflammatory response
Authors: Nela Cosic, Yan Yu* Reviewers: Sean Doherty Martin Atkinson*
* MD at time of publication
Palpable or necrotic purpura
Malignant Hypertension
Renal Insufficiency
Myocardial ischemia
Heart failure Diffuse myalgias
Postulate 2
Viral replication causes direct injury to vascular endothelial cells
↑ Anti- endothelial cell autoantibodies (AECA)
Altered cytokine profile (↑TNF-α, IL-1β, IFN-α, IL- 2)à↑ T-cell mediated immune response
Weight metabolism Loss
Autoimmune attack on various areas of the body
Malaise and/or Arthralgias (knees, ankles, elbows, wrists)
Orchitis: Testicular pain, erythema and/or swelling
Small intestine perforation GI Manifestations
Non-specific abdo pain
GI hemorrhage
Peripheral sensory changes: Distal mononeuropathy
multiplex
Polyarteritis Nodosa (PAN)
Focal segmental necrotizing leukocytoclastic vasculitis of medium or small-sized arteries
Inflammation of arteries damages the vascular endothelium of those arteries
Inflammation predisposes formation of arterial thromboses
Blockage of arteriesà tissue ischemia and possible necrosis (tissue cell death)
↑ basal
Arterial aneurysms
Inflamed subcutaneous arteries
Inflamed renal artery
àluminal narrowing and reduced blood flow to kidneys
Inflamed coronary artery à luminal narrowing, occlusion, thromboses
Segmental inflammation of muscular arteries, stimulating surrounding nociceptors. Muscle ischemia develops long-term.
Ischemia/necrosis of the testicles
Ischemia/necrosis of the small intestine
Ischemic vasculitic nerve damage: Immune complex deposition within vessel walls of arteries traveling with nerves leads to persistent vascular inflammation and ischemia of associated nerve
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 18, 2019 on www.thecalgaryguide.com")
Secondary Polycythemia

Poor lung function
Renal artery stenosis
↓ blood flow to kidney
Kidney senses ↓ O2
High affinity Hb or CO poisoning
Hb does not easily unload O2
Tissues become hypoxic
Tumors (e.g. renal, hepatic, lung)
Secretes EPO in an unregulated way, as a “paraneoplastic syndrome”
High altitude
Obstructive sleep apnea
Episodic airway obstruction during sleep
Intermittent hypoxia
Cyanotic heart disease
Shunting of blood
Venous and arterial blood mixes
Poorly oxygenated blood
↓ O2 partial pressure
↑ EPO production independent of O2 (inappropriate response)
↑ EPO production due to hypoxia (appropriate response)
Abbreviations:
• Hb- Hemoglobin
• EPO- Erythropoietin • ILD- Interstitial Lung
Disease
• COPD- Chronic
Obstructive Pulmonary Disease
“Endogenous causes” of high EPO
Secondary Polycythemia
“Exogenous causes” of high EPO
Testosterone therapy Iatrogenic EPO (results in ↑ EPO synthesis administration
within the body)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
Appendicitis

The appendix is anatomically located in the RLQ; appendicitis may be confused with disorders of surrounding structures: Gynecological Diseases
• RuleoutpregnancywithHCG pregnancy test
• Rupturedovariancyst
• Ectopicpregnancy
• Mittelschmerz(mid-cycle
pain)
Gastro-intestinal Diseases
• Meckel’sdiverticulum (presents identically to appendicitis; surgically located 2 feet from ileocecal valve; mostly seen in children)
• Diverticulitis(presentsasleft sided appendicitis)
Non-GI Abdominal Issues
• Mesentericadenitisinkids <15: swollen mesenteric lymph nodes
• Renalcolic
Obstruction of appendiceal lumen (by fecalith, fibrosis, neoplasia, foreign bodies or lymph nodes in kids)
Appendix distension and spasms
↑ lumen pressure, ↓ blood flow to appendix
Ischemia, tissue necrosis, loss of appendix structural integrity
Bacterial invasion of the appendix wall, causing transmural inflammationandnecrosis
Stretching of visceral peritoneum, stimulation of autonomic nerves T9-T10
Progression of inflammation over several days (variable length of time)
Irritation of parietal peritoneum, stimulation of somaticnerves
If appendix not surgically removed
Perforation of colon wall, causing peritonitis, abscesses or death
Note: Symptoms hugely variable. Only 30% present with classic history. Diagnosis is mostly clinical. Further investigations:
CBC: Leukocytosis (due to inflammatory response) CT: Gold standard test. Thickened visceral membrane with enhancing (white) rim due to ↑ blood flow
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Diverticulosis and Angiodysplasia

Angiodysplasia
Autoimmune Diseases
Unclear Mechanisms
These patients tend to have “arterial-venous malformations” that rise up to the mucosa of the lower GI tract
Irritation of these malformations leads to bleeding into the GI tract lumen
Lower GI bleed
(occult, slow, asymptomatic, large- volume blood loss, usually associated with iron deficiency anemia)
Renal Failure
Older Age
Gradual expansion over
time thins the diverticular wall
Capillaries within diverticuli burst and leak blood into the colon lumen
Lower GI bleed
(usually stops by itself)
Colon wall forms little outpouchings (diverticuli)
Stretching of colonic serosa stimulates
somatic sensory nerves innervating the colon
Bloating, cramping
(But most often PAINLESS)
Trapping of feces in the colonic diverticuli
Bacteria have more time to metabolize the undigested materials, producing gas
Flautulence
Irregular defecation
Both conditions share similar features:
• Both are common, and their prevalence increases with age
• Are relatively benign and most are easy to treat (80% stop w/o intervention)
• Both present without pain in a previously-well patient
• Together, account for 50-80% of lower GI bleeds (diverticulosis > angiodysplasia)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published August 4, 2019 on www.thecalgaryguide.com")
iga-vasculitis-henoch-scholein-purpura-pathogenesis-and-clinical-findings
 : Pathogenesis and clinical findings
Authors: Mia Koegler Nela Cosic Reviewers: Crystal Liu Yan Yu* Martin Atkinson* * MD at time of publication
Infectious Agents
50% have preceding upper respiratory tract infections, i.e., influenza virus or Group A Strep
Drugs
I.e., antibiotics (penicillin, erythromycin), NSAIDs and biologics (tumor necrosis factor α inhibitors)
Immunogenetic and cellular predisposition
Various genetic polymorphisms alter cell- mediated immune response, IgA levels elevated in 50% of people
↑ Circulating galactose-deficient IgA1 (GD-IgA1). Deficiency in galactosylation of IgAà↓ IgA serum clearanceàadhesion of IgA complexes, which then deposit into the endothelial lining of blood vesselsàattraction of various inflammatory cells to the area:
Formation of Secretion of Interleukin 8 (IL8) - cytokine that induces Neutrophils infiltrate Activation of complement immune complexes neutrophilic chemotaxis and macrophage phagocytosis the tissue site factors (C3, C4)
Leukocytoclastic vasculitis (histopathologic term for small vessels inflamed by neutrophilic autoimmune response)
Inflamed cutaneous vessels become enlarged in clusters
Symmetrical palpable purpura (red/purple, non- blanchable papules) distributed on lower limbs and buttocks areas
Cutaneous small vessel vasculitis (100%)
Inflamed gastric vessels - hemorrhage and edema within bowel wall
Gastrointestinal (85%)
Colicky abdominal pain (commonly in the periumbilical region), nausea, vomiting
Gastrointestinal
GI bleeding (hematemesis, melena), Intussusception
Glomerular mesangial proliferation and inflammation
↑ mast cell deposition in joints
Joints (60-85%)
Arthralgia's (common), arthritis (especially knees and ankles)
Arthralgia often transient. No permanent sequelae
Sympathetic nervous system activation
Glomerulosclerosis, tubulointerstitial and podocyte damage
Renal tissue ischemia
↑ Na sensitivity in renal tubules (↑ Na and water retention)
Renal (10-50%)
Increased renin secretion
HTN, nephrotic/nephritic syndrome, renal insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 1, 2019 on www.thecalgaryguide.com")
Varicocele
.
• Small varicoceles can be identified by preforming the Valsalva maneuver (decreases venous return).
• Unilateral right varicoceles are uncommon and should be investigated for underlying pathology causing obstruction.
Primary
Anatomically: the left spermatic vein drains into the left renal vein
Nutcracker Effect: The left renal vein can get pinched by the abdominal aorta and superior mesenteric artery
Backup of blood in left renal vein ↑ pressure in left spermatic vein
Secondary
Renal cell carcinoma or retroperitoneal masses
Inferior vena cava thrombus
External compression of spermatic vein
Obstruction of blood flow
↑ spermatic vein pressure
Vein valve leaflet failure & retrograde bloodflow back towards testicle
Dilation of pampiniform plexus and scrotal vein plexus
Varicocele
↑ scrotal blood volume ↑ volume in a closed
space
↑ pressure and distension of scrotal layers
↑ scrotal vein plexus pressure
Compliant veins distend, becoming visible through scrotum
Blood heats up the structures it flows through
Scrotal hyperthermia
Unsuitable environment for spermatogenesis
Loss of germ cell mass
Bag of Worms Sign
Dull ache/heaviness
Decreased fertility Testicular atrophy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com")
Multiple-Myeloma
 immunoglobulins
Normal SPEP: no spike in the gamma (γ) region
Notes:
• MGUSismuchmorecommon than MM!
• “Plasmacell”:Blymphocytes that produce antibodies/ immunoglobulins
Stimulation by specific antigens
Genetic changes/mutations accumulate over time in one type of plasma cell
Abbreviations/Definitions: • SPEP - Serum Protein
Electrophoresis
• Ig – Immunoglobulin • Monoclonal – “of one
specific genetic strain or subtype”
One type of plasma cell starts to proliferate abnormally
Monoclonal Gammopathy of Undetermined Significance (MGUS) (Premalignant, mild monoclonal plasma cell proliferation; asymptomatic)
In 1-2% of cases, further cytogenetic changes over time stimulate further proliferation of this plasma cell line
Multiple Myeloma (MM)
(extensive monoclonal B lymphocyte proliferation, causing end organ damage)
Slightly more monoclonal plasma cells will produce slightly more monoclonal Immunoglobulins
Small spike in the gamma (γ) region of the SPEP (less prominent compared to the spike in MM)
More monoclonal plasma cells result in far greater amounts of monoclonal immunoglobulins being secreted
Large spike in gamma (γ) region of the SPEP
Ig light chains accumulate in the tubules of kidney nephrons
Light chain casts obstruct tubules
Renal Insufficiency (↓GFR)
Osteoblasts ↑ expression of RANK-ligand (RANKL, an apoptosis regulator), and ↓ expression of Osteoprotegerin (OPG, a decoy receptor for RANKL)
↑ osteoclast activity vs osteoblast activityàbone loss
Clonal plasma cells overrun normal bone marrow, crowding out production of red blood cells, ↓ red blood cell counts
Anemia
Authors: Tristan Jones, Tyler Anker, Yan Yu Reviewers: Jennifer Au, Crystal Liu, Man- Chiu Poon*, Lynn Savoie* * MD at time of publication
Damaged bones hurt, & become more brittle
Bony pain, pathologic fractures
Osteolytic bone lesions
Osteoclasts release calcium from bone and into blood
Hypercalcemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 12, 2020 on www.thecalgaryguide.com")
Diabetic-Nephropathy

↑ Intrarenal angiotensin II
↑ Advanced glycation end products (AGE)
Shunting of glucose through non- glycolytic pathways (e.g. polyol)
Activation of Protein Kinase C (PKC) pathway
Excessive production and accumulation of glycolytic intermediates (e.g. sorbitol, hexosamine, succinate)
hyperglycemia
Succinate via GPR91
↑ Free radical production (oxidative stress)
Activation of cellular signalling, transcription factors and cytokines (e.g. TGF-β-Smad-MAPK, IGF-1, NF-κB)
↑NADPH oxidase activity
↑Blood volume ↑ Blood pressure ↑ Renal perfusion
Relative afferent arteriole dilatation, efferent arteriole constriction
Initial ↑ in glomerular filtration rate (GFR)
Podocyte loss/injury
Authors: Steven Chen Shannon Gui Yan Yu* Reviewers: Julia Heighton Ryan Brenneis Sophia Chou* * MD at time of publication
Initial glomerular hyperfiltration at time of diagnosis
↓ Production of matrix metallo- proteinases
Aberrant extracellular matrix (ECM) protein expression and accumulation
Sheer stress to glomeruli à pressure-induced damage
↑ Glomerular basement membrane permeability to proteins like albumin
↓ Extracellular matrix regulation
“Metabolic Pathway”
Mesangial matrix expansion
Kimmelstiel-
Wilson lesions (pink
hyaline nodules due to accumulation of damaged proteins)
Tubular fibrosis
Scarred glomeruli are less able to effectively filter blood
↓ in glomerular filtration rate (GFR)
Albuminuria
Usually occurs after ~5 years from time of diagnosis in T1DM; can occur at time of diagnosis in T2DM
Abbreviations
IGF: Insulin-like growth factor
MAPK: Mitogen-activated protein kinases NADPH: Nicotinamide adenine dinucleotide phosphate
NF-κB: Nuclear factor kappa-light-chain- enhancer of activated B cells
TGF-β: Transforming growth factor-β
Protein endocytosis into tubular cells causing inflammation
“Hemodynamic Pathway”
Diabetic Nephropathy
Overt diabetic nephropathy may take upwards of 15-25 years to develop
Note: The mechanisms presented here have been simplified. The cross- talk and signaling between the metabolic and hemodynamic factors do not manifest in a step-wise fashion, but rather occur in parallel.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 3, 2020 on www.thecalgaryguide.com")
GU-changes-in-pregnancy

Mechanism unclear, possibly 1) ↑ circulating anti- angiogenic factorsà ↑ permeability of glomerular basement membrane, or 2) ↑ plasma volumeà↓ oncotic pressure of plasma at the glomerulus
Proteinuria
> 300 mg/day, abnormal in pregnancy
↑ hCG level
Dilation of renal vasculature
↑ renal vascular & interstitial volume
↑ filtration surface area
Overwhelming load of glucose to proximal tubule
↑ urine output
↑ relaxin secreted by placenta
Mechanism not well understood
↓ osmotic threshold for ADH release & thirst
↑ ADH secretion & ↑ oral hydration
Incomplete reabsorption of glucose
Glucosuria
Encourage bacterial growth in the urine
Urinary tract infection (e.g. cystitis, pyelonephritis)
↑ serum progesterone
Uterine rotation as uterus enlarge due to presence of large bowel
Ureter compression (R > L)
Ureterovesical reflux (back-flow of urine into the ureters/kidneys)
Dilatation of ureters (R > L) (hydroureter) & renal pelvis (hydronephrosis)
Progesterone competes with aldosterone
↓ sodium reabsorption
↓ plasma sodium concentration
Hyponatremia of pregnancy* (pathological if < 130 mEq/L)
*Despite factors favoring sodium excretion, there is a net retention of sodium during pregnancy from adaptation of the renal tubules
↑ urinary stasis
↑ excretion of creatinine and urea in urine
↓ serum creatinine and urea
↓ ureteral toneà ↑potential for ureter dilation
Mechanism not well understood
↓ peristalsis of ureters
↑ urinary frequency (voiding > 7x/day)
↑ nocturia (voiding ≥ 2x/night)
↓ oncotic pressure of plasma intra-vascularly àwater leaves blood, enters interstitial tissue, and stays there in gravity-dependent regions of the body
Pedal +/- ankle edema
Author: Simonne Horwitz Reviewers: Claire Lothian, Crystal Liu, Ronald Cusano*, Candace O’Quinn*, Yan Yu* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 28, 2020 on www.thecalgaryguide.com")
acute-pancreatitis-complications
:
Interstitial edematous pancreatitis
Local accumulation of fluid in the pancreas
<2 weeks after onset
Acute peripancreatic fluid collection (not encapsulated)
Walled off by fibrous & granulation tissue
>2 weeks after onset
Pancreatic pseudocyst
(completely encapsulated)
Peritoneal irritation à pain
Large cyst can (very rarely) compress surrounding bowel
Acute Pancreatitis
Inflammatory cytokines are released from damaged pancreas
If recurrentàchronic pancreatitis (see relevant slide)
Inflammation damages pancreatic exocrine
cellsàInappropriate release of pancreatic enzymes into surrounding tissue & vasculature àdigesting pancreatic parenchyma
Authors: Nissi Wei, *Yan Yu Reviewers: Dean Percy, Miles Mannas, Varun Suresh, Brandon Hisey, *Kerri Novak, *Sylvain Coderre * MD at time of publication
complete resolution (most cases)
Necrotic tissue is vulnerable to
infection (esp. Gram neg GI bacteria)
inflammation & necrosis activate cytokine cascade
Severe, necrosis (15%): Necrotizing pancreatitis
Local infection
Severe pancreatic inflammation shifts body fluid into retroperitoneal spaceàintravascular volume depletion
Systemic Inflammatory Response Syndrome (SIRS) (see relevant slide)
Organ failure (may be sole feature on presentation)
Stagnant fluid can more easily become infected
Infection spreads to bloodstream
Cardiac failure Hypovolemic shock Renal failure
Local accumulation of fluid & necrosis in the pancreas
< 4 weeks after onset:
Acute necrotic collection (not encapsulated)
Walled off by fibrous & granulation tissue
> 4 weeks after onset
walled-off necrosis
(completely encapsulated)
When treated with excess fluid resuscitation:
Intra- abdominal hypertension
Respiratory failure (ARDS)
Disseminated intravascular coagulation (DIC)
Bowel obstruction Gastric outlet (see relevant slide) obstruction
Infected pancreatic necrosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 20, 2016, updated September 7, 2020 on www.thecalgaryguide.com")
insuffisance-cardiaque-gauche-les-resultats-de-lexamen-physique

Dysfonction systolique
̄ Perfusion tissulaire (au niveau cerebral, renal etc.)
Vasoconstriction périphérique àdetournement limité du volume d’ejection systolique vers les organes principaux
Extrémités froides, cyanose périphérique
̄ Du débit urinaire
̄ De l’état de conscience
Hypoxie tissulaire la respiration anaérobique, production d’acide lactique (acidose)
Les centres respiratoires tentent de compenser
Expulsion des fluides des capillaires vers les alvéolesà oedème pulmonaire transudatif
La congestion vasculaire et les alvéoles oedématiées compriment les voies respiratoires, provoquant une turbulence du flux d'air
Un flux d'air turbulent est entendu lors de l'auscultation
Respiration sifflante (wheezing)
Flux turbulent dans le ventricule gauche distendu au début de la diastole
B3
Choc
de la pointe diffuse
̄ Du flux sanguin artériel pendant la systole
̄ Tension artérielle en systole
De la
tension artérielle lors de la diastole
̄ Pouls cardiaque
Fermeture des valves pulmonaires avec une force supérieure à la normale
B2 pulmonaire
̄ De l’oxygenation sanguine
Le transsudat obstrue les petites voies aériennes et alvéolaires
Si le ventricule gauche est en surcharge de pression ou si hypertrophié (i.e. sténose aortique, hypertension sévère)
Choc de la pointe soutenue
De l'activité du système sympathique (pour tenter de rétablir le débit cardiaque)
Pendant l'inspiration, de petites zones de compartiments aériennes s'ouvrent
Crépitements pulmonaires
(ils sont généralement bilatéraux et surtout au niveau de la base pulmonaire)
Auteur: Yan Yu
Editeurs: Sean Spence, Jason Baserman, Nanette Alvarez*
Traductrice/Traducteur:
Emma Hofland-Burry, Jean-François Lemay* *MD au moment de la publication
Activité des glandes sudoripares
Diaphorèse
Activité cardiaque
Tachycardie
Fréquence respiratoire
Tachypnée
Remarque: l'insuffisance cardiaque gauche étant la cause principale de l'insuffisance cardiaque droite, elle peut également se présenter par des signes d'insuffisance cardiaque droite. Les autres caractéristiques de l'insuffisance cardiaque gauche dépendent de la cause sous-jacente.
Si la pression vasculaire artérielle pulmonaire est chroniquement élevéeàporvequera un surmenage prolongé de la function du ventricule droit:
Insuffisance cardiaque droite: Le patient présente des conséquences directes de sa congestion veineuse systémique: œdème
périphérique (i.e.cheville), épanchements pleuraux, congestion hépatique/ascites (s.v.p. voir la diapositive correspondante)
Publié le 10 Janvier 2013 à www.thecalgaryguide.com")
Pathogenesis-of-Female-Infertility
 from hypothalamus
↓ release of Luteinizing hormone (LH) & Follicle stimulating hormone (FSH) by pituitary
↓ release of estrogen by ovaries
Anovulation (oocyte is not released)
Fewer follicles available to ovulate
* Causes of Hyperprolactinemia include: prolactinoma (prolactin-producing tumor), hypothalamic infiltrate or mass, chest wall irritation, hypothyroidism, renal or liver disease (↓ prolactin clearance), dopamine antagonists that ↑ prolactin secretion (antipsychotics, anti- depressants, anti-emetics)
Polycystic ovary syndrome (see PCOS: Pathogenesis and Clinical findings)
↑ androgen production & ↑ estrogen earlier in the menstrual cycle
↓ FSHà↓ follicle growth
↑ rate of follicle depletion
Oocyte not available every month for fertilization
Premature ovarian insufficiency due to unexplained causes, chemotherapy, radiation, autoimmune ovarian destruction, Turner’s & Fragile X Syndromes
Damage in germ cells that accumulates over a woman’s lifetime
Age-related changes in quality of granulosa cells surrounding oocyte
Genetic damage accumulates, such as ↑ rates of meiotic nondisjunction (failure of chromosomes to separate during gamete cell division)
Tubal occlusion or ↓ transport of oocyte tubal cilia dysfunction through fallopian tube
↓ quality of oocytes
Normal transport of oocyte & sperm through fallopian tube is impaired
↓ facilitation of sperm transportation
Inhibits normal zygote implantation
Chlamydial or gonorrhoeal pathogens
Previous tubal surgery or ectopic pregnancy surgery tissue removal ↓ transport of oocyte through fallopian tube
Female Infertility
Previous abdominal infection or surgery Endometriosis
Congenital malformations or trauma / surgery to cervix
Uterine leiomyomata (benign smooth muscle monoclonal tumor) or polyp
Intrauterine procedures
Pelvic adhesions (scar-like tissue that tether together abdominal organs) may distort the shape and normal anatomy of the fallopian tube
Ectopic endometrial cells implant & Local inflammatory response grow along pathway of egg/sperm further ↓ egg/sperm mobility
Inability of cervix to produce normal mucus, and/or sperm physically unable to enter the cervix
Submucosal or intracavitary component disrupts uterine lining
Trauma to basalis layer of endometrium
Intrauterine scarring or synechiae (adhesions)
↓ vascularization & endometrial regrowth
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 25, 2020 on www.thecalgaryguide.com")
Tumour-Lysis-Syndrome

Though rare, aggressive tumours can spontaneously lyse without treatment
Intracellular potassium released into bloodstream
Intracellular phosphate released
Hyperphosphatemia
↑ serum phosphate
Intracellular lactate dehydrogenase (LDH) released
↑ serum LDH
Intracellular nucleic acids released
Nucleic acids metabolized to uric acid
Hyperuricemia
↑ serum uric acid
Hyperkalemia
↑ serum potassium
(see Hyperkalemia: clinical findings)
Uric acid (a crystallizing substance) ↑ precipitation of calcium phosphate
↑ filtration of poorly soluble uric acid into acidic environment of renal tubules
Serum phosphate binds serum calcium, forming solid calcium phosphate precipitate crystals
High levels of calcium phosphate ↑ uric acid precipitation
Uric acid precipitates as crystals and deposits in kidney tubules and collecting ducts
Tubular injury and/or intraluminal obstruction
Endothelial dysfunction in renal vasculature
Renal inflammation, vasoconstriction, and
impaired renal vascular autoregulation
Decreased renal filtration
Acute Kidney Injury
(see Acute Kidney Injury Overview)
Crystal deposition in the heart
Depletion of soluble calcium
Hypocalcemia
Calcium phosphate crystals deposit in kidneys
Main mechanism of Acute Kidney Injury
Cardiac Arrythmias
↓ serum calcium
(see Hypocalcemia: clinical findings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 25, 2020 on www.thecalgaryguide.com")
Primary-Aldosteronism

↑ Serum aldosterone level
↑ Circulating aldosterone activates mineralocorticoid receptors on cardiac myocytes
↑ Transcription of proinflammatory and profibrotic genes in cardiac myocytes
Cardiac fibrosis and hypertrophy
In the rest of the body, K+ moves from intracellular to extracellular environment (down it's concentration gradient) to compensate for decreased serum K+
Loss of positively charged K+ànegative intracellular chargeàcells take up H+ to remain electrostatically neutral
↑ Expression of epithelial sodium channels in
principal cells of cortical collecting duct
↑ Na+ reabsorption from cortical collecting duct into blood vessels
+ Water follows Na
into the blood vessels to balance the osmotic pressure between the blood and the renal tubules
↑ blood volume within the volume-
constrained space of blood vessels
↑ Activation of Na+/K+ ATPase in principle cells of cortical collecting duct
Removal of positively charged Na+ from tubular lumenà lumen becomes electronegative versus the interstitial space & inside tubular epithelial cells
Positively charged K+ follows the electrical gradient and is secreted into tubular lumen
↓ Serum K+ concentration
↑ Expression of H+ ATPase in the apical (luminal)
membrane of intercalated cell of cortical collecting duct
H+ is secreted into cortical collecting duct → renal loss of H+ from the body
Metabolic Alkalosis
(blood becomes more basic; ↑ serum pH)
Hypertension
Muscle weakness, fatigue, polyuria
↓ pH in intercalated cell
↓ pH in cells of proximal convoluted tubule
↑ loss of H+ through kidneys
H+ secretion into cortical collecting duct
↑ H+ ATPase activity in intercalated cell
Activation of glutaminase in proximal convoluted tubule
HCO3- pumped into blood
↑ production of HCO3- (product of glutamine breakdown)
↑ breakdown of glutamine
Hypokalemia
(See Hypokalemia: Clinical Findings slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 16, 2020 on www.thecalgaryguide.com")
Beta-Blockers-Mechanism-of-Action-and-Side-Effects
 to these receptors, ↓ their normal adrenergic tone
Beta-2 receptor antagonism Beta-1 receptor antagonism
Lungs Eyes Central nervous system Heart Kidneys ↓ cAMP (intracellular messenger) productionàcomplex, tissue-specific intracellular mechanisms resulting in a variety of effects in different tissues:
Throughout body tissue
Epinephrine (via cAMP) indirectly ↑ the activity of the Na+/K+ pump on cell membranes (a pump that moves 3 Na+ out of cells per 2 K+ moved into cells)
Blocking epinephrine from binding
the beta-2 receptor and producing cAMPà↓ activity of Na+/K+ pump à↓K+ moved into cells
↑ proportion of K+ now resides in extracellular fluid, detectable in serum (total body K+ remains the same)
Hyperkalemia (see Calgary Guide: Hyperkalemia – Clinical findings)
Blocking sympathetic hormonesà↓ relaxation of smooth muscle circumferentially wrapped around airways
↑ resting airway muscle toneà bronchoconstriction
↑ resistance to airflow
Wheezing, dyspnea, chest tightness
Exacerbation of underlying airway disease (e.g. asthma)
↓ ciliary epithelium’s production of aqueous humor (fluid that fills anterior chamber of the eye)
Reduced intraocular pressure
Blocking adrenergic response mediated by epinephrine and norepinephrine (e.g. the physiologic “fight- or-flight” response to stress)
↓ tremor, irritability, anxiety
↓ ability to produce adrenergic symptoms in response to hypoglycemia
Hypoglycemia unawareness
Coronary perfusion pressure = diastolic blood pressure in aorta – LV end diastolic pressure
↓ inotropy (contractility of cardiac muscle)
↓ chronotropy (heart rate and conduction velocity)
↓ renin releaseà↓ creation of angiotensin II & aldosterone
+ ↓ reabsorption of Na
and H2O in nephron
↑ urinary Na+ & H2O loss
↓ total blood volume
Decompensation of acute heart failure
Dizziness and fatigue Hypotension (Blood pressure = cardiac
output x systemic vascular resistance)
↓ O2 demand of myocardial tissue
Bradycardia
Inability to ↑ heart rate in response to stress (e.g. shock, sepsis)
↓ stroke volume
↓ cardiac output
Beta blockers ↓ diastolic blood pressure, & thus may ↓ coronary perfusion pressure
Before giving beta blockers, ensure blood pressure isn’t too low
Otherwise, may worsen acute myocardial ischemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 14, 2021, updated Feb 7, 2021 on www.thecalgaryguide.com")
Potassium-Sparing-Diuretics-Mechanism-of-Action-and-Side-Effects
 Inhibit Na+ channels (involved in Na+ reabsorption) in the luminal membrane of the principal cells in the cortical collecting duct
Aldosterone Antagonists (Spironolactone and Eplerenone) Competitively blocks mineralocorticoid receptors and ↓ aldosterone effect in the renal tubules and throughout the body
↓ aldosterone effectà↓ expression of basolateral Na+/K+ pumps & luminal epithelium Na+ channels on the principal cells of cortical collecting duct
Spironolactone’s molecular structure is similar to that of steroid
hormonesàspironolactone can also block androgen receptors
Anti-androgenic effects
(due to ↓ androgen function in reproductive organs, skin, and on brain centers)
Triamterene can form triamterene crystals
and granular casts (unclear mechanism)
↓ Na+ reabsorption by principal cells
↓ in serum Na+ concentration: Hyponatremia
↓ K+ pumped out into the tubule by principal cells
Crystals & casts obstruct tubular lumen → inflammation (unclear mechanism)
Triamterene crystals are
directly cytotoxic to tubular cells
Only ~2-5% of Na+ filtered by the glomerulus is normally reabsorbed in the
cortical collecting ductàthe ↑ in Na+ retained in cortical collecting duct is mild
Water follows Na+ to maintain a balanced osmotic pressureà↑ in water in cortical collecting duct available for excretion
↑ positive charges in lumen relative to surroundings generates an electropositive tubular lumen
Unfavorable electrical gradient ↓ secretion of positive charged ions into electropositive lumen
↓ libido
Menstrual abnormalities (in women)
↓ acne Gynecomastia
(in men)
↓ secretion of K+
↑ in serum K+ concentration:
Hyperkalemia
Cardiac Arrythmias (See relevant slide on Hyperkalemia: Clinical Findings)
Interstitial inflammation and tubular injury
Drug-induced Nephrotoxicity
Mild Diuresis
↓ blood volume
↓ Blood pressure/ Hypotension
↓ secretion of H+
↑ in serum H+ concentration:
Metabolic Acidosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 15, 2021 on www.thecalgaryguide.com")
AAA-Pathogenesis
: Pathogenesis
Different parts of the aorta have different embryologic origins
Atherosclerosis
Hypertension
Age > 65
Progressive deterioration of aorta structural integrity over life span
Connective Tissue Disease
Structurally abnormal protein or protein organization in aorta
Autoimmunity
Infection (e.g Chlamydia, Mycoplasma pneumoniae, Helicobacter pylori, human cytomegalovirus, herpes simplex virus)
Antigens (substance that causes immune response) on virus or bacteria resemble local proteins in abdominal aorta
Antibodies produced in response to infection inappropriately target host cells in the aorta
Antibodies tag cells in the abdominal aorta for destruction by T-lymphocytes
Immune-mediated destruction of aorta
Smoking
Genetics
Unclear mechanisms
Subacute (not clinically detectable) inflammation of aortic tissue
Inflammatory cytokines are released and immune cells are recruited
↑ pressure on aorta and other vessel walls
Infiltration of vessel wall by lymphocytes and macrophages
Production of enzymes that break down elastin & collagen proteins (which provide most tensile strength to aorta)
Aorta susceptible to damage
Degradation of aortic connective tissue
Biomechanical stress on vessels
Authors: Olivia Genereux Davis Maclean Reviewers: Jason Waechter* Amy Bromley* Yan Yu* *MD at time of publication
The exact mechanisms are complex, debatable, and an area of intensive research – the 3 mechanisms and associated pathophysiology presented here are generally thought to be the main causes of abdominal aortic aneurysms
Infrarenal aorta has poorly developed vaso vasorum (dedicated blood supply to vessel wall)
Infrarenal aorta relies solely on nutrient diffusion from aortic blood that crosses abdominal aorta
Infrarenal aortic wall has fewer “lamellar” units (fibromuscular units) than other regions of the aorta
Infrarenal aorta is less elastic & less able to distribute stress
Loss of smooth muscle cells & thinning of tunica media
Destruction of elastin in tunica media
Normal layers of the aortic wall
↓ aortic tensile strength (ability to withstand stretching) Aorta expands and dilates due to internal pressure
Tunica Intima (inner-most tissue layer of aorta)
Tunica Media (layers of elastic
tissue (elastin) and muscle fibers)
Adventitia (thin outermost collagenous layer)
(longitudinal section)
Aortic aneurysms are usually infrarenal (85%)
Abdominal Aortic Aneurysm
Infrarenal aorta more prone to ischemia and has impaired repair potential
Abnormal, irreversible dilation of a focal area of abdominal aorta (area of aorta between diaphragm & aortic bifurcation) to twice the diameter of adjacent normal artery segment
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published February 27, 2021 on www.thecalgaryguide.com")
VITT
: Pathogenesis and Clinical Findings
Current leading theory: COVID-19 viral vector vaccines (Johnson and Johnson and AstraZeneca) contain an anionic molecule (currently unspecified), which binds to the cationic platelet factor 4 (PF4) molecule in the bloodstream, forming vaccine/PF4 complexes
Authors: Brooke Fallis Reviewers: Yan Yu* Katie Lin* * MD at time of publication
Spleen macrophages remove antibody/platelet complexes from circulation
Fewer unbound platelets in circulation detected on complete blood count (CBC)
Thrombocytopenia: Platelets <150x!")
disseminated-intravascular-coagulation
: Pathogenesis and clinical findings
Authors: Emily Wildman Mehul Gupta Sean Spence Yan Yu* Reviewers: Kiera Pajunen Wendy Yao Tristan Jones Man-Chiu Poon* Lynn Savoie* * MD at time of publication
Sepsis
Microorganisms express pathogen- associated molecular patterns (PAMPs)
Severe Trauma
Damaged endothelial cells release damage- associated molecular patterns (DAMPs)
Solid and Hematologic Malignancies
Cancer cells express tissue factor and release procoagulants
Immune cells recognize DAMPs and PAMPs and begin expressing tissue factor and releasing procoagulants
Systemic activation of coagulation cascade
Activation of coagulation cascade results in the factor X mediated conversion of large quantities of prothrombin (factor II) to its active form, thrombin (factor IIa)
Thrombin cleaves fibrinogen (factor I) circulating in blood to an activate form known as fibrin (factor 1a)
↓ Serum fibrinogen
Diffuse coagulation causes imbalances between coagulation and anticoagulation pathways
Consumption of coagulation factors (including platelets, fibrinogen, prothrombin, factor V, factor VIII) exceeds rate of production
Fibrin, in conjunction with platelets, form widespread thrombi within vasculature
Fibrin thrombi accumulate in the microvasculature and shear transiting red blood cells
Microangiopathic hemolytic anemia (MAHA)
↑ thrombi formation ↑ fibrinolysis, a parallel process that naturally degrades fibrin thrombi
Relative deficiency of coagulation factors leads to a bleeding diathesis (tendency to bleed) despite widespread clots
↑ Prothrombin time (PT)
↑ Partial thromboplastin time (PTT)
↑ D-dimer Fibrin thrombi
↑ Fibrin degradation products
Platelets are used up forming thrombià less free platelets in circulation
↓ Platelets on Complete Blood Count
accumulate in microvasculature of major organs
Deposition of thrombi occlude blood flow resulting in ischemia of organ parenchyma
Lack of coagulation factors can predispose spontaneous hemorrhage in various organs
Multiple organ dysfunction syndrome (MODS) - (renal failure, hepatic dysfunction, stroke, pulmonary disease)
Clinical manifestations of bleeding, including petechiae (pinpoint red spots on skin), ecchymoses (bruising), weeping wound sites, bleeding mucous membranes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published Aug 7, 2012, updated July 27, 2019 & Aug 29, 2021 on www.thecalgaryguide.com")
Primary-Adrenal-Insufficiency

Note: “Primary” refers to pathology in the gland that produces the functional hormone (in this case, the adrenal gland), as opposed to “secondary” or “tertiary” which refers to pathology in glands that indirectly control the primary gland.
Bilateral adrenal Autoimmune damage (cancer,
↓ Androgen levels in women (in whom adrenal glands are the primary source)
↓ Libido
↓ Axillary and pubic hair
Muscle/joint pain
Anorexia, weight loss
Abdominal pain, nausea, vomiting
Diseases bleeding, etc)
↓ Androgen production from the zona reticularis
↓ Cortisol production from the zona fasciculata
↓ Serum cortisol
Patients could present with many severe symptoms of
adrenal insufficiency, e.g. low blood pressure refractory to fluid resuscitation
Significant bilateral damage to the adrenal glands
Entire adrenal cortex function impaired
↓ Serum levels of adrenal steroid hormones exert positive feedback effect on pituitary gland, ↑ pituitary gland’s production of adrenocorticotropic hormone (ACTH)
↑ Serum levels of ACTH
The same gene that encodes ACTH also encodes melanocyte stimulating hormone (MSH)
Coincidental ↑ in MSH production by the pituitary
↓ Serum DHEAS, testosterone and androstenedione
Unknown mechanism(s)
Malaise
Adrenal Crisis
↓ Cortisol mediated gluconeogenesis and glycogenolysis
↑ Cortisol Releasing Hormone (CRH) from the hypothalamus
Lack of cortisol-driven vasoconstriction of blood vesselsà↑ Vasodilation
↓ Blood pressure, postural dizziness
Water follows sodiumà ↑ excretion of water
↓ Sodium resorbed from kidney tubulesà↑ Sodium excretion
↓ Potassium pumped into kidney tubules à↑ potassium retained in serum
Hypoglycemia (↓ blood glucose)
↑↑ Antidiuretic hormone (ADH) release
Kidneys reabsorb water à↑ total body water
Hyponatremia (↓ serum sodium)
↑ Salt craving
Hyperkalemia (high serum potassium level)
↓ Aldosterone production from the zona glomerulosa
↓ Serum aldosterone
MSH triggers ↑ production of melanin by the melanocytes in skin
↓ Excretion of hydrogen ions from kidneys (See type IV RTA slide for full mechanism)
Metabolic acidosis (low pH, low bicarbonate)
↓ Sodium channel and Na/K ATPase
expression on principle cells of the kidney
Hyperpigmentation of the skin and mucosal surfaces
Authors: Jaye Platnich, Brooke Fallis, Yan Yu* Reviewers: Mark Elliott, Alexander Arnold, Hanan Bassyouni*, David Campbell* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 13, 2013, updated October 1, 2021 on www.thecalgaryguide.com")
Hypercortisolemia
: Clinical Findings
Cortisol is a net catabolic hormone affecting many body systems, serving to release energy into the blood in response to stress. Excess cortisol also impacts circulation and impairs immune function. Excess Serum Cortisol affects:
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Amanda Henderson, Brooke Fallis, David Campbell* * MD at time of publication
Bone and Calcium Metabolism
Kidney and vasculature
Excess cortisol in the renal tubule saturates the enzyme 11β- HSD2, which converts cortisol to cortisone
Capacity of body to convert cortisol to cortisone is exceeded
Excess cortisol can mimic aldosterone
and bind to mineralocorticoid receptors (cortisone can’t bind to these receptors)
↑ Aldosterone effect → ↑ Na+ reabsorption from the cortical collecting duct into blood vessels
Liver and Peripheral Tissue
Cortisol ↑ gluco- neogenesis in liver, and ↑ insulin resistance by body tissue (unclear mechanisms)
Hyper- glycemia
Reproductive System
Cortisol exerts negative feedback on hypothalamus
à↓ gonadotropin releasing hormone (GnRH) secretion
↓ GnRH → ↓ LH/FSH → ↓ estrogen and testosterone production (especially important in females)
Infertility, ↓ Libido, Irregular Menses
Adipose Tissue
Cortisol ↑ fat breakdown (lipolysis)
Selective expression of cortisol receptor on different adipose tissuesàcentral, facial, dorsal fat is less broken down than in other areas (mechanism unclear)
Combined with cortisol ↑ appetite:
Skin & Connective Tissue
↑ Serum cortisol à↓ Fibroblast proliferation → ↓ Collagen synthesis
Skin atrophy with loss of connective tissue
Muscle
↑ Proteolysis & ↓ Protein synthesisà↓ muscle growth and function
Immune System
Normal serum cortisol protects against damaging effects of uncontrolled inflammatory and immune responses
↑ Serum cortisolà over-suppression of inflammation and impaired cell- mediated immunity
↑ Serum cortisol leads to ↓ Intestinal Ca2+ absorption and ↓ renal Ca2+ reabsorption
↓ Serum Ca2+ ↑ PTH secretion
↑ Serum cortisolà↑ RANKL:OPG ratio
↓ Osteoblast activity & ↑ Osteoclast activity
Cardiac muscle
Cardio- myopathy, Heart Failure
Skeletal
muscle, especially upper arms & thighs (for unclear reasons)
Proximal Muscle Weakness
Easy Bruising
↑ abdominal size stretches the fragile skin to become thinneràvenous blood of the underlying dermis becomes visible
Purple Striae
If hypertension is chronic
Ca2+ resorption from bone into the blood
Osteoporosis
Supraclavicular & Dorsal Fat Pads
Central Obesity
Poor Wound Healing
Susceptibility to infection
Round Face (Moon Face)
Abbreviations:
• RANKL – Receptor activator of nuclear factor kappa-Β ligand • OPG – Osteoprotegerin
• 11β-HSD2 – 11β-hydroxysteroid dehydrogenase type 2
Water follows Na+ into blood vessels to balance the osmotic pressure between the blood and renal tubules
Water reabsorption → Expansion of blood volume
Hypertension
Both primary Cushing’s (e.g. adenomas that extend into zona reticularis of the adrenal cortex) and central/secondary Cushing’s (e.g. ↑ ACTH stimulation of zona reticularis) are associated with ↑ adrenal androgen secretion
Removal of positively charged Na+ from tubular lumen creates a negative luminal environment
K+ follows the electrical gradient and is secreted into tubular lumen
↓ Serum K+ concentration
Hypokalemia
Arrhythmia, Paralysis, Cramps
(see Hypokalemia: Clinical Findings slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 17, 2021 on www.thecalgaryguide.com
Hirsutism, Acne")
Diabetische Ketoazidose (DKA)

Betrifft hauptsächlich Patienten mit Diabetes Mellitus Typ 1: Bestimmte Situationen (z.B. Infektionen) erhöhen den Insulinbedarf, welcher durch fehlende Produktion/unzureichende Substitution nicht gedeckt werden kann
Autor: Yan Yu Rezensenten: Peter Vetere, Gill Goobie, Sean Spence, Hanan Bassyouni* Übersetzung: Sarah Schwarz Übersetzungsprüfung: Dr. Gesche Tallen * MD zum Zeitpunkt der Veröffentlichung
Hyperglykämie
(erhöhter Blutzucker)
Bei >12mmol/L, Glukosefiltration > - resorption, Glukose verbleibt im Urin
Glukosurie
Glukose ist osmotisch wirksam und zieht große Mengen Wasser mit sich (Osmotische Diurese)
Polyurie
Schwere Dehydrierung(bis zu 4-5L)
(ZVD↓, Orthostase: posturale Hypotension/ posturale Tachykardie, Ruhepuls ↑ )
Insulinmangel enthemmt die Lipolyse, sodass der Körper Energie aus Triglyceriden produziert
Freisetzung von freien Fettsäuren aus Fettgewebe
Absoluter
Insulinmangel
Hypothalamische Zellen induzieren bei geringem intrazellulären Glukosespiegel ein starkes Hungergefühl
Glukose bleibt im Blut & kann nicht durch Muskel- /Fettgewebe verstoffwechselt werden
“Ausgehungerte” Zellen triggern die Freisetzung kataboler Hormone: Glucagon, Katecholamine, Cortisol, Somatotropin
Damit intrazellulärer Glukosespiegel ↑, erhöht der Körper den Blutzucker
Hydrolyse von freien Fettsäure in
der Leber (Ketogenese) Polyphagie
↓ Proteinsynthese, ↑ Proteolyse (in Muskelgewebe)
↑ Gluconeogenese, ↑ Glykogenolyse (in der Leber)
Acetyl Co-A
Energiequelle für “ausgehungerte” Zellen
Beachte: Neben Glukose sind Ketonkörper die einzigen Energieträger die von Nervenzellen metabolisiert werden können. Deshalb werden sie vom Körper bei geringem Glukoseangebot produziert.
Ketonkörper
( β-Hydroxybutyrat, Acetoacetat, Aceton, akkumulieren im Blut)
Ketonurie
Metabolische Azidose
(↑Anionenlücke: Ketonkörper verbrauchen den HCO3--Puffer)
Substrate der Gluconeogenese↑
Durch ↓ Extrazellulärflüssigkeit, werden Ketonkörper konzentriert → Azidose
Stört das enterische Nervensystem, Magenentleerung ↓, Ileus
Bauchschmerzen, Übelkeit, Erbrechen
(Dehydration↑)
Abatmen von CO2 um Azidose auszugleichen
Kussmaul- Atmung (Tiefe, schnelle Züge)
Abatmen von Keton- körpern
Azeton- geruch der Atemluft
Beeinträchtigung elektrischer Signale zum Gehirn, Rücken- mark und Nervenzellen
Perfusion des Gehirns, Rückenmark, Nervenzellen↓
Verschiebung des Wasser- und Elektrolythaushalts
Falls Trinkwasser vorhanden
Polydipsie Beachte: Während der DKA verliert der Körper K+ durch
Elektrolytstörung
Schwäche, Delirium +/- Koma
osmotische Diurese und Erbrechen. Da gleichzeitig allerdings K+ aus den Zellen diffundiert, kann das Serumkalium unauffällig/erhöht sein. Um Hypokaliämien zu verhindern sollte bei K+ <5.0mmol/L KCl zusammen mit Insulin i.v. verabreicht werden. Cave: gute Nierenfunktion des Patienten
Therapie: 1) +++ Flüssigkeit. 2) Insulin + KCl. 3) Auffüllen der Anionenlücke. 4) Auslösende Faktoren identifizieren. 5) Wenig PO4 (typischerweise wenige Stunden bis einen Tag nach der Ketoazidose durch ↑ ATP-Produktion.)
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Publikationsdatum: 17 Juni 2013 auf www.thecalgaryguide.com
Hyperosmolares/ Hyperglykämisches Koma (HHS)
Beachte: betrifft nur Patienten mit Diabetes mellitus Typ II
Beachte: Es sollte stets nach auslösenden Faktoren z.B. einer Infektion gesucht werden
Autor: Yan Yu Rezensenten:
Peter Vetere
Gill Goobie
Hanan Bassyouni* Übersetzung:
Sarah Schwarz Übersetzungsprüfung: Dr. Gesche Tallen
* MD zum Zeitpunkt der Veröffentlichung
Verschiebung des Wasser- und Elektrolythaushalts
Elektrolytstörung
Unzureichende Insulin- produktion, Insulinresistenz, Nichtansprechen auf Insulintherapie
Relativer Insulinmangel
Situationen mit ↑Insulinbedarf: Infekt, Pneumonie, Herzinfarkt, Pancreatitis, etc.)
Hyperglykämie
(Stark erhöhter Blutzucker, höher als bei der DKA)
Bei >12mmol/L, Glukosefiltration > - resorption, Glukose verbleibt im Urin
Glukosurie
Glukose ist osmotisch wirksam und zieht große Mengen Wasser mit sich (Osmotische Diurese)
Polyurie Dehydration
(ZVD↓, Orthostase: posturale Hypotension/posturale Tachykardie, Ruhepuls ↑ )
Durch das wenige noch vorhandene Insulin, wird ein Teil der Glukose von Muskel- /Fettgewebe verstoffwechselt, ein Teil verbleibt im Blut
Körperzellen brauchen eine weitere Energiequelle
Freisetzung kataboler Hormone: Glucagon, Katecholamine, Cortisol, Somatrotropin
Damit intrazellulärer Glukosespiegel ↑, erhöht der Körper den Blutzucker
Hypothalamische Zellen induzieren bei geringem intrazellulären Glukosespiegel ein starkes Hungergefühl
Polyphagie
Beachte: Durch das wenige noch
vorhandene Insulin wird die Lipolyse gehemmt und werden keine Ketonkörper produziert. Es kommt nicht zur Azidose und Ketonurie (Gegensatz zur DKA). Sollte es doch zur Ketourie kommen, ist das meist Folge von Hungerzuständen oder anderen Mechanismen
Extrazellulärflüssigkeit ↓ mit erhöhter Osmolarität (z.B. Hypernatriämie)
↑ Gluconeogenese, ↑ Glykogenolyse (in der Leber)
↓ Proteinsynthese, ↑ Proteolyse (in Muskelgewebe)
Substrate der Gluconeogenese ↑
Sollte der Patient nicht ausreichend trinken um das Volumendefizit auszugleichen
Falls Trinkwasser vorhanden
Polydipsie
Wasser verlässt Zellen entlang des osmotischen Gradienten, Neuronen schrumpfen
Neuronaler Schaden: Delirium, Krampfanfall, Benommenheit, Koma
Renale Perfusion↓, GFR ↓
Nierenversagen
(prä-renal, siehe entsprechende Folie)
Beachte: Während der DKA verliert der Körper K+ durch osmotische Diurese. Da gleichzeitig allerdings K+ aus den Zellen diffundiert, kann das Serumkalium unauffällig/erhöht sein. Um Hypokaliämien zu verhindern sollte bei K+ <5.0mmol/L KCl zusammen mit Insulin i.v. verabreicht werden.
Cave: gute Nierenfunktion des Patienten
Beachte: Elektrolytstörungen (z.B. Hyperkaliämien, Hypernatriämien) verschlechtern sich bei akutem Nierenversagen, welches bei der DKA &HK häufig auftritt
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Veröffentlicht: 3. November 2016 auf www.thecalgaryguide.com")
Hyperosmolares/ Hyperglykämisches Koma (HHS)

Betrifft hauptsächlich Patienten mit Diabetes Mellitus Typ 1: Bestimmte Situationen (z.B. Infektionen) erhöhen den Insulinbedarf, welcher durch fehlende Produktion/unzureichende Substitution nicht gedeckt werden kann
Autor: Yan Yu Rezensenten: Peter Vetere, Gill Goobie, Sean Spence, Hanan Bassyouni* Übersetzung: Sarah Schwarz Übersetzungsprüfung: Dr. Gesche Tallen * MD zum Zeitpunkt der Veröffentlichung
Hyperglykämie
(erhöhter Blutzucker)
Bei >12mmol/L, Glukosefiltration > - resorption, Glukose verbleibt im Urin
Glukosurie
Glukose ist osmotisch wirksam und zieht große Mengen Wasser mit sich (Osmotische Diurese)
Polyurie
Schwere Dehydrierung(bis zu 4-5L)
(ZVD↓, Orthostase: posturale Hypotension/ posturale Tachykardie, Ruhepuls ↑ )
Insulinmangel enthemmt die Lipolyse, sodass der Körper Energie aus Triglyceriden produziert
Freisetzung von freien Fettsäuren aus Fettgewebe
Absoluter
Insulinmangel
Hypothalamische Zellen induzieren bei geringem intrazellulären Glukosespiegel ein starkes Hungergefühl
Glukose bleibt im Blut & kann nicht durch Muskel- /Fettgewebe verstoffwechselt werden
“Ausgehungerte” Zellen triggern die Freisetzung kataboler Hormone: Glucagon, Katecholamine, Cortisol, Somatotropin
Damit intrazellulärer Glukosespiegel ↑, erhöht der Körper den Blutzucker
Hydrolyse von freien Fettsäure in
der Leber (Ketogenese) Polyphagie
↓ Proteinsynthese, ↑ Proteolyse (in Muskelgewebe)
↑ Gluconeogenese, ↑ Glykogenolyse (in der Leber)
Acetyl Co-A
Energiequelle für “ausgehungerte” Zellen
Beachte: Neben Glukose sind Ketonkörper die einzigen Energieträger die von Nervenzellen metabolisiert werden können. Deshalb werden sie vom Körper bei geringem Glukoseangebot produziert.
Ketonkörper
( β-Hydroxybutyrat, Acetoacetat, Aceton, akkumulieren im Blut)
Ketonurie
Metabolische Azidose
(↑Anionenlücke: Ketonkörper verbrauchen den HCO3--Puffer)
Substrate der Gluconeogenese↑
Durch ↓ Extrazellulärflüssigkeit, werden Ketonkörper konzentriert → Azidose
Stört das enterische Nervensystem, Magenentleerung ↓, Ileus
Bauchschmerzen, Übelkeit, Erbrechen
(Dehydration↑)
Abatmen von CO2 um Azidose auszugleichen
Kussmaul- Atmung (Tiefe, schnelle Züge)
Abatmen von Keton- körpern
Azeton- geruch der Atemluft
Beeinträchtigung elektrischer Signale zum Gehirn, Rücken- mark und Nervenzellen
Perfusion des Gehirns, Rückenmark, Nervenzellen↓
Verschiebung des Wasser- und Elektrolythaushalts
Falls Trinkwasser vorhanden
Polydipsie Beachte: Während der DKA verliert der Körper K+ durch
Elektrolytstörung
Schwäche, Delirium +/- Koma
osmotische Diurese und Erbrechen. Da gleichzeitig allerdings K+ aus den Zellen diffundiert, kann das Serumkalium unauffällig/erhöht sein. Um Hypokaliämien zu verhindern sollte bei K+ <5.0mmol/L KCl zusammen mit Insulin i.v. verabreicht werden. Cave: gute Nierenfunktion des Patienten
Therapie: 1) +++ Flüssigkeit. 2) Insulin + KCl. 3) Auffüllen der Anionenlücke. 4) Auslösende Faktoren identifizieren. 5) Wenig PO4 (typischerweise wenige Stunden bis einen Tag nach der Ketoazidose durch ↑ ATP-Produktion.)
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Publikationsdatum: 17 Juni 2013 auf www.thecalgaryguide.com
Hyperosmolares/ Hyperglykämisches Koma (HHS)
Beachte: betrifft nur Patienten mit Diabetes mellitus Typ II
Beachte: Es sollte stets nach auslösenden Faktoren z.B. einer Infektion gesucht werden
Autor: Yan Yu Rezensenten:
Peter Vetere
Gill Goobie
Hanan Bassyouni* Übersetzung:
Sarah Schwarz Übersetzungsprüfung: Dr. Gesche Tallen
* MD zum Zeitpunkt der Veröffentlichung
Verschiebung des Wasser- und Elektrolythaushalts
Elektrolytstörung
Unzureichende Insulin- produktion, Insulinresistenz, Nichtansprechen auf Insulintherapie
Relativer Insulinmangel
Situationen mit ↑Insulinbedarf: Infekt, Pneumonie, Herzinfarkt, Pancreatitis, etc.)
Hyperglykämie
(Stark erhöhter Blutzucker, höher als bei der DKA)
Bei >12mmol/L, Glukosefiltration > - resorption, Glukose verbleibt im Urin
Glukosurie
Glukose ist osmotisch wirksam und zieht große Mengen Wasser mit sich (Osmotische Diurese)
Polyurie Dehydration
(ZVD↓, Orthostase: posturale Hypotension/posturale Tachykardie, Ruhepuls ↑ )
Durch das wenige noch vorhandene Insulin, wird ein Teil der Glukose von Muskel- /Fettgewebe verstoffwechselt, ein Teil verbleibt im Blut
Körperzellen brauchen eine weitere Energiequelle
Freisetzung kataboler Hormone: Glucagon, Katecholamine, Cortisol, Somatrotropin
Damit intrazellulärer Glukosespiegel ↑, erhöht der Körper den Blutzucker
Hypothalamische Zellen induzieren bei geringem intrazellulären Glukosespiegel ein starkes Hungergefühl
Polyphagie
Beachte: Durch das wenige noch
vorhandene Insulin wird die Lipolyse gehemmt und werden keine Ketonkörper produziert. Es kommt nicht zur Azidose und Ketonurie (Gegensatz zur DKA). Sollte es doch zur Ketourie kommen, ist das meist Folge von Hungerzuständen oder anderen Mechanismen
Extrazellulärflüssigkeit ↓ mit erhöhter Osmolarität (z.B. Hypernatriämie)
↑ Gluconeogenese, ↑ Glykogenolyse (in der Leber)
↓ Proteinsynthese, ↑ Proteolyse (in Muskelgewebe)
Substrate der Gluconeogenese ↑
Sollte der Patient nicht ausreichend trinken um das Volumendefizit auszugleichen
Falls Trinkwasser vorhanden
Polydipsie
Wasser verlässt Zellen entlang des osmotischen Gradienten, Neuronen schrumpfen
Neuronaler Schaden: Delirium, Krampfanfall, Benommenheit, Koma
Renale Perfusion↓, GFR ↓
Nierenversagen
(prä-renal, siehe entsprechende Folie)
Beachte: Während der DKA verliert der Körper K+ durch osmotische Diurese. Da gleichzeitig allerdings K+ aus den Zellen diffundiert, kann das Serumkalium unauffällig/erhöht sein. Um Hypokaliämien zu verhindern sollte bei K+ <5.0mmol/L KCl zusammen mit Insulin i.v. verabreicht werden.
Cave: gute Nierenfunktion des Patienten
Beachte: Elektrolytstörungen (z.B. Hyperkaliämien, Hypernatriämien) verschlechtern sich bei akutem Nierenversagen, welches bei der DKA &HK häufig auftritt
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Veröffentlicht: 3. November 2016 auf www.thecalgaryguide.com")
Nephrotisches Syndrom: Pathogenese und klinische Befunde

Lupus-Nephritis
Postinfektiöse Glomeruloneprhitis
IgA Nephropathie
Membranöse Glomerulonephritis
Antikörper greifen Podozyten an, Verdickung der glomerulären Basalmembran
Fokal-segmentale Glomerulosklerose (FSSGN)
Schädigung des glomerulären Endo- und Epithels
Minimal Change Glomerulo- nephritis (MCNG)
Diabetes mellitus
Autor: Yan Yu Rezensenten: Alexander Arnold David Waldner
Sean Spence
Stefan Mustata* Übersetzung:
Sarah Schwarz Übersetzungsprüfung: Gesche Tallen*
* MD zum Zeitpunkt der Veröffentlichung
Podozyten-Schädigung auf der epithelialen Seite des Glomerulums (Abflachung der Podozytenfortsätze)
Glomeruläre Immunkomplex- ablagerungen
Chronische Hyperglykämien schädigen das Glomerulum
Geschädigter Proteinfilter (v.a. für geladene Proteine)
Ablagerungen von Immunglobulin-Leichtketten im Glomerulum
Amyloidose
Geschädigte Glomeruli --> gestörte Filterbarriere v.a. für Proteine --> übermäßige Filtration von Plasmaproteinen
Vermehrte renale Ausscheidung von Immunglobulin-Leichtketten (Filtration>Resorption)
Hypoalbuminämie*
Übermäßiger Verlust an Albumin über den Urin
Proteinurie >3.5g/Tag*
Verlust an Antikoagulationsproteinen (Antithrombin, Plasminogen, Protein C & S) über den Urin
Koagulations- /Gerinnungsfaktoren (z.B. 1,7,8, 10) sind in Überzahl
Proteinurie >3.5g/Tag*
Thrombophilie
Anasarka
(Generalisiertes Ödem)
Lidödem
(klassisches Frühzeichen)
Lipidurie
(zeigt unter
gekreuztem polarisiertem Licht eine Malteserkreuz- form)
50% des Serumkalziums sind an Albumin gebunden, sodass Serumkalzium- spiegel ↓
Serum- Ca2+ repräsentiert nicht mehr das Gesamt-Ca2+
Beachte:
• DerklassischeSymptomkomplex(*)desnephrotischen Syndroms besteht aus: Proteinurie (>3,5g/Tag), Ödemen, Hypoalbuminämie,Hyperlipidämie
• Fürjede10g/LmitAlbumin<40:
➔ Addiere 2.5 zur errechneten Anionenlücke um
dessen “wahren” Wert zu bekommen
➔ Addiere 0,2mmol/L zum Gesamt-Ca um den
Wert des ionisierten Kalziums zu errechnen
Blut neigt zur Bildung von Thromben
Ödeme*
↑ Renale Filtrationder Lipide und Ausscheidung über den Urin
Die Anionenlücke ergibt sich hauptsächlich aus negativ geladenem Serumalbumin
Anionenlücke↓
Kolloid- osmotischer Druck ↓
Flüssigkeit kann nicht mehr in den Blutgefäßen gehalten werden und diffundiert ins Gewebe
Signalisiert der Leber die Albuminproduktion zuerhöhen,Albumin wird aber weiterhin über die Nieren verloren
Synthese- arbeit der Leber↑, auch ↑ Lipoprotein- synthese
Hyperlipidämie*:
(Serum-LDL, -VLDL, - TG ↑ )
Legende:
Pathophysiologie
Mechanismen
Symptome/Klinische Befunde
Komplikationen
Veröffentlicht: 19. August 2013 auf www.thecalgaryguide.com")
impetigo-patogenesis-y-hallazgos-clinicos

Psuedocholinesterase Deficiency

Break down or inhibit the pseudocholinesterase enzymeà↓ pseudo- cholinesterase activity
Note:
Pseudocholinesterase has many synonymous
names including butyrylcholinesterase, BChE, BuChE, plasma esterase, plasma cholinesterase, and serum cholinesterase
Malignancy Abnormal gene
expressionà↓ protein synthesis
Acquired
Liver disease
↓ liver’s ability to synthesize proteins
Malnutrition
↓ molecular precursors for protein production
Renal Disease
Mechanism unclear
Fluid Overload
Hemodilution of circulating proteins
Hereditary
BChE (Butyrylcholinesterase) gene mutation
↓ production or production of non-functional pseudo- cholinesterase by the liver
↓ synthesis of pseudocholinesterase by the liver
Pseudocholinesterase Deficiency: reduced levels of functional pseudocholinesterase in plasma and tissues
Impaired ability to hydrolyze ester linkages of substrates like neuromuscular blocking agents (e.g. succinylcholine, mivacurium, diamorphine, acetylsalicylic acid, methylprednisolone, cocaine, heroin )
Prolonged
binding of neuromuscular blocking agent to nicotinic cholinergic receptors in neuromuscular junctions
↑ patient’s susceptibility to side effects from drugs with ester linkages
Mivacurium administered to produce muscle paralysis
Succinylcholine administered
to produce muscle paralysis
Competitively binds to acetylcholine nicotinic receptor
Irreversibly binds to acetylcholine nicotinic receptor
Active site of post-synaptic acetylcholine receptor is blocked
Continuous depolarization
of skeletal muscle
Acetylcholine cannot act on receptor = skeletal muscle can’t depolarize
Skeletal muscle unable to repolarize
Skeletal muscle paralysis
Acetylcholine released cannot trigger an action potential
↑ duration of muscle fiber paralysis
Since respiratory muscles are affectedà Apnea requiring sedation and respiratory assistance for up to several hours
Extended paralysis and/or anesthesia
Authors: Evan Allarie Yan Yu* Reviewers: Stephen Chrusch Brooke Fallis Melinda Davis* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2021 on www.thecalgaryguide.com")
Primary Aldosteronism Pathogenesis
à↑ aldosterone
Overproduction of aldosterone, independent from renin-angiotensin- aldosterone system (RAAS)
Ectopic aldosterone secreting tumor
adrenocortical tissue outside of the adrenal glands produce aldosterone
Familial hyperaldosteronism (FH) Type I
Rare mutation causing ACTH- sensitive aldosterone production in the zona fasciculata
Aldosterone binds its receptor on the principal cells located in the collecting duct of the kidney
↑ Na+ and K+ channel insertion on luminal surface of the principal cell and ↑ Na/K ATPase activity on basolateral surface
Na+ follows the concentration gradient and moves into the principal cell cytoplasmàK+ moves into the collecting duct to maintain electroneutrality
Aldosterone binds its receptor on the alpha intercalated cells located in the late distal tubule and collecting duct of the kidney
↑ H+ ATPase and Na/H+ ATPase activity on the luminal surface of alpha intercalated cellsà↑ H+ excretion
H+ loss permits HCO3- to move down the electrochemical gradient across the luminal surfaceà↑ HCO3- resorption into peritubular capillaries
Metabolic alkalosis
K+ efflux (or hypokalemia of any etiology) is counterbalanced by influx of H+ into tubular cells to maintain electroneutrality
↓ pH in tubular cells activates glutaminase (a pH dependent enzyme) generating glutamate from glutamine
Glutamate within renal tubules dissociates into NH4+, HCO3- Intracellular acidosis within tubular cells
Disrupted cellular signaling within the collecting duct results in reduced APQ2 translocation to luminal surface
Authors: Kyle Moxham Reviewers: Emily Wildman Austin Laing Yan Yu* Matthew Harding* * MD at time of publication
Hypertension
↑ Na+ reabsorption
H2O follows active reabsorption
of solute into circulationà ↑ effective arterial blood volume (EABV)
Chronic EABV expansion resets hypothalamic osmotic sensitive ADH releaseàdecreased ADH production
↑ K+ excretion
Hypokalemia (see our Hypokalemia: Clinical Findings Slide)
↓ Na+ delivery to macula densa in the distal convoluted tubule
↓Endogenous renin secretion by juxtaglomerular apparatus while aldosterone continues to be independently produced
Polydipsia & Polyuria
Mild hypernatremia
↓ Renin: Aldosterone ratio
Nephrogenic diabetes insipidus: ↓ urinary concentrating ability
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2021 on www.thecalgaryguide.com")
Normal anion gap metabolic acidosis
, the distal nephron secretes one corresponding urine Cl- anion
Urine NH4+ cannot be measured, so measured
urine Cl- exceeds measured urine (Na+ + K+)
Negative urine net charge (Urine (Na+ + K+) - Urine Cl-)
Type II RTA RTA: renal tubular acidosis ↓ activity of proximal
Type I RTA
↓ activity of H+ ATPase on luminal surface of ⍺- intercalated cell in the collecting duct
Impaired ⍺-intercalated cell function
↓ H+ secretion into urine by ⍺- intercalated cell
↑ H+ concentration in plasmaà↓ in blood pH
Activation of blood bicarbonate buffer system
Compensatory ↓ in plasma HCO3- (in response to ↑ in plasma H+)
Type IV RTA
↓ aldosterone production or aldosterone resistant state
↓ Na+ channels on luminal surface of principal cell in the collecting duct
Impaired principal cell function
↓ Na+ reabsorption by principal cell
↑ Na+ remains in collecting duct lumen
↓ negative charge in collecting duct lumen
↓ K+ secretion into urine by principal cell
↑ K+ in plasma
Hyperkalemia
Normal anion gap
tubule transporters, pumps or enzymes
Impaired proximal tubule cell function
reabsorption
Complex and Incompletely understood mechanisms
Hypokalemia
Distal nephron function is impairedàdistal nephron is unable to secrete excess acid into the urine in the form of NH4+
↓ in urinary NH + 4
secretion is accompanied by corresponding ↓ in urinary Cl- secretion
Measured urine (Na+ + K+) exceeds measured urine Cl-
Positive urine net charge (Urine (Na+ + K+) - Urine Cl-)
↓ HCO3
-
in proximal tubule
↑ HCO3- loss through urine
↓ HCO3- concentration in plasma
Relative ↑ in plasma H+ compared to plasma HCO3-
Compensatory ↑ in CO2 exhalation by lungs (since CO2 is acidic once metabolized in the blood)
Since Anion gap = Na+ - Cl- - HCO3-,
1 to 1 replacement of Cl- for HCO - in the 3
plasma results in anion gap unchanged
↓ ability to buffer excess acid
Activation of the membrane Cl-/HCO3- exchanger in the collecting duct
Exchanger works to ↑ Cl- levels in the plasma by
one Cl- for each ↓ of one HCO3- in the plasma
Metabolic Acidosis
↓ Plasma partial pressure of CO2
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 21, 2021 on www.thecalgaryguide.com")
Renal Artery Stenosis
 of the renal artery
Renal Artery Stenosis can be unilateral or bilateral
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Jessica Krahn Timothy Fu, Brooke Fallis, Juliya Hemmett* * MD at time of publication
↓ Pressure perfusing the kidney
↑ RAAS (renin-angiotensin- aldosterone system) activation
↓ pressure gradient in glomerulus
↓ Glomerular filtration rate (GFR)
↑ Secretion of aldosterone
Turbulent blood flow through area of stenosis
Abdominal bruit on side of affected kidney(s)
↑ Secretion of Angiotensin IIà ↑ Systemic vasoconstriction
Hypertension
↑ Expression of epithelial sodium channels in cortical collecting duct
↑ Blood volume within volume- constrained space of blood vessels
↓ Renal blood flowà ischemic renal injury
Atrophy and fibrosis of affected kidney(s)
Unilateral stenosis à Kidney size asymmetry (≥1.5cm difference)
↓ Positively charged Na+ in lumen à Electronegative lumen compared to the interstitial/tubular epithelial cells
K+ follows the electrical gradient and is secreted into the electronegative tubular lumen
↓ Serum K+ concentration
Hypokalemia
*Note: In unilateral renal artery stenosis, the contralateral (normal) kidney can compensate for the increase in renal perfusion pressure caused by hypertension by increasing sodium excretion (pressure natriuresis), preventing flash pulmonary edema.
↑ NHE3 (Sodium Hydrogen Exchanger 3) activity in proximal collecting tubule
↑ Na+ and water reabsorption from renal tubular lumen into blood vessels
Chronic left ventricle pressure overload àLeft ventricle hypertrophy (see Left Heart Failure: Pathogenesis Slide)
Systolic dysfunction → ↓ left ventricle stroke volume
Normally, ↑ in renal perfusion pressureà↑ Na+ excretion and water loss (pressure natriuresis)
In bilateral renal artery stenosis*, ↓ GFRàinability for kidney to ↑ renal Na+ & water excretion à volume overload
Acute increase in afterload or preload → sudden ↑ in left ventricular filling pressures → blood backup into lungs
Pulmonary vasculature hypertension → ↑ fluid filtration across the pulmonary endothelium into interstitium and alveolar spaces
Flash (rapid onset) pulmonary edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 30, 2021 on www.thecalgaryguide.com")
Membranous Nephropathy
 Membranous Nephropathy
Secondary Membranous Nephropathy
Drugs, infections, auto-immune diseases, and malignancies make antigens
Blood tests for Anti- PLA2R antibodies
are positive in ~70% of cases
Autoantibodies are made to antigens expressed near or on podocyte surfaces or planted in the glomerular capillary wall (ie. PLA2R; THSD7A; NELL-1)
IgG antibodies filter through the glomerulus
Autoimmune: (e.g. Systemic Lupus Erythematous, thyroiditis)
Drugs: (e.g. NSAIDs, gold, penicillamine, captopril)
Malignancies: (ie. Prostate, Colon)
Infections: (e.g. Hepatitis B, Syphilis)
Circulating antigens filter through the glomerulus and between the GBM and podocytes
Antibodies & antigens form immunocomplexes, which lodge Immunofluorescence shows diffuse “granular”
between the glomerular basement membrane & podocytes
deposits of immunocomplexes throughout GBM
Basement membrane is formed between and around immunocomplex deposits
Immunocomplexes activate complement and the assembly of the Membrane attack complex (MAC)
MAC creates holes in podocyte plasma membranes
Stimulates the release/activation of proteases and oxidases from glomerular podocytes and mesangial cells
GBM appears thick on light microscopy
“Spike and dome” pattern appears with silver stain
Podocyte effacement
Damage to negatively charged foot processes damages the charge barrier of the glomerulus that repels negatively charged molecules
Increased filtration of large negatively charged molecules, especially albumin
Induces ↑ hepatic lipoprotein synthesis and ↓ lipoprotein catabolism
Hyperlipidemia
(↑ serum LDL, VLDL, and triglycerides)
↑ lipid filtration through glomerulus
Lipiduria (fatty casts)
*Hypo-albuminemia
↓ oncotic pressure in capillaries
Fluid leaks into interstitial space
↑ Filtration of Proteins C and S and antithrombin
Hypercoagulable state
Thrombosis *Edema (especially
*Proteinuria
↑ Filtration of immunoglobulins
Immunosuppression
Infections
↑ Filtration of Plasminogen
Plasminogen converted to plasmin in the cortical collecting duct via urokinase- type plasminogen activator
Plasmin activates the epithelial sodium channel
↓ intravascular volume
Hypotension
Pre-Renal Acute Kidney Injury
Underfill edema
(see slide)
peri-orbital, scrotal, labial, and extremities)
Overfill
edema
(see slide)
↑ Na+ and water reabsorption
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com")
Overview of Calcium Phosphate Vitamin D Physiology
 and ↓ expression of osteoprotegerin (OPG), a decoy receptor for RANKL
RANKL binds to receptor activator of nuclear factor kappa-B (RANK) on osteoclasts
↑ Osteoclast differentiation and activity
↑ Ca2+ resorption from bone into blood
Sensed by Calcium-Sensing Receptor on Chief Cells of the Parathyroid Gland
− −
↑ Serum phosphate (PO4) ↓ Serum calcium (Ca2+)
Parathyroid Gland releases Parathyroid Hormone (PTH) into the blood, which acts on the kidneys and the bones
Kidney
↑ Activation of Transient Receptor Potential Vanilloid subfamily member 5 (Ca2+ channel)
in the distal convoluted tubule
↓ Expression of 24-hydroxylase enzyme (which functions to catabolize calcitriol)
↑ Expression of 1α- hydroxylase enzyme
↑ Conversion of 25-hydroxy vitamin D (Calcidiol) to the
active form, 1,25-dihydroxy vitamin D (Calcitriol)
↑ Calcitriol Small Intestine
↑ Endocytosis of sodium phosphate co-transporters NaPi-2a and NaPi-2c, which reabsorb PO4 from ultrafiltrate in the renal tubules
↓ Reabsorption of PO 4
↓ Serum PO
Calcitriol negatively feeds back on parathyroid gland to inhibit PTH production
↑ Expression of sodium phosphate co- transporters NaPi-2a and NaPi-2b that absorb PO4 from intestinal lumen
4
↑ Expression of apical epithelial Ca2+ channels (Transient Receptor Potential Vanilloid subfamily member 6)
↑ Entry of Ca2+ on apical side of enterocytes
↑ Reabsorption of Ca2+ in the distal convoluted tubule through Ca2+ channels
↑ Reabsorption of PO
↑ Expression of cytoplasmic Calbindin-D
↑ Transport of Ca2+ across enterocytes
↑ Absorption of Ca2+ in small intestine
↑ Serum Ca+2
↑ Expression of basolateral plasma membrane calcium ATPase
↑ Extrusion of Ca2+ from enterocytes into bloodstream
4
Authors: Samin Dolatabadi, Hannah Yaphe Reviewers: Amanda Henderson, Meena Assad, Brooke Fallis, Yan Yu*, Hanan Bassyouni* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published Oct 15, 2017, updated Nov 11, 2021 on www.thecalgaryguide.com")
Minimal Change Disease
 present in serum
Immunofluorescence test negative
Idiopathic/Primary Minimal Change Disease
No identifiable extraglomerular disease process causes this condition
Secondary Minimal Change Disease
Infections, NSAIDS, neoplasms via unclear mechanisms
Minimal change to glomerulus seen on light microscopy
Podocyte effacement seen on electron microscopy
Abnormal T Cell activation and release of cytokines (sometimes called permeability factors) that are toxic to podocytes
Podocyte foot processes efface (become flattened) or fuse together
Damage to negatively charged foot processes damages the charge barrier of the glomerulus that repels negatively charged molecules
↑ filtration of larger negatively charged molecules, such as low-molecular weight proteins like albumin, from the blood into the renal tubular filtrate
Induces ↑ hepatic lipoprotein synthesis and ↓ lipoprotein catabolism
Hyperlipidemia
(↑ serum LDL, VLDL, and triglycerides)
↑ lipid filtration through glomerulus
Lipiduria (fatty casts)
Hypo-albuminemia
↓ oncotic pressure in capillaries
Fluid leaks into interstitial space
↑ Filtration of Proteins C and S and antithrombin
Hypercoagulable state
Proteinuria
↑ Filtration of immunoglobulins
Immunosuppression
Infections
↑ Filtration of Plasminogen
Plasminogen converted to plasmin in the cortical collecting duct via urokinase- type plasminogen activator
Plasmin activates the epithelial sodium channel
↓ intravascular volume
Hypotension
Pre-Renal Acute Kidney Injury
Underfill edema
(see slide)
Thrombosis Edema (especially peri-
orbital, scrotal, labial, and extremities)
Overfill
edema
(see slide)
↑ Na+ and water reabsorption
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 30, 2021 on www.thecalgaryguide.com")
ACE inhibitors
 inhibitors: Mechanism of Action and Clinical Findings Angiotensin Converting Enzyme (ACE) Inhibitors
Inhibits the conversion of angiotensin I to angiotensin IIà↓ serum angiotensin II levels
Inhibits breakdown of bradykinin
↓ Activation of zona glomerulosa region of the adrenal cortex
↓ Aldosterone secretion from the adrenal cortex
↓ Expression of basolateral Na+/K+ pump
and ↓ insertion of luminal Na+ channels in principal cells of the cortical collecting duct in kidney
↓ K+ secretion into urine
↑ Serum K+ concentration
Hyperkalemia
↓ Activation of Na+/H+ exchanger in proximal convoluted tubule (PCT) of the kidney
↓ Na+ absorption into PCT and ↓ H+ excretion into lumen
↓ Na+ absorption into the blood
↓ Renal H2O reabsorption via osmosis
↓ Activation of paraventricular nuclei located in the hypothalamus
↓ Secretion of anti- diuretic hormone (ADH)
into the capillaries of the posterior pituitary gland
↓ Aquaporin channel insertion at cortical collecting duct in kidney
↓ Renal H2O reabsorption
à↑ serum bradykinin levels Vasodilation of efferent
arteriole in kidneys
↓ Hydrostatic pressure within the glomerular capillaries
↑ Activation of cyclooxygenase-2 pathway
↑ Prostaglandin production
↓ Activation of angiotensin II type 1 receptors on surface of arteriolar smooth muscle
↓ Activity of G protein-coupled receptor intracellular secondary messenger cascade
↓ Systemic arteriolar vasoconstriction
↓ Total peripheral resistance (resistance
to blood flow by systemic vasculature)
↓ Blood Pressure
↓ total blood flow perfusing kidneys
Renal hypoxia
↑ Systemic arteriolar vasodilation
↓ Total peripheral resistance
↓ Blood Pressure
↓ Concentration of protein
travelling through tubules for excretion
↓ Fraction of H2O filtered from glomerular capillaries into bowman’s capsule (start of the renal tubule)
↓ Filtration of blood contents through glomerular membranes
Sensitization of airway vagal afferent receptors
Stimulation of the cough
center located in the medulla oblongata
Cough
↓ Protein in urine
High K+ levels surrounding the heart muscle cellsàchronic depolarization
of the cardiomyocyte cell membrane àalters cardiomyocyte conduction (complex mechanisms)
Cardiac Arrythmias (see relevant slide on Hyperkalemia: Clinical Findings)
↓ Effective arterial blood volume
Authors:
Nicole Brockman Reviewers:
Emily Wildman, Austin Laing Adam Bass*, Yan Yu*
* MD at time of publication
Renal tubules have relatively less water compared with the peritubular capillaries
↓ H2O reabsorption from the renal tubule back into the blood
↑ Serum creatinine, ↓ estimated glomerular filtration rate
Renal nephron injury and dysfunction
Acute Kidney Injury
(rise in creatinine >26.5umol/L in <7 days)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 10, 2022 on www.thecalgaryguide.com")
complications-of-chronic-kidney-disease-ckd

Authors: Samin Dolatabadi, Brooke Fallis Reviewers: Jessica Krahn, Meena Assad, Yan Yu* Juliya Hemmett* * MD at time of publication
Abnormalities of kidney structure or function that is present for 3 or more months
Kidney tubules atrophy & kidney interstitial tissue undergo fibrosis
Kidney damage ↓ erythropoietin production (normally a kidney function)
↓stimulation of bone marrow → ↓ red blood cell production
Build up of toxic substances (e.g. urea, guanidine, and indoxyl sulfate)
↓ Conversion of calcidiol to calcitriol in by kidney
↓ Calcitriol levels in blood
↓ Ca+2 absorption from small intestine
Hypocalcemia
↓ Glomerular Filtration Rate
↑ Vascular calcification and endothelial dysfunction (e.g. changes in permeability, clotting response to inflammation, amongst other mechanisms)
Atherosclerotic disease (see “Complications of Atherosclerosis” slide)
↓ Lipoprotein lipase, apoA-1, and Lecithin-cholesterol acyltransferase
activity acting on serum lipoproteins (complex mechanisms)
↓ Lipoprotein clearance from blood
Dyslipidemia (↑ LDL, ↑ triglycerides, ↓ HDL)
Toxic damage ↓ red blood cell survival
Anemia
Uremic Syndrome
↓ Renal excretion of phosphate
↑ phosphate remaining in bloodstream
Hyperphosphatemia
↑ serum phosphate binds with ionized calcium
↓ Renal excretion of K+
↑ K+ remaining in bloodstream
Hyperkalemia Edema
↓ Renal excretion of ammonium
Reduced filtration capability ↑ organic anions remaining in blood→ ↑ anion gap
↓ Renal excretion of salt and water
↑ in extracellular fluid → systemic volume overload
↓ calcium in blood ↓ inhibition of Parathyroid Hormone (PTH) release
↑ PTH in blood
Secondary hyperparathyroidism
Metabolic Acidosis
Hypertension
Pitting
Chronic kidney disease – mineral and bone disorder (CKD-MBD)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 4, 2022 on www.thecalgaryguide.com")
NSAIDs and the Kidney Nephrotoxicity

Authors: Kyle Moxham Mehul Gupta Reviewers: Emily Wildman Yan Yu* Adam Bass* * MD at time of publication
Inhibition of Cyclooxygenase COX-1 (expressed in kidney) and COX-2 (expressed in kidney and sites of inflammation)
NSAID induced nephrotoxicity: associated with chronic NSAID usage independent of dosage
COX inhibition ↑ conversion of arachidonic acid (AA) to leukotrienes, causing systemic T-cell dysfunction (unknown mechanism)
Type IV systemic hypersensitivity (delayed
T helper cell mediated) reaction to drug exposure
T cells release inflammatory cytokines into the bloodstream
(see Calgary Guide slide on NSAIDs and the Kidney: Mechanism of Action and Side Effects)
T cells infiltrate the renal interstitium, sparing the glomeruli and blood vessels
Overproduction of cytokines by T cells causing inflammation,
tissue damage, and cell death, of the renal intersitium
Drug Induced Acute interstitial nephritis (AIN): a type of immune-mediated tubulointerstitial injury
Activated T-cells infiltrate the glomerulus and cause podocyte injury (epithelial cells attached to the glomerular basement membrane)
Membranous nephropathy:
nephrotic syndrome involving autoimmune glomerular basement membrane thickening & complete podocyte effacement (seen on kidney biopsy)
Minimal change disease: nephrotic syndrome caused by autoimmune podocyte effacement (seen on kidney biopsy)
Cytokine mediated activation and
proliferation of immune cells like macrophages and eosinophils
Cytokines travel to hypothalamus,
causing change in the body’s thermal set point
Fever
Podocyte effacement allows for serum proteins to across the glomerulus into the tubular lumen (see Calgary Guide slide on Nephrotic Syndrome for full mechanisms)
Repeated NSAID exposure causing
recurrent unrecognized AIN and damage of the kidney
Chronic interstitial nephritis /analgesic nephropathy
Infiltrating immune cells (predominantly neutrophils) are filtered into/enter the renal tubules, and form clumps (“casts”) within the tubulesà casts are then released into urine
WBC cast on urinalysis
↑ Blood eosinophils
Immune cells infiltrate the
dermis and epidermis of the skin
Rash
Abnormal quantities of protein present in urine
Protein present in the blood is improperly filtered into the filtrate at the glomerulus
Protein- Creatinine
Ratio >3.5mg/mg
Proteinuria >3.5g/d
Hypo- albuminemia
↓ plasma oncotic pressure resulting in fluid extravasation into the interstitium (see Calgary guide slide on Edema for full mechanisms)
Pitting Edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 13, 2022 on www.thecalgaryguide.com")
Overfill Edema Pathogenesis

Aberrant filtration of proteins including plasminogen
(glycoprotein in the systemic circulation involved in the dissolution of fibrin blood clots)
↑ Plasminogen concentration in tubular fluid
Conversion of plasminogenà plasmin by urokinase-type plasminogen activator in the cortical collecting tubule
Plasmin activates epithelium
sodium channels (involved in Na+ reabsorption) in principal cells of the cortical collecting duct
Nonsteroidal Anti-inflammatory Drugs
Inhibition of cyclooxygenase throughout body (enzyme that converts arachidonic acidàprostaglandins)
↓ Prostaglandins throughout body
Thiazolidines
↓ Prostaglandin- mediated inhibition of Na+ and Cl- transport in ascending loop of Henle and collecting ducts
↑ Na+ reabsorption from kidney tubules back into blood
↓ Prostaglandin-mediated vasodilation in kidneys
↓ Pressure of blood perfusing kidneys → ↓ pressure gradient between glomerulus and bowman’s capsule
↓ Glomerular filtration rate
↓ Renal excretion of salt & water
↑ Salt and water retention
↑ Effective arterial blood volume
↑ blood pressure in veins
Unclear mechanism but possible theories include upregulation of epithelium sodium channels in the cortical collecting tubule and involvement of other transporters in the proximal tubule and cortical collecting tubule
Acute Renal Failure Chronic Renal Failure
↑ Hydrostatic pressure within capillariesàexceeds hydrostatic pressure within interstitial spaceàfluid moves from capillaries into interstitial space
Overfill Edema
Abnormal accumulation of fluid in the interstitial space where urine Na+ >40meq/L
Authors: Samin Dolatabadi Reviewers: Meena Assad, Jessica Krahn, Brooke Fallis, Ran (Marissa) Zhang, Yan Yu*, Juliya Hemmett* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 23, 2022 on www.thecalgaryguide.com")
NSAIDs and the Kidney mechanism of action and side effects
 or angiotensin II receptor blockers (ARB)
AECi and ARBs act to ↓ renin- angiotensin-aldosterone system (RAAS) activation
Reduced angiotensin (AT) 2 activity at its receptors on efferent arteriole of the nephron
Net vasodilation of efferent arterioles ↓ in glomerular pressure
↓ blood perfusing kidney tissueà↑ hypoxemia & renal ischemia
Pre-existing ↓effective arterial blood volume (EABV) from
dehydration, GI loss, diuretics, CKD, CHF, cirrhosis, etc.
Decreased EABV triggers endogenous renal autoregulation, resulting in norepinephrine (NE) mediated vasoconstriction of afferent arteriole of the nephron
Net ↓ in renal blood flow and ↓ in glomerular pressure
↓ volume of blood filtered by the glomeruli per unit time
Non-steroidal anti-inflammatory drugs (NSAIDs)
Inhibition of Cyclooxygenase COX-1 (expressed in kidney) and COX-2 (expressed in kidney and sites of inflammation)
↓ Renal prostaglandin (PG) synthesis: local hormones involved in renal homeostasis
NSAID induced nephrotoxicity:
associated with chronic usage independent of dosage
(see Calgary Guide slide on NSAIDs and the Kidney: NSAID induced nephrotoxicity)
↓ intrarenal PG reduces inhibitory effects of PG over ADH in cortical colleting duct (CCD) of the kidneyà↓ antagonism on ADH activity
↑ ADH activity causes insertion of more
aquaporins (water channels) in the collecting duct of renal tubules
Net ↑ in volume of water reabsorbed into the blood
↓ vasodilatory effect of PG at the afferent arteriole of the nephron
↓ Glomerular filtration rate (GFR)
↓ PG signalling results in ↓ renin secretion at juxtaglomerular apparatus
Low renin levelsà↓ conversion of angiotensinogen into its AT1 form and, by extension, ACE mediated conversion of AT1 to AT2
↓ ACE 2 signalling leads to ↓ levels of aldosterone in the serum
↓ Na+ and K+ channel insertion on apical surface and ↓ Na/K ATPase activity on basolateral surface of principal cells
↓ K+ excretion into urine, and ↓ Na+ reabsorption
back into the blood, at the late DCT and collecting duct of the kidney
Pre-renal Acute Kidney Injury (AKI): kidney injury due to renal hypoperfusion
Prolonged and/or severe ischemia causes cell death and aggregation of tubular epithelial cells of the kidney with subsequent inability to reabsorb luminal Na+
Renal dehydration predisposes
precipitation of uromodulin protein
Renal tubules mold uromodulin into cylindrical structures known as “casts”. Casts that contain only uromodulin protein are known as “hyaline casts”
Hyaline cast seen on urinalysis
Hypoperfusion of the kidney activates the renin- angiotensin- aldosterone system (RAAS)
↑ amount of sodium (Na) reabsorbed from the filtrate (less Na excreted)
Fractional excretion of Na <1%
Papillary necrosis: ureteral passage of sloughed ischemic tissue causing ureteral obstruction
Acute tubular necrosis: a type of kidney injury causing damage to the tubules
Hypertension
Post-renal AKI: a type of kidney injury due to
obstruction of the urinary tract
Distal distal obstruction of the urinary tract causes fluid to accumulate within the kidneysàenlarging the kidneys
Renal Ultrasound shows hydronephrosis (enlarged kidneys)
Damaged tubule epithelial cells slough into the tubular lumen
Epithelial cell breakdown in the tubular lumen
releases uromodulin & other proteins, which aggregate into “casts” (cylindrical imprints of the renal tubule). The varied protein content of these casts result in them having a coarse, granular appearance
Damaged tubular epithelial cells are unable to properly reabsorb sodium
↓ amount of sodium (Na) reabsorbed from filtrate into the blood (more Na excreted)
Fractional excretion of Na >2%
True excess of free water relative to Na+ in the blood
Excess free water ↑ venous hydrostatic pressure (see Calgary Guide slide on edema for full mechanisms)
Pitting Edema
Hyperkalemia
Hyponatremia
Coarse granular casts seen on urinalysis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 29, 2022 on www.thecalgaryguide.com")
Hypokalemia Physiology
![Hypokalemia: Physiology
Authors: Samin Dolatabadi, Ran (Marissa) Zhang, Mannat Dhillon Reviewers: Meena Assad, Yan Yu*, Juliya Hemmett*
Beta-2 receptor stimulation
(e.g. Salbutamol)
↑ Red blood cell production
↑ Na+/K+ ATPase activity in skeletal muscle cells (moves K+ into the cell & Na+ out of cell)
↑ K+ entry into skeletal muscle cells
* MD at time of publication
Abbreviations:
• EABV – Effective Arterial
Blood Volume
• ENaC – Epithelial Sodium
Channel
• HCL – Hydrochloric acid • HCO3- –Bicarbonate ion
↑ K+ uptake by new red blood cells
↑ Intracellular shift of K+ into cells
Refeeding Syndrome Exogenous insulin
↓ K+ dietary intake
(rare cause in isolation)
↑ Insulin in response to carbohydrate load
↑ Na+/K+ ATPase activity in skeletal muscle & hepatic cells
↑ K+ entry into skeletal muscle & hepatic cells
↓ K+ availability for gastrointestinal absorption
Hypokalemia (Serum [K+] < 3.5 mmol/L)
↑ Renal K+ secretion
K+ follows the electrical gradient into tubular lumen
↑ Electronegativity of tubular lumen
↑ Na+ reabsorptionin principal cellsà Cl- left behind in tubular lumen of kidneys
Gastric acid depletionà ↓HCl
Loss of H+àShift in bicarbonate buffer system to ↑ plasma HCO3-
Plasma HCO3- above reabsorptive capacity of the proximal tubule
↑ HCO3- in the distal tubular lumen of kidneys
Vomiting
Diarrhea Laxatives
Renin secreting tumour Hyperaldosteronism Renal artery stenosis Loop and Thiazide
diuretics
Bartter’s and Gittelman’s syndrome
Liddle syndrome
Extracellular fluid volume depletion
↓ EABV ↑ Renin secretion
↓ Afferent arteriole pressure perfusing kidneys
Renin-Angiotensin- Aldosterone System (RAAS) activationà ↑ Aldosterone release from the adrenal cortex
↑ Expression of ENaC (Na+ reabsorption) in principal cells of the cortical collectingduct)
+ ↑Na &
water excretion in kidneys
↓ EABV
Genetic condition leading to inability to degrade ENaC channels in principal cells of the cortical collecting duct
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019, updated Jan 23, 2022 on www.thecalgaryguide.com
Hypokalemia: Physiology
Authors: Samin Dolatabadi Reviewers: Meena Assad Dr. Juliya Hemmett* * MD at time of publication
TTKG > 4 with N/↑ EABV in hypokalemia is inappropriate and a principal cell problem.
β2 Stimulation (e.g., Salbutamol)
↑ Na+/K+ ATPase activity
↑ K+ entry into cell
↑ RBC Production
↑ Cell production
↑ K+ uptake by new cells
↓ Extracellular ↑ Insulin in response to H+
carbohydrate load
↑ Na+/H+ antiporter activity (movement of H+ out of cell and Na+ into cell)
↑ Intracellular Na+
↑ Na+/K+ ATPase activity ↑ K+ entry into cell
↑ Intracellular Shift of K+
Notes:
Refeeding Syndrome
Insulin
Alkalemia
•
Abbreviations:
• CCD – Cortical Collecting Duct
• EABV – Effective Arterial Blood Volume
• RAAS – Renin-Angiotensin-Aldosterone System • TTKG – Trans-tubular Potassium Gradient
• ENaC – Epithelial Sodium Channel
↓ K+ Intake (Rare cause in isolation)
↓ K+ availability
Diarrhea, Vomiting, Laxatives
↑ Gastrointestinal loss of K+
Polyuria
↑ Renal loss of K+ (TTKG < 4 as principal cell is working appropriately but small amount of K+ is lost per urination)
Hypokalemia (Serum [K+] < 3.5 mmol/L)
Liddle Syndrome Hyperaldosteronism Renin Secreting Tumour
Renal artery stenosis
Loop and Thiazide Diuretics
Bartter’s and Gittelman’s Syndrome
Genetic condition leading to inability to degrade ENaC channels ↑ Renin
↑ Renal K+ secretion
K+ follows the electrical gradient
Electronegative lumen
↓ Pressure perfusing the kidney
RAAS activation RAAS activation
↑ Aldosterone
↑ Na+ and water excretion
↓ EABV
↑ Expression of ENaC in principal cells of CCD
↑ Na+ reabsorption
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2019/03/Hypokalemia-Physiology.jpg "Hypokalemia: Physiology
Authors: Samin Dolatabadi, Ran (Marissa) Zhang, Mannat Dhillon Reviewers: Meena Assad, Yan Yu*, Juliya Hemmett*
Beta-2 receptor stimulation
(e.g. Salbutamol)
↑ Red blood cell production
↑ Na+/K+ ATPase activity in skeletal muscle cells (moves K+ into the cell & Na+ out of cell)
↑ K+ entry into skeletal muscle cells
* MD at time of publication
Abbreviations:
• EABV – Effective Arterial
Blood Volume
• ENaC – Epithelial Sodium
Channel
• HCL – Hydrochloric acid • HCO3- –Bicarbonate ion
↑ K+ uptake by new red blood cells
↑ Intracellular shift of K+ into cells
Refeeding Syndrome Exogenous insulin
↓ K+ dietary intake
(rare cause in isolation)
↑ Insulin in response to carbohydrate load
↑ Na+/K+ ATPase activity in skeletal muscle & hepatic cells
↑ K+ entry into skeletal muscle & hepatic cells
↓ K+ availability for gastrointestinal absorption
Hypokalemia (Serum [K+] < 3.5 mmol/L)
↑ Renal K+ secretion
K+ follows the electrical gradient into tubular lumen
↑ Electronegativity of tubular lumen
↑ Na+ reabsorptionin principal cellsà Cl- left behind in tubular lumen of kidneys
Gastric acid depletionà ↓HCl
Loss of H+àShift in bicarbonate buffer system to ↑ plasma HCO3-
Plasma HCO3- above reabsorptive capacity of the proximal tubule
↑ HCO3- in the distal tubular lumen of kidneys
Vomiting
Diarrhea Laxatives
Renin secreting tumour Hyperaldosteronism Renal artery stenosis Loop and Thiazide
diuretics
Bartter’s and Gittelman’s syndrome
Liddle syndrome
Extracellular fluid volume depletion
↓ EABV ↑ Renin secretion
↓ Afferent arteriole pressure perfusing kidneys
Renin-Angiotensin- Aldosterone System (RAAS) activationà ↑ Aldosterone release from the adrenal cortex
↑ Expression of ENaC (Na+ reabsorption) in principal cells of the cortical collectingduct)
+ ↑Na &
water excretion in kidneys
↓ EABV
Genetic condition leading to inability to degrade ENaC channels in principal cells of the cortical collecting duct
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019, updated Jan 23, 2022 on www.thecalgaryguide.com
Hypokalemia: Physiology
Authors: Samin Dolatabadi Reviewers: Meena Assad Dr. Juliya Hemmett* * MD at time of publication
TTKG > 4 with N/↑ EABV in hypokalemia is inappropriate and a principal cell problem.
β2 Stimulation (e.g., Salbutamol)
↑ Na+/K+ ATPase activity
↑ K+ entry into cell
↑ RBC Production
↑ Cell production
↑ K+ uptake by new cells
↓ Extracellular ↑ Insulin in response to H+
carbohydrate load
↑ Na+/H+ antiporter activity (movement of H+ out of cell and Na+ into cell)
↑ Intracellular Na+
↑ Na+/K+ ATPase activity ↑ K+ entry into cell
↑ Intracellular Shift of K+
Notes:
Refeeding Syndrome
Insulin
Alkalemia
•
Abbreviations:
• CCD – Cortical Collecting Duct
• EABV – Effective Arterial Blood Volume
• RAAS – Renin-Angiotensin-Aldosterone System • TTKG – Trans-tubular Potassium Gradient
• ENaC – Epithelial Sodium Channel
↓ K+ Intake (Rare cause in isolation)
↓ K+ availability
Diarrhea, Vomiting, Laxatives
↑ Gastrointestinal loss of K+
Polyuria
↑ Renal loss of K+ (TTKG < 4 as principal cell is working appropriately but small amount of K+ is lost per urination)
Hypokalemia (Serum [K+] < 3.5 mmol/L)
Liddle Syndrome Hyperaldosteronism Renin Secreting Tumour
Renal artery stenosis
Loop and Thiazide Diuretics
Bartter’s and Gittelman’s Syndrome
Genetic condition leading to inability to degrade ENaC channels ↑ Renin
↑ Renal K+ secretion
K+ follows the electrical gradient
Electronegative lumen
↓ Pressure perfusing the kidney
RAAS activation RAAS activation
↑ Aldosterone
↑ Na+ and water excretion
↓ EABV
↑ Expression of ENaC in principal cells of CCD
↑ Na+ reabsorption
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com")
metabolic-alkalosis-pathogenesis
![Metabolic Alkalosis: Pathogenesis
Authors: Wazaira Khan Reviewers: Jessica Krahn, Emily Wildman, Austin Laing, Huneza Nadeem, Ran (Marissa) Zhang, Adam Bass* * MD at time of publication
Primary hyperaldosteronism E.g., aldosterone- secreting mass, adrenal hyperplasia
Secondary hyperaldosteronism E.g., renin-secreting mass, renal artery stenosis
Pseudo- hypoaldosteronism E.g., Liddle’s Syndrome
Unregulated aldosterone production in adrenal cortex
Excess aldosterone suppresses renin production
Unregulated renin production by juxtaglomerular cells
Sustained ↑ in mineralocorticoid (aldosterone) activity
Insertion of epithelial sodium channels on principal cells in collecting duct
↑ Water retention by the kidney
↑ Na+ reabsorption by principal cells
↑ EABV
• ↑ Jugular venous pressure • Hypertension
• Urine Na+ > 40 mEq/L
Low renin, high aldosterone state
Activation of renin- angiotensin-aldosterone system (RAAS)
Release of aldosterone from adrenal cortex
High renin, high aldosterone state
↑ Negative charge in collecting duct lumen
K+ leaks into collecting duct lumen by principal cell to maintain electroneutrality
Hypokalemia
Intracellular K+ leaks out of any cell in the body to compensate for low serum K+ levels
Extracellular H+ enters cell to maintain electroneutrality
Intracellular acidosis
Activation of compensatory acid secreting mechanisms in kidney
Impaired tubular function
E.g., loop/thiazide diuretics, Bartter’s/ Gitelman’s Syndrome
Upper GI Loss
E.g., vomiting, nasogastric suction
Unregulated epithelial sodium channel activity in collecting duct mimicking aldosterone function
↑ in Na+ and water retention à RAAS inhibition
↓ Na+ and Cl- reabsorption in thick ascending limb or distal convoluted tubule
Low renin, low aldosterone state
↑ Na+, Cl- and water secretion through kidney
RAAS activation
See “Physiology of RAAS” slide
↓ EABV • • •
Temporary ↑ in mineralocorticoid (aldosterone) activity
↓ Jugular venous pressure Orthostatic hypotension Dry mucous membranes Urine Na+ < 20 mEq/L
•
Loss of fluid through GI tract
↓ HCl delivery to small intestine
↑ NH + secretion and 4
↑ HCO3- reabsorption in proximal tubule
↑ H+ secretion in cortical collecting duct
Loss of gastric contents, including HCl
↓ HCO3- secretion by pancreas, liver and intestines to neutralize HCl
Loss of intrinsic acid to neutralize HCO3- ↑ Plasma [HCO3-]
Metabolic Alkalosis
Arterial blood gas pH > 7.40 Plasma [HCO3-] > 24 mEq/L
Effective Arterial Blood Volume (EABV): component of arterial blood volume that is effectively perfusing organs
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 31, 2022 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2022/05/Metabolic-Alkalosis-1.jpg "Metabolic Alkalosis: Pathogenesis
Authors: Wazaira Khan Reviewers: Jessica Krahn, Emily Wildman, Austin Laing, Huneza Nadeem, Ran (Marissa) Zhang, Adam Bass* * MD at time of publication
Primary hyperaldosteronism E.g., aldosterone- secreting mass, adrenal hyperplasia
Secondary hyperaldosteronism E.g., renin-secreting mass, renal artery stenosis
Pseudo- hypoaldosteronism E.g., Liddle’s Syndrome
Unregulated aldosterone production in adrenal cortex
Excess aldosterone suppresses renin production
Unregulated renin production by juxtaglomerular cells
Sustained ↑ in mineralocorticoid (aldosterone) activity
Insertion of epithelial sodium channels on principal cells in collecting duct
↑ Water retention by the kidney
↑ Na+ reabsorption by principal cells
↑ EABV
• ↑ Jugular venous pressure • Hypertension
• Urine Na+ > 40 mEq/L
Low renin, high aldosterone state
Activation of renin- angiotensin-aldosterone system (RAAS)
Release of aldosterone from adrenal cortex
High renin, high aldosterone state
↑ Negative charge in collecting duct lumen
K+ leaks into collecting duct lumen by principal cell to maintain electroneutrality
Hypokalemia
Intracellular K+ leaks out of any cell in the body to compensate for low serum K+ levels
Extracellular H+ enters cell to maintain electroneutrality
Intracellular acidosis
Activation of compensatory acid secreting mechanisms in kidney
Impaired tubular function
E.g., loop/thiazide diuretics, Bartter’s/ Gitelman’s Syndrome
Upper GI Loss
E.g., vomiting, nasogastric suction
Unregulated epithelial sodium channel activity in collecting duct mimicking aldosterone function
↑ in Na+ and water retention à RAAS inhibition
↓ Na+ and Cl- reabsorption in thick ascending limb or distal convoluted tubule
Low renin, low aldosterone state
↑ Na+, Cl- and water secretion through kidney
RAAS activation
See “Physiology of RAAS” slide
↓ EABV • • •
Temporary ↑ in mineralocorticoid (aldosterone) activity
↓ Jugular venous pressure Orthostatic hypotension Dry mucous membranes Urine Na+ < 20 mEq/L
•
Loss of fluid through GI tract
↓ HCl delivery to small intestine
↑ NH + secretion and 4
↑ HCO3- reabsorption in proximal tubule
↑ H+ secretion in cortical collecting duct
Loss of gastric contents, including HCl
↓ HCO3- secretion by pancreas, liver and intestines to neutralize HCl
Loss of intrinsic acid to neutralize HCO3- ↑ Plasma [HCO3-]
Metabolic Alkalosis
Arterial blood gas pH > 7.40 Plasma [HCO3-] > 24 mEq/L
Effective Arterial Blood Volume (EABV): component of arterial blood volume that is effectively perfusing organs
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 31, 2022 on www.thecalgaryguide.com")
pheochromocytoma-pathogenesis-and-clinical-findings
 Zhang Hanan Bassyouni* * MD at time of publication
↑ Blood pressure results in the activation of neural pain receptors
Sustained or paroxysmal 2o hypertension (↑ blood pressure)
Pallor
Tachycardia (↑ heart rate), palpitations
Diaphoresis (excessive sweating)
Hyperglycemia Weight loss, fatigue
Familial Disorders (10%)
E.g., Multiple Endocrine Neoplasm 2 Syndrome (MEN2) types A and B, Neurofibromatosis 1 (NF-1), Von Hippel Lindau Syndrome (VHL), familial pheochromocytoma
Dysfunction of various tumor suppressor and/or oncogene proteins
Uncontrolled proliferation of the chromaffin cells in the medulla of the adrenal gland(s)
Adenoma formation (10% bilateral)
Over-production of epinephrine and
norepinephrine from the adrenal adenoma(s) or extra- adrenal tumour (10%)
Detectable metanephrines (epinephrine/norepinephrine breakdown products) in both plasma and urine
Sporadic DNA mutations arising from
DNA damage from exposure to mutagens, malignancy (10%), or during DNA replication
Detectable mutations on the Von Hippel Linda (VHL), (Rearranged During Transcription) RET, (Succinate Dehydrogenase) SDH, and/or other tumour suppressor or oncogenes
Visible adrenal mass on CT scan Heart attack, stroke, or death (Note: These
tumors can be fatal therefore screening is essential in patients with adrenal masses or 2o hypertension)
Episodic hyper-activity of the sympathetic nervous system
Hyper-stimulation of G protein-coupled receptors involved in catabolic metabolic processes
Headaches
↑ Vasoconstriction of peripheral blood vessels
Hyper-stimulation of adrenergic receptors on cardiac myocytes
↑ Secretion from the eccrine sweat glands
Panic, tremor, anxiety
↑ Ability to mobilize glucose into the bloodstream through enhanced lipolysis, glycogenolysis and gluconeogenesis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 20, 2014, updated June 27, 2022 on www.thecalgaryguide.com")
Epilepsy Pathogenesis

Neoplasm
Metabolic
Inborn errors of metabolism
Inherited enzyme deficiencies
Neurodegenerative
Alzheimer’s Disease
Protein-rich plaque build-up and brain atrophy
Inflammation and formation of scar tissue irritates neural tissue
Infiltration of mass, grey matter irritation
Damage to the brain and subsequent alteration of neuronal circuitry
Neurotransmitter imbalances (i.e. ↑ glutamate, ↓ GABA, ↓ serotonin, ↓ dopamine, ↓ noradrenaline)
Abbreviations:
• HSV1 – Herpes Simplex Virus 1 • VZV – Varicella Zoster Virus
↑ Inflammatory cytokines (e.g. interleukin-6, tumor necrosis factor-α)
Altered neurogenesis and gliosis
Ion channel and receptor dysfunction causes imbalance of ion channel charges
Authors: Keerthana Pasumarthi Christopher Li Reviewers: Negar Tehrani, Ephrem Zewdie, Ran (Marissa) Zhang, Carlos R. Camara-Lemarroy* * MD at time of publication
Neurons fire in burst activity (referred to as paroxysmal depolarization shift) and often in groups (hypersynchrony)
Abnormal neural activities eventually create self-reinforcing circuits and transform neural network over time
Injuries from
falls, bumps, operating heavy machinery
Involuntary contractions Loss of consciousness
Post-ictal confusion
Recurrent seizures
Sudden Unexplained Death of Epilepsy Patient (SUDEP)
Loss of airway reflexes
Aspiration of saliva or food contents
Aspiration Pneumonia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 5, 2022 on www.thecalgaryguide.com")
etomidate

↓ Adrenal cortisol production
↓ Serum cortisol available for stress response
Transient adrenal steroid insufficiency
↑ Morbidity & mortality in trauma/critically ill patients (Contraindicated in sepsis)
Inhibits nitric oxide signaling
Transient cerebral vasoconstriction
↓ Cerebral blood flow
↓ Oxygen delivery to brain
↓ Cerebral metabolic rate
Suppression of electrical activity in brain
Flat electroencephalogram
Binds to GABAA
(inhibitory CNS neurotransmitter) receptor
Authors:
Cindy Chang
Ran (Marissa) Zhang Reviewers:
Melissa King
Brooke Fallis
Julia Haber*
* MD at time of publication
Abbreviations:
• CNS - Central Nervous
System
• GABAA- Gamma-
aminobutyric acid type A • TRPA1- Transient
receptor potential type A1
Higher selectivity for specific GABAA receptor subtypes compared to other induction agents
Positively modulates GABAA receptor (GABAA receptor activated at lower concentrations of GABA )
↓ Cerebral blood volume
Activation of fewer GABAA receptor subtypes in neurons and cardiovascular structures compared to other induction agents
↓ Intracranial pressure ↑ Hemodynamic stability
(minimal changes in blood pressure or heart rate)
Myoclonus (brief, involuntary, irregular muscle twitch)
↑ Spontaneous CNS neuron firing to skeletal muscle
Prolonged opening of GABAA receptors (acts as ion channel for chloride)
Inhibits activity of nerve cells in the reticular activating system
Activation of peripheral nociceptor receptors
↑ Involuntary muscle contractions
Influx of chlorideàHyperpolarization of nerve membranes in reticular activating system
(brainstem neuronal network that regulates arousal and sleep- wake transitions)
Depression of arousal & loss of consciousness
Induction of general anesthesia
(no analgesic effect)
Direct activation of TRPA1 cation channels (key receptor in pain pathway)
Stinging pain with injection
(Treat with co-administration of local anesthetic)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 9, 2022 on www.thecalgaryguide.com")
complicaciones-de-la-enfermedad-renal-cronica

hyperkalemia-↓-renal-excretion-pathophysiology
![Hyperkalemia (↓ Renal Excretion): Pathophysiology
Non-steroidal anti- inflammatory drugs (NSAIDs)
Inhibition of prostaglandins which promote renin secretion (see NSAIDs and the Kidney: Mechanism of Action and Side Effects slide)
Diabetic Nephropathy
Acute (AIN)and chronic (CIN) interstitial nephritis
Immune-mediated damage of the kidney tubule and interstitium
Damage to distal tubule leads to aldosterone resistance at principal cell
Aldosterone cannot ↑ EnaC insertion on principal cell of CCD
Epithelial sodium channel (ENaC) blockers
Acute kidney injury and chronic kidney disease
↓ Effective arterial blood volume (volume of blood effectively perfusing tissue)
↓ Oxygen perfusion to renal tissue causing renal ischemia
Autonomic neuropathy ↓ sympathetic drive to produce renin
Chronic juxtaglomerular cell damage ↓ synthesis of renin
Blockage of ENaC on the principal cells of the CCD
Angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs)
Angiotensin II is either not formed (ACEi), or blocked at its receptor (ARBs)
Angiotensin II cannot stimulate the release of aldosterone from the adrenal cortex
Adrenal Insufficiency
Adrenal gland cannot produce sufficient amounts of aldosterone
↓ Renin secretion by the afferent arteriole prevents RAAS activation
↓ Aldosterone release from adrenal cortex
↓ ENaC (Na+ reabsorption channel) expression on principal cells of the cortical collecting duct (CCD)
Damage to kidney causes renal impairment and ↓ glomerular filtration rate
↓ Glomerular filtrate production means ↓ tubular flow rate
↓ Na+ delivery to the distal tubule
↓ Na+ reabsorption by ENaCs at the principal cell in CCD
↓ Na+ and water reabsorption by ENaCs in CCD ↓ Effective arterial blood volume (EABV)
Activates renin-angiotensin-aldosterone system (RAAS) leads to ↑ renin secretion in the afferent arteriole (see Physiology of the renin-angiotensin-aldosterone system (RAAS) slide)
↑ Na+ and water loss in tubular lumen
↑ Positive charge in tubular lumen
↓ Electronegativity gradient in tubular lumen
of CCD
↓ K+ excretion by the principal cell in the CCD as there is less of a electronegative gradient
↑ Accumulation of K+ in blood Hyperkalemia
Serum [K+] > 5.1 mmol/L
See Hyperkalemia: Clinical Findings slide
In the case of diabetic nephropathy and NSAIDS ↓ EABV does not stimulate RAAS and therefore aldosterone production
↓ Renin
↓ Aldosterone
↑ Renin secretion activates an ↑ in aldosterone production but aldosterone action at the principal cell is blocked because of ENaCs or resistance in AIN and CIN
↑ Renin
↑ Aldosterone
In the case of ACEi, ARBs, or adrenal insufficiency ↑ renin secretion does not lead to ↑ aldosterone
↑ Renin
↓ Aldosterone
Note: as described in the above flow chart, measuring serum renin and aldosterone levels can be used to help diagnose the cause of hyperkalemia.
Authors: Mannat Dhillon, Joshua Low, Emily Wildman, Huneza Nadeem Reviewers: Andrea Kuczynski, Marissa (Ran) Zhang, Adam Bass*, Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 2, 2022 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2022/08/Hyperkalemia-renal-excretion.jpg "Hyperkalemia (↓ Renal Excretion): Pathophysiology
Non-steroidal anti- inflammatory drugs (NSAIDs)
Inhibition of prostaglandins which promote renin secretion (see NSAIDs and the Kidney: Mechanism of Action and Side Effects slide)
Diabetic Nephropathy
Acute (AIN)and chronic (CIN) interstitial nephritis
Immune-mediated damage of the kidney tubule and interstitium
Damage to distal tubule leads to aldosterone resistance at principal cell
Aldosterone cannot ↑ EnaC insertion on principal cell of CCD
Epithelial sodium channel (ENaC) blockers
Acute kidney injury and chronic kidney disease
↓ Effective arterial blood volume (volume of blood effectively perfusing tissue)
↓ Oxygen perfusion to renal tissue causing renal ischemia
Autonomic neuropathy ↓ sympathetic drive to produce renin
Chronic juxtaglomerular cell damage ↓ synthesis of renin
Blockage of ENaC on the principal cells of the CCD
Angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs)
Angiotensin II is either not formed (ACEi), or blocked at its receptor (ARBs)
Angiotensin II cannot stimulate the release of aldosterone from the adrenal cortex
Adrenal Insufficiency
Adrenal gland cannot produce sufficient amounts of aldosterone
↓ Renin secretion by the afferent arteriole prevents RAAS activation
↓ Aldosterone release from adrenal cortex
↓ ENaC (Na+ reabsorption channel) expression on principal cells of the cortical collecting duct (CCD)
Damage to kidney causes renal impairment and ↓ glomerular filtration rate
↓ Glomerular filtrate production means ↓ tubular flow rate
↓ Na+ delivery to the distal tubule
↓ Na+ reabsorption by ENaCs at the principal cell in CCD
↓ Na+ and water reabsorption by ENaCs in CCD ↓ Effective arterial blood volume (EABV)
Activates renin-angiotensin-aldosterone system (RAAS) leads to ↑ renin secretion in the afferent arteriole (see Physiology of the renin-angiotensin-aldosterone system (RAAS) slide)
↑ Na+ and water loss in tubular lumen
↑ Positive charge in tubular lumen
↓ Electronegativity gradient in tubular lumen
of CCD
↓ K+ excretion by the principal cell in the CCD as there is less of a electronegative gradient
↑ Accumulation of K+ in blood Hyperkalemia
Serum [K+] > 5.1 mmol/L
See Hyperkalemia: Clinical Findings slide
In the case of diabetic nephropathy and NSAIDS ↓ EABV does not stimulate RAAS and therefore aldosterone production
↓ Renin
↓ Aldosterone
↑ Renin secretion activates an ↑ in aldosterone production but aldosterone action at the principal cell is blocked because of ENaCs or resistance in AIN and CIN
↑ Renin
↑ Aldosterone
In the case of ACEi, ARBs, or adrenal insufficiency ↑ renin secretion does not lead to ↑ aldosterone
↑ Renin
↓ Aldosterone
Note: as described in the above flow chart, measuring serum renin and aldosterone levels can be used to help diagnose the cause of hyperkalemia.
Authors: Mannat Dhillon, Joshua Low, Emily Wildman, Huneza Nadeem Reviewers: Andrea Kuczynski, Marissa (Ran) Zhang, Adam Bass*, Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 2, 2022 on www.thecalgaryguide.com")
presentation-of-sah
![Subarachnoid Hemorrhage: Clinical Findings
Sudden bleeding into space surrounding the brain (for pathogenesis, see Subarachnoid Hemorrhage: Pathogenesis)
Authors: Jason An, M. Patrick Pankow Reviewers: Owen Stechishin, Dave Nicholl, Haotian Wang, Hannah Mathew, Ran (Marissa) Zhang, Yan Yu*, Cory Toth* * MD at time of publication
Bleed into subarachnoid space
Subarachnoid Hemorrhage (SAH)
Posterior hypothalamus ischemia (↓ Blood flow and oxygen)
Red blood cell lysis from energy depletion or complement activation
Release of spasmogens (spasm inducing agents)
Cerebral vasospasm (narrowing of arteries from persistent contraction) ↓ blood flow
Cerebral ischemia
Release catecholamines (hormones from the adrenal gland; e.g., epinephrine, norepinephrine)
↑ Intracellular calcium
Release of antidiuretic hormone
Antidiuretic hormone acts on the distal convoluted tubule and collecting duct in kidney to reabsorb water
Dilution of serum sodium
Hyponatremia (low blood sodium levels)
Release of epileptogenic (potential seizure causing agents) into cerebral circulation
Seizure
Products from blood breakdown in cerebral spinal fluid
Irritation of meninges (membranes surrounding the brain)
Aseptic meningitis (non-infectious inflammation)
Meningismus
(neck pain + rigidity)
Cerebral infarction (death of tissue)
Obstructs cerebral spinal fluid flow and absorption at subarachnoid granulations
Hydrocephalus (fluid build up in ventricles)
↓ Level of consciousness
Reduced cerebral blood flow
Dilation of cranial vessels to ↑ blood flow
Rapid ↑ internal carotid artery intracranial pressure
Refer to Increased Intracranial Pressure: Clinical Findings slide
Internal carotid artery
Pituitary ischemia
Hypopituitarism
[underactive pituitary gland, failing to produce 1+ pituitary hormone(s)]
Refer to hypopituitarism slides
Myocardial disruption
Left ventricle dysfunction
↑ Pressure in left heart
Blood forced backwards into pulmonary veins
↑ Pulmonary blood pressure
Fluid from blood vessels leaks into lungs
Dysrhythmias (disturbance in rate/rhythm of heart) causing ↓ cardiac output
Syncope
(loss of consciousness due to ↓ blood flow to the brain)
Pulmonary edema
(excess accumulation of fluid in lung)
Cerebral hypoperfusion
Sudden ↑in blood volume
Vessels and meninges suddenly stretch
Thunderclap Headache (worst headache of patient's life)
Shortness of breath
Reactive cerebral hyperemia (excess blood in vessels supplying the brain)
Artery specific findings:
Rapid ↑ internal carotid artery intracranial pressure
Middle cerebral artery
Posterior communicating artery
Compression of outer CN3 Compression of inner CN3
Anterior communicating artery
Nonreactive pupil
Gaze palsy
(eye deviates down and out)
Diplopia
(double vision)
Ptosis
(drooping of upper eyelid)
Frontal lobe ischemia
Avolition
(complete lack of motivation)
Ischemia of motor strip pertaining to the legs
Bilateral leg weakness
Motor strip ischemia
Hemiparesis
(weakness/ inability to move one side of the body)
Ischemia of parietal association areas (brain regions integral for motor control of the eyes, the extremities and spatial cognition)
Aphasia
(impaired ability to speak and/or understand language)/ neglect
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 1, 2014, updated August 10, 2022 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/SAH-Clinical-Findings-2022.jpg "Subarachnoid Hemorrhage: Clinical Findings
Sudden bleeding into space surrounding the brain (for pathogenesis, see Subarachnoid Hemorrhage: Pathogenesis)
Authors: Jason An, M. Patrick Pankow Reviewers: Owen Stechishin, Dave Nicholl, Haotian Wang, Hannah Mathew, Ran (Marissa) Zhang, Yan Yu*, Cory Toth* * MD at time of publication
Bleed into subarachnoid space
Subarachnoid Hemorrhage (SAH)
Posterior hypothalamus ischemia (↓ Blood flow and oxygen)
Red blood cell lysis from energy depletion or complement activation
Release of spasmogens (spasm inducing agents)
Cerebral vasospasm (narrowing of arteries from persistent contraction) ↓ blood flow
Cerebral ischemia
Release catecholamines (hormones from the adrenal gland; e.g., epinephrine, norepinephrine)
↑ Intracellular calcium
Release of antidiuretic hormone
Antidiuretic hormone acts on the distal convoluted tubule and collecting duct in kidney to reabsorb water
Dilution of serum sodium
Hyponatremia (low blood sodium levels)
Release of epileptogenic (potential seizure causing agents) into cerebral circulation
Seizure
Products from blood breakdown in cerebral spinal fluid
Irritation of meninges (membranes surrounding the brain)
Aseptic meningitis (non-infectious inflammation)
Meningismus
(neck pain + rigidity)
Cerebral infarction (death of tissue)
Obstructs cerebral spinal fluid flow and absorption at subarachnoid granulations
Hydrocephalus (fluid build up in ventricles)
↓ Level of consciousness
Reduced cerebral blood flow
Dilation of cranial vessels to ↑ blood flow
Rapid ↑ internal carotid artery intracranial pressure
Refer to Increased Intracranial Pressure: Clinical Findings slide
Internal carotid artery
Pituitary ischemia
Hypopituitarism
[underactive pituitary gland, failing to produce 1+ pituitary hormone(s)]
Refer to hypopituitarism slides
Myocardial disruption
Left ventricle dysfunction
↑ Pressure in left heart
Blood forced backwards into pulmonary veins
↑ Pulmonary blood pressure
Fluid from blood vessels leaks into lungs
Dysrhythmias (disturbance in rate/rhythm of heart) causing ↓ cardiac output
Syncope
(loss of consciousness due to ↓ blood flow to the brain)
Pulmonary edema
(excess accumulation of fluid in lung)
Cerebral hypoperfusion
Sudden ↑in blood volume
Vessels and meninges suddenly stretch
Thunderclap Headache (worst headache of patient's life)
Shortness of breath
Reactive cerebral hyperemia (excess blood in vessels supplying the brain)
Artery specific findings:
Rapid ↑ internal carotid artery intracranial pressure
Middle cerebral artery
Posterior communicating artery
Compression of outer CN3 Compression of inner CN3
Anterior communicating artery
Nonreactive pupil
Gaze palsy
(eye deviates down and out)
Diplopia
(double vision)
Ptosis
(drooping of upper eyelid)
Frontal lobe ischemia
Avolition
(complete lack of motivation)
Ischemia of motor strip pertaining to the legs
Bilateral leg weakness
Motor strip ischemia
Hemiparesis
(weakness/ inability to move one side of the body)
Ischemia of parietal association areas (brain regions integral for motor control of the eyes, the extremities and spatial cognition)
Aphasia
(impaired ability to speak and/or understand language)/ neglect
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 1, 2014, updated August 10, 2022 on www.thecalgaryguide.com")
patellar-tendon-rupture-pathogenesis-and-clinical-findings

Repetitive activities involving rapid knee flexion and extension
Tendon inflammation and micro-tearing
Fluoroquinolone (antibiotic class) use
Smoking
Immobilization of knee
↓ Muscle and tendon flexibility and strength
Steroid use (including intraarticular injections)
Changes in collagen fibrils composing tendon (exact mechanism unknown)
Disrupted blood supply to tendon and poor healing
Compromised integrity and strength of the tendon
Sudden heavy load on flexed knee while foot is planted
Quadriceps muscles contract while lengthening (eccentric contraction)àforce exceeds tendon strength
Patellar tendon innervated by common peroneal (fibular) nerve
Nociceptors (pain receptors) within tendon activated by tendon rupture
Pain and tenderness below the patella
Collagen fibres in tendon tear
Tearing or popping sensation at time of injury
Patellar Tendon Rupture
Tendon/Ligament detaches from bony attachment on patella or tibial tubercle No connection of quadriceps to tibia via patellar tendon
↑ Force on tibial tubercle during tendon detachment
Avulsion fracture of tibial tubercle
Trauma to tendon ruptures surrounding blood vessels
Coagulation cascade and inflammatory mediators released at rupture site
Quadriceps muscles unable to stabilize patellar tracking
Instability of knee joint
Quadriceps muscle tension pulls patella upwards with no resistance from patellar tendon
Patellar tendon cannot use distal attachment site for leverage
Knee extensor muscles unable to effectively contract
Knee buckling
Abnormal gait
Patella alta
(high sitting patella) on X-ray
Palpable gap below the patella
Bruising below the patella
Swelling below the patella
↑ Risk of falls
Loss of patellar reflex
Inability to perform a straight leg raise (hip flexes and knee cannot remain straight)
Hematoma (blood collection under the skin)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 28, 2022 on www.thecalgaryguide.com")
quadriceps-tendon-rupture-pathogenesis-and-clinical-findings

Quadricep muscles atrophy
↓ Quadricep muscle strength
Smoking
Chronic disease (e.g. renal failure, gout, rheumatoid arthritis, and diabetes)
Fluoroquinolone (antibiotic class) use
Changes in collagen fibrils composing tendonàimpaired tendon strength (exact mechanism unknown)
Quadriceps tendon shortens
↓ Quadricep tendon flexibility
Disrupted blood supply to quadriceps tendon and poor healing
Compromised integrity of the quadriceps tendon and ↓ strength
Sudden heavy load on flexed knee while foot is plantedàquadriceps muscles contract while lengthening (eccentric contraction)
Force on quadriceps tendon exceeds its strength
Quadriceps Tendon Rupture
Tendon detaches from bony attachment on patella
↑ Force on patella during quadriceps tendon detachment
Collagen fibres in quadriceps tendon tear
No connection of quadriceps to tibia via quadriceps tendon
Patellar tendon tension pulls patella downwards with no resistance from quadriceps muscles
Quadriceps tendon innervated by common peroneal (fibular) nerve
Nociceptors (pain receptors) within tendon activated by tendon rupture
Pain and tenderness above the patella
Trauma to tendon ruptures blood vessels
Coagulation cascade and inflammatory mediators released at rupture site
Quadriceps muscles unable to stabilize patellar tracking
Knee joint instability
Patella baja (low sitting patella) on X-ray
Palpable gap above the patella
Loss of patellar reflex
Patellar tendon cannot use proximal attachment site for leverage
Knee extensor muscles unable to effectively contract
Inability to perform a straight leg raise (hip flexes while knee cannot remain straight)
Bruising above the patella
Swelling above the patella
Avulsion fracture of patella
Tearing or popping
sensation at time of injury
Knee buckling
Abnormal gait
↑ Risk of falls
Hematoma (blood collection under the skin)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 2, 2022 on www.thecalgaryguide.com")
unstable-angina-pathogenesis-and-clinical-findings
![Unstable Angina/Unstable Angina Pectoris: Pathogenesis and clinical findings Primary cause:
Secondary causes:
Coronary artery vasospasm - primary or drug induced (Ex: cocaine, triptans)
Coagulopathy
(Ex: antiphospholipid antibody syndrome)
Vasculitic syndromes (Ex: Takayasu arteritis)
Authors: Marisa Vigna Ryan Wilkie Yan Yu* Reviewers: Julena Foglia Davis Maclean Mehul Gupta Andrew Grant* * MD at time of publication
Atherosclerosis
Fatty plaque accumulates inside the intimal walls of arteries Coronary arterial atherosclerotic plaque rupture or erosion
Plaque disruption exposes subendothelial components of damaged vessel wall to platelets, initiating the coagulation cascade and platelet adhesion
Aggregation of platelets results in the formation of a thrombus Thrombus partially occludes blood flow through a coronary artery âmyocardial blood supply
Congenital anomalies (Ex: myocardial bridge, anomalous coronary)
Spontaneous coronary artery dissection
Increased blood viscosity (Ex: polycythemia, thrombocytopenia)
Factors thatámyocardial (cardiac muscle) oxygen demand (Ex: tachycardia, hypotension, hypertension, anemia, exertion, stress)
Coronary embolism (Ex: A. Fib, endocarditis, prosthetic valve thrombus)
áheart rate, contractility, and/or wall tension ámyocardial oxygen demand
Myocardial ischemia due to imbalance between blood supply and oxygen demand (insufficient blood/oxygen supply)
Unstable Angina/Unstable Angina Pectoris
Can be new onset angina; typically progressive in frequency, severity, or duration; can occur at rest
Subtotal occlusion of a coronary arteryà
reduced, but continued, myocardial blood supply
Maintained perfusion means cardiomyocytes are still alive and thus do not leak troponin into bloodstream
Normal serum troponin
Diaphoresis
(sweating)
Since bloodflow occurs from epicardium to endocardium, myocardial ischemia is more
pronounced in the subendocardium (region furthest away from heart’s external surface)
Sufficient blood flow is maintained in regions superficial to the subendocardium, resulting in non-transmural (partial thickness) heart wall ischemia
Non-inferior wall ischemia triggers a predominantáin sympathetic nervous system activity, given the proximity of cardiac sympathetic nerve innervation
Ischemiaâ cardiomyocyte resting membrane potential andâ action potential duration
Voltage gradient between normal and subendocardial ischemic zones creates injury currents, shifting the ST- vector on ECG
ECG: ST depression
and/or T wave inversion
Cardiac sensory nerve fibres mix with somatic sensory nerve
fibres and enter the spinal cord via the T1-T4 nerve roots
Brain perceives increased cardiac sensory nerve signaling as nerve pain coming from the skin of T1-T4 dermatomes (“Referred Pain”)
Myocardial ischemia causes hypoxic stress on cardiomyocytesàâaerobic (requiring oxygen) metabolism,áanaerobic (not requiring oxygen) metabolism
áanerobic respirationálactic acid production,á[H+], andâcellular pH which impairs cardiomyocyte function
Cardiomyocyte dysfunction impairs myocardial relaxation in diastole and/orâ left ventricular contractility in systole
âleft ventricular cardiac output àbackup of blood in the left ventricle, atrium, and pulmonary vasculature
ápulmonary capillary pressures pushes fluid out of the capillaries into the alveoli in the lungs
Fluid filled alveoliâgas exchange andâ oxygenation, triggering harder and faster breathing in order to compensate
Dyspnea
Activation of sweat glands via acetylcholine release
Hormones bind to cardiac β1 receptors
Tachycardia
(áheart rate)
Epinephrine/ Norepinephrine hormone release from the adrenal medulla
Hormones bind to arterial smooth muscle α1 receptors ávascular tone (vasoconstriction)
Hypertension
The Vagus nerve sits in close physical proximity to the inferior wall of the heart àinferior wall ischemia triggers involuntary Vagus nerve activation
Since the Vagus nerve coordinates parasympathetic activity,áVagus nerve activity leads to a variety of parasympathetic nervous system responses:
Retrosternal discomfort: May present as pain, heaviness, tightness, aching, pressure, burning or squeezing
Pain radiation to T1-T4 dermatomes:
Left shoulder and arm, lower jaw, neck, abdomen, upper back
Syncope
(fainting)
Bradycardia
Nausea Hypotension
(âheart rate)
(âblood pressure)
(áblood pressure)
(shortness of breath)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Findings
Complications
Published Oct 18, 2015, updated Aug 29, 2021 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2015/10/Unstable-Angina-2021.jpg "Unstable Angina/Unstable Angina Pectoris: Pathogenesis and clinical findings Primary cause:
Secondary causes:
Coronary artery vasospasm - primary or drug induced (Ex: cocaine, triptans)
Coagulopathy
(Ex: antiphospholipid antibody syndrome)
Vasculitic syndromes (Ex: Takayasu arteritis)
Authors: Marisa Vigna Ryan Wilkie Yan Yu* Reviewers: Julena Foglia Davis Maclean Mehul Gupta Andrew Grant* * MD at time of publication
Atherosclerosis
Fatty plaque accumulates inside the intimal walls of arteries Coronary arterial atherosclerotic plaque rupture or erosion
Plaque disruption exposes subendothelial components of damaged vessel wall to platelets, initiating the coagulation cascade and platelet adhesion
Aggregation of platelets results in the formation of a thrombus Thrombus partially occludes blood flow through a coronary artery âmyocardial blood supply
Congenital anomalies (Ex: myocardial bridge, anomalous coronary)
Spontaneous coronary artery dissection
Increased blood viscosity (Ex: polycythemia, thrombocytopenia)
Factors thatámyocardial (cardiac muscle) oxygen demand (Ex: tachycardia, hypotension, hypertension, anemia, exertion, stress)
Coronary embolism (Ex: A. Fib, endocarditis, prosthetic valve thrombus)
áheart rate, contractility, and/or wall tension ámyocardial oxygen demand
Myocardial ischemia due to imbalance between blood supply and oxygen demand (insufficient blood/oxygen supply)
Unstable Angina/Unstable Angina Pectoris
Can be new onset angina; typically progressive in frequency, severity, or duration; can occur at rest
Subtotal occlusion of a coronary arteryà
reduced, but continued, myocardial blood supply
Maintained perfusion means cardiomyocytes are still alive and thus do not leak troponin into bloodstream
Normal serum troponin
Diaphoresis
(sweating)
Since bloodflow occurs from epicardium to endocardium, myocardial ischemia is more
pronounced in the subendocardium (region furthest away from heart’s external surface)
Sufficient blood flow is maintained in regions superficial to the subendocardium, resulting in non-transmural (partial thickness) heart wall ischemia
Non-inferior wall ischemia triggers a predominantáin sympathetic nervous system activity, given the proximity of cardiac sympathetic nerve innervation
Ischemiaâ cardiomyocyte resting membrane potential andâ action potential duration
Voltage gradient between normal and subendocardial ischemic zones creates injury currents, shifting the ST- vector on ECG
ECG: ST depression
and/or T wave inversion
Cardiac sensory nerve fibres mix with somatic sensory nerve
fibres and enter the spinal cord via the T1-T4 nerve roots
Brain perceives increased cardiac sensory nerve signaling as nerve pain coming from the skin of T1-T4 dermatomes (“Referred Pain”)
Myocardial ischemia causes hypoxic stress on cardiomyocytesàâaerobic (requiring oxygen) metabolism,áanaerobic (not requiring oxygen) metabolism
áanerobic respirationálactic acid production,á[H+], andâcellular pH which impairs cardiomyocyte function
Cardiomyocyte dysfunction impairs myocardial relaxation in diastole and/orâ left ventricular contractility in systole
âleft ventricular cardiac output àbackup of blood in the left ventricle, atrium, and pulmonary vasculature
ápulmonary capillary pressures pushes fluid out of the capillaries into the alveoli in the lungs
Fluid filled alveoliâgas exchange andâ oxygenation, triggering harder and faster breathing in order to compensate
Dyspnea
Activation of sweat glands via acetylcholine release
Hormones bind to cardiac β1 receptors
Tachycardia
(áheart rate)
Epinephrine/ Norepinephrine hormone release from the adrenal medulla
Hormones bind to arterial smooth muscle α1 receptors ávascular tone (vasoconstriction)
Hypertension
The Vagus nerve sits in close physical proximity to the inferior wall of the heart àinferior wall ischemia triggers involuntary Vagus nerve activation
Since the Vagus nerve coordinates parasympathetic activity,áVagus nerve activity leads to a variety of parasympathetic nervous system responses:
Retrosternal discomfort: May present as pain, heaviness, tightness, aching, pressure, burning or squeezing
Pain radiation to T1-T4 dermatomes:
Left shoulder and arm, lower jaw, neck, abdomen, upper back
Syncope
(fainting)
Bradycardia
Nausea Hypotension
(âheart rate)
(âblood pressure)
(áblood pressure)
(shortness of breath)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Findings
Complications
Published Oct 18, 2015, updated Aug 29, 2021 on www.thecalgaryguide.com")
type-ii-proximal-renal-tubular-acidosis-pathogenesis-and-laboratory-findings
 Zhang, Julian Midgley* * MD at time of publication
Overview of bicarbonate reabsorption in the proximal tubule (PT):
Serum bicarbonate (HCO3-) is filtered by the glomerulus and enters PT lumen
H+ ATPase and sodium- hydrogen exchanger 3
(NHE3) on luminal surface of PT cell secrete H+ into PT lumen
H+ combines with HCO3- in
PT lumen to form carbonic acid (H2CO3)
H2CO3 is broken down to H2O and CO2 by luminal membrane carbonic anhydrase 4
CO2 diffuses into PT cell
CO2 reacts with H2O to form H2CO3 in PT cell, catalyzed by cytosolic carbonic anhydrase 2
H2CO3 rapidly breaks down intracellularly to form HCO3- and H+
HCO3- is reabsorbed into plasma by sodium
bicarbonate transporter (NBCE1) on basolateral surface of PT cell
HCO3- is available for use to buffer plasma H+
H+ is available intracellularly for use by H+ ATPase and NHE3 exchanger
Mutation encoding NHE3 exchanger
↓ H+ secretion into PT lumen
Galactosemia, Wilson disease, cystinosis, tyrosinemia, glycogen storage disorders
Dent disease, Lowe syndrome
Infiltrative disorders
e.g., amyloidosis, multiple myeloma, monoclonal gammopathies
Drugs
e.g., tenofivir, ifosfamide, cisplatin
Carbonic anhydrase inhibitors
↓ H2CO3 breakdown to H2O and CO2
Mutation encoding CAII enzyme, carbonic anhydrase inhibitors
↓ H2CO3 production in PT lumen
↓ CO2 diffusion into PT cell
↓ H2CO3 production in PT cell
↓ HCO3- production in PT cell
↓ HCO3- reabsorption by PT cell into plasma
Type II/Proximal Renal Tubular Acidosis (RTA)
Defective HCO3- reabsorption in proximal tubule
Normal anion gap metabolic acidosis (NAGMA)
See NAGMA slide
Accumulation of toxic metabolites systemically, including in the PT
Disruption of endocytosis and intracellular transport systemically, including in the PT
Accumulation of light chain/amyloid deposits in PT
Interfere with PT’s ability to reabsorb ions/molecules
• • • •
Fanconi Syndrome:
generalized PT dysfunction
Defective tubular reabsorption of other ions/molecules to varying
degrees, including phosphate, glucose, sodium and amino acids
Tubular proteinuria Phosphaturia
Glucosuria
↑ Na+ secretionàhypovolemia
Mutation encoding NBCE1 transporter
↑ HCO3- delivery to distal nephron
K+ in distal nephron lumen binds to HCO3-
K+ is lost through osmotic diuresis
Hypokalemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 24, 2022 on www.thecalgaryguide.com")
Granulomatosis with Polyangiitis Pathogenesis

Environmental exposures
Silica dust, cigarette smoke, infections (Staphylococcus aureus)
Genetic factors
Alpha-1 antitrypsin deficiency, proteinase 3 gene mutation
↑ Production of cytokines and antineutrophil cytoplasmic antibodies (ANCAs) (mechanism unknown) Cytokines bind to endothelial cells (that line blood vessels) and neutrophils, priming them
Proteinase 3 (PR3), an enzyme that degrades extracellular matrix proteins, migrates from neutrophil granules to neutrophil cell surface
Circulating ANCAs bind to PR3 on neutrophils
PR3 stimulates maturation of dendritic cells in lungs
Dendritic cells present antigen (PR3) to naïve CD4+ T cells in peripheral lymph nodes
T cells differentiate into type 1 and type 17 helper T cells (Th1 and Th17 cells)
Th1 and Th17 cells secrete cytokines (interferon γ (INF-γ) and tumor necrosis factor α (TNF-α)) in lungs
Secreted cytokines trigger macrophage maturation
Formation of granulomas (giant cells with central necrosis surrounded by plasma cells, lymphocytes, and dendritic cells) primarily in lungs and upper airways
ANCA-activated neutrophils release proinflammatory cytokines, attracting more neutrophils to endothelium (blood vessel wall)
ANCA-activated neutrophils undergo firm adhesion to endothelium
ANCAs stimulate ↑ secretion of proteolytic enzymes and reactive oxygen species from neutrophils
Endothelial damage and tissue injury
Granulomatosis with polyangiitis (GPA)
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms with involvement of multiple organ systems
(see slide on clinical findings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com
Granulomatosis with polyangiitis: Clinical findings Inflammation-mediated endothelial damage and granuloma formation
(see slide on pathogenesis)
Granulomatosis with polyangiitis (GPA)
Author:
Oswald Chen
Reviewers:
Ben Campbell
*Liam Martin
* MD at time of publication
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms
Fever, unintentional weight loss, night sweats, arthralgias
Skin involvement
Inflammation of cutaneous vessels
Systemic inflammation obstructing blood flow, with granulomatous lesions primarily in upper airways and lungs
Ear, nose, and throat involvement
↑ C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) (markers of inflammation)
Necrotizing granulomas on biopsy of affected tissue
Positive PR3-ANCA/c-ANCA blood test (antibodies present in ~90% of patients, described in GPA Pathogenesis slide)
Renal involvement
Inflammation of renal vessels
Rupture of basement membrane (layer that filters blood from glomerular capillaries into Bowman’s capsule)
Pauci-immune glomerulonephritis (see Nephritic Syndrome slide)
Rapidly progressive glomerulonephritis
Eye involvement
Inflammation of ocular tissue
Conjunctivitis
Scleritis/ episcleritis (painful red eye)
Lower respiratory tract involvement
Inflammation of pulmonary vessels
Vessel occlusion and ischemia
Skin necrosis
Vessels burst and blood pools under skin
Round and retiform (net- like) palpable purpura of lower extremities
Granulomatous destruction of nasal cartilage
Collapse of nasal bridge
Saddle nose deformity
Inflammation of paranasal sinus and nasal cavity vessels
↓ Perfusion of lungs
Dyspnea
Damage to interstitial capillaries
Hemoptysis
Diffuse alveolar hemorrhage
Rhinitis/ sinusitis
Granulomatous obstruction of eustachian tube
Otitis media (see Otitis Media slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com")
Granulomatosis with polyangiitis: Clinical findings

Granulomatosis with polyangiitis (GPA)
Author:
Oswald Chen
Reviewers:
Ben Campbell
*Liam Martin
* MD at time of publication
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms
Fever, unintentional weight loss, night sweats, arthralgias
Skin involvement
Inflammation of cutaneous vessels
Systemic inflammation obstructing blood flow, with granulomatous lesions primarily in upper airways and lungs
Ear, nose, and throat involvement
↑ C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) (markers of inflammation)
Necrotizing granulomas on biopsy of affected tissue
Positive PR3-ANCA/c-ANCA blood test (antibodies present in ~90% of patients, described in GPA Pathogenesis slide)
Renal involvement
Inflammation of renal vessels
Rupture of basement membrane (layer that filters blood from glomerular capillaries into Bowman’s capsule)
Pauci-immune glomerulonephritis (see Nephritic Syndrome slide)
Rapidly progressive glomerulonephritis
Eye involvement
Inflammation of ocular tissue
Conjunctivitis
Scleritis/ episcleritis (painful red eye)
Lower respiratory tract involvement
Inflammation of pulmonary vessels
Vessel occlusion and ischemia
Skin necrosis
Vessels burst and blood pools under skin
Round and retiform (net- like) palpable purpura of lower extremities
Granulomatous destruction of nasal cartilage
Collapse of nasal bridge
Saddle nose deformity
Inflammation of paranasal sinus and nasal cavity vessels
↓ Perfusion of lungs
Dyspnea
Damage to interstitial capillaries
Hemoptysis
Diffuse alveolar hemorrhage
Rhinitis/ sinusitis
Granulomatous obstruction of eustachian tube
Otitis media (see Otitis Media slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com")
hypovolemic-shock

Inflammation (pancreatitis, cirrhosis, post-operative, etc.)
Inflammatory mediators vessel permeability and fluid leaks out
Trauma
Ruptured vessels leak fluid into potential spaces
Hemorrhagic losses
(GI bleed, postpartum hemorrhage, etc.)
↓ Intravascular volume
↓ Venous return to the heart
↓ Cardiac output (blood pumped from the heart)
Hypovolemic Shock
↓ Oxygen delivery to tissues due to low blood volume
Insufficient organ perfusion
Non-Hemorrhagic losses
(dehydration, GI losses, skin losses / burns, renal losses, etc.)
‘Third Spacing’ of fluid
(fluid located outside the intravascular or intracellular space; large collections can occur in the pelvis, thorax, GI tract, long bones of children, intra-abdominally, retroperitoneally)
P = Q x R; less ‘flow’ in the vessels (Q), with vessels not constricting enough to maintain resistance (R)à pressure (P) will drop
↓ Blood Pressure
Caution: young, healthy individuals can maintain blood pressure during circulatory collapse with cardiac output and vasoconstriction; do not use blood pressure as an indicator of shock severity in children
Carotid sinus baroreceptors sense low blood pressure ↓ Carotid sinus inhibition of sympathetic nervous system Release of sympathetic catecholamines (epinephrine and
↓ Pressure in venous circulation
Brain
Heart
Kidneys
↓ Blood in the right internal jugular vein
↓ Oxygen delivery to the brain
↓ Myocardial contractility (from lactic acidosis)
↓ Blood flow to kidneys
↓ Jugular Venous Pressure
Catecholamines bind to beta-1 receptors in the sinoatrial node of the heart
Beta-1 receptor activation causes ↑ heart rate
Tachycardia
norepinephrine)
Catecholamines bind to and stimulate alpha-1 receptors in peripheral vessels
Vasoconstriction of peripheral vessels
↓ Blood flow to peripheral tissue
Catecholamines bind to and stimulate beta receptors in sweat glands
Diaphoresis
(sweating)
In all body tissues
Inadequate oxygen delivery
↓ ATP production
↑ Anaerobic metabolism
↓ Body temperature
Impaired neurological functioning
Renal ischemia
Activation of the renin-angiotensin aldosterone system
↓ Glomerular filtration rate
↓ Clearance of lactic acid by the kidney
↑ Lactic acid production
↓ Rate of activity of clotting enzymes
Lactic Acidosis
Unknown mechanism
Coagulopathy Hypothermia
Trauma Triad of Death
↑ Capillary Cold, mottled refill time extremities
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 24, 2013, updated December 4, 2022 on www.thecalgaryguide.com")
Approach to Arterial Blood Gases ABGs

Normal pO2 should be FiO2 x 4-5
(FiO2 in room air= 21%)
pH >7.40 = Alkalemia
1. Adequate oxygenation?
2. Define the acid-base disturbance
Diarrhea (Loss of electrolytes not reabsorbed through bowel)
Normal ABG on Room Air = 7.40 / 40 / 90 / 24
pO2 ↓ than expected
Possible hypoxemia
See slide on
Hypoxemia: Pathogenesis and Clinical Findings
(pH)
(Loss of acidic fluids from stomach)
(HCO3-)
(pCO2)
(pO2)
Renal Tubular Acidosis (RTA)
pH <7.40 = Acidemia
Metabolic derangement (Due to poisons, infection, or ketones)
Gain of acid (H+)
Brain unable to promote respiratory drive
(ex. drugs, trauma)
Inability for chest wall to expand (ex. obesity, neuromuscular weakness, pleural or chest wall abnormalities)
Vomiting or
nasogastric
suction
Impaired tubular transport of H+
(Due to loop/thiazide diuretics, hypomagnesemia, congenital abnormalities)
1o Hyperaldosteronism =
↑ H+ ion secretion at
distal tubule
(Due to tumours, congenital abnormalities , malignant hypertension, etc)
Type II RTA = HCO3- not reabsorbed
Type I or IV RTA = H+ not secreted
GI or renal loss of HCO3-
Hypoventilation
↑ CO2 from ↓ exhalation Respiratory Acidosis Acute= ↑10:↑1, Chronic= ↑10:↑3
GI or renal loss of acid (H+)
↑ HCO3- from ↓ H+ to bind with Metabolic Alkalosis ↑7:↑10
↑ Ventilation from stress, trauma, infection
↓ CO2 from ↑ exhalation Respiratory Alkalosis Acute= ↓10:↓2, Chronic= ↓10:↓4
3. Identify the primary (1o) process
4. Compensatory mechanisms in lungs and kidneys attempt to lose/retain CO2 or HCO3- to maintain normal pH. Determine if compensation is appropriate (approximate normal ratio of change in pCO2 : HCO3- is shown in green boxes). If inappropriate, there is a secondary (2o) process occurring
HCO3- binds with extra H+
↓ HCO3- Metabolic Acidosis ↓12 :↓10
Less CO2 than expected, due to ↑ exhalation = Less acid in serum
2o Respiratory alkalosis
More CO2 than expected, due to ↓ exhalation = More acid in serum
2o Respiratory acidosis
Less HCO3- than expected, due to 2o gain of H+ or loss of HCO3-
2o Metabolic acidosis
More HCO3- than expected, due to 2o loss of H+
2o Metabolic alkalosis
Less CO2 than expected, due to ↑ exhalation = Less acid in serum
2o Respiratory alkalosis
↑ CO2 than expected, due to ↓ exhalation = More acid in serum
2o Respiratory acidosis
Less HCO3- than expected, due to 2o gain of H+ or loss of HCO3-
2o Metabolic acidosis
More HCO3- than expected, due to 2o loss of H+
2o Metabolic alkalosis
5. Calculate anion gap (AG) to determine the presence and type of metabolic acidosis. This is done regardlessofthe1o or2oprocess, as there may also be a hidden metabolic acidosis
6. HAGMA only: In normal blood buffer system, acid gain should match bicarbonate lost. If not, identify if another process is causing an inappropriate loss or gain of HCO3-
Gain of acid (∆AG) = AG-12 LossofHCO3- (∆HCO3-)=24-HCO3-
7. Calculate Osmolar Gap (for HAGMA) or Urine net charge (for NAGMA) to narrow the etiology
Authors:
Sravya Kakumanu
Reviewers:
Huneza Nadeem, Ben Campbell *Adam Bass, *Yan Yu
* MD at time of publication
(normal is ~12)
Calculate AG = Na+- Cl- - HCO3-
If a metabolic acidosis is present, ↓ HCO3- is
compensatedby↑otherserumanionstomaintain neutral charge
If no metabolic acidosis was identified in steps 2-4:
No Metabolic acidosis present
Classically, the compensating anion is Cl-,maintaininganormalAG
AG ≤ 12
If a 1o or 2o metabolic acidosis was identified in steps 2-4:
Normal Anion Gap Metabolic Acidosis (NAGMA)
In this scenario, a normal distal nephron should be excreting excess acid
Excess acid is normally excreted as ammonium (NH +) with Cl- 4
The more Cl- in the urine relative to cations, the more acid is being excreted Calculate urine (U) net charge to determine cause of NAGMA = UNa+ + UK+ - UCl-
When the cause is addition of an abnormal acid, HCO3- is used up asabuffer,andthecompensatinganionistheabnormalacid's conjugate base – which is not measured in the AG calculation
↓ HCO3- is compensated by unmeasured anionsà the AG ↑ AG>12
High Anion Gap Metabolic Acidosis (HAGMA)
Calculate ∆AG = AG-12
Calculate ∆HCO3- = 24-HCO3-
∆HCO3- > ∆AG
Loss of HCO3- > Gain of acid
Additional process causing further loss of HCO3-
HAGMA + NAGMA
∆HCO3- = ∆AG
Loss of HCO3- = Gain of acid
Only acid gain from HAGMA causing HCO3- loss
HAGMA only
∆HCO3- < ∆AG
Loss of HCO3- < Gain of acid
Additional process causing gain of HCO3- despite losses due to HAGMA
HAGMA + Metabolic alkalosis
See slide on
Metabolic Alkalosis: Pathogenesis
-ve U net charge Appropriately large Cl- excretionà
Toxic alcohol ingestion ↑ serum osmolality (and H+) from metabolites produced, so osmolality helps identify etiology
Calculate osmolar gap to determine cause of HAGMA
= (measured serum osm) – (expected serum osm)
= (measured serum osm) – (2(Na+) + urea + serum glucose)
+ve U net charge
Inappropriately small Cl- excretionà impaired acid excretion is the issue
Type IV or Type I RTA See slide on Normal Anion Gap Metabolic Acidosis: Pathogenesis and Laboratory Findings
HCO3
GI losses or Type II RTA
-
loss is the issue
Osmolar gap > 10 (extra osmoles present)
Toxic alcohol poisoning
Osmolar gap ≤10 (normal)
Test for other causes
See slide on High Anion Gap Metabolic Acidosis: Pathogenesis and Laboratory Findings
Legend:
Disease State
Mechanism
Lab Finding/Calculation
Published January 29, 2023 on www.thecalgaryguide.com")
Coronary Artery Bypass Graft CABG Indications
: Indications
Author: Breanne Gordulic Reviewers: Miranda Schmidt Ben Campbell Sunawer Aujla Angela Kealey* * MD at time of publication
Symptomatic multivessel (≥ 3 vessels) coronary artery disease (MVCAD) or complex MVCAD
Acute coronary syndrome (ACS)
Left main coronary artery disease
Multivessel (≥ 3 vessels) CAD and diabetes
Cardiac surgery required for other pathology
Multivessel CAD, LV dysfunction and congestive heart failure (CHF)
Complex CAD includes stenosed vein grafts, bifurcation lesions, calcified lesions, total occlusions, ostial lesions
STEMI initial treatment is PCI/thrombolysis
CABG outcomes compared to percutaneous coronary intervention (PCI) in MVCAD include ↑ survival in diabetes, ↑ survival with LV dysfunction, ↓ repeat revascularization, ↓ myocardial infarction, ↓ stroke
↑ Risk of failure in complex CAD with PCI
Rapid reperfusion to myocardium most important in STEMI to decrease myocardial damage
CABG can be considered for residual stenoses 6-8 weeks later
NSTEMI or unstable angina (UA) with MVCAD involving at least three vessels including the proximal left anterior descending (LAD)
Left main coronary artery divides into left anterior descending (LAD) and left circumflex (LCx) which supplies 2/3 of myocardium
↑ Survival Myocardial infarction from left main artery occlusion Death
Left main stenosis
Ventricular dysrhythmias
Ongoing ischemia
LV dysfunction Hemodynamic instability
↑ risk of PCI
CABG has mortality benefit
↓ Number of operations
↑ Risk of cardiovascular disease in diabetes
Revascularization indicated along with other cardiac surgery
Multivessel CAD with >90% stenosis and CHF
LV ejection fraction <35%
↑ Risk of atherosclerosis from hyperglycemia and dyslipidemia
CABG bypasses several atherosclerotic plaques in coronary arteries
↑ Durability
↑ Complete perfusion
Valve stenosis or regurgitation Septal defect
Aortic root or arch pathology
Combination procedure
Evidence of ischemia at rest
Evidence of
impaired LV function at rest
↓ All-cause mortality in CABG vs medical management
Chronic obstructive pulmonary disease
Abbreviations:
• ACS- acute coronary syndrome. Acute reduction in
blood flow to heart muscle resulting in cell death. • CAD- coronary artery disease. Narrowing or blockage of the coronary arteries by plaque
• NSTEMI- myocardial infarction (heart attack) with no ST elevation on electrocardiogram
• PCI- percutaneous coronary intervention. A balloon tipped catheter is used to open blocked coronary arteries; a stent may be placed.
• STEMI- myocardial infarction with ST segment elevation on electrocardiogram
Consider revascularization (restore blood flow to blocked or narrowed blood vessels) of coronary arteries to increase perfusion to myocardium (heart muscle)
Coronary artery bypass graft recommended
Assess surgical risk and comorbidities with evaluation by heart team that includes both a cardiac surgeon and interventional cardiologist (SYNTAX Trial)
Individual management plan for patients with comorbidities that increase mortality
Frailty
Chronic Renal Failure
↑ Inflammation and deregulated angiogenesis affects all organ systems
↓ Physiologic reserve and ↓ ability to recover from acute stress
↑ Pneumonia
↑ Respiratory and Renal Failure
↑ Stroke
↑ In hospital mortality
↓ Survival two years after surgery
Use Society of Thoracic Surgeons Score, EuroSCORE, or SYNTAX II Score to predict patient outcome with anatomy, disease severity, and preoperative characteristics
Coronary Artery Bypass Graft
Surgery to take healthy blood vessels from the body and connect them proximally and distally to blocked coronary arteries
Cardiopulmonary bypass, fluid overload, ↑ renal vasoconstriction and ↓ renal oxygenation from rewarming
Kidney injury
↑ End stage kidney disease
Blood flow restored to
ischemic myocardium
↓ Angina
↑ Quality of life ↑ LV function ↑ Survival
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 12, 2023 on www.thecalgaryguide.com")
normal neonatal changes pathogenesis and clinical findings
.
Authors: Erin Auld, Dasha Mori Reviewers: Kayla Feragen Mao Ding Danielle Nelson* *MD at time of publication
Birth weight: Loss of birth weight up to 10%; should be re-gained within 10-14 days (30 g/day)
Stool: transitions from meconium (first stool of neonate that is black, tarry and sticky) to normal (green/brown or yellow mustard) within 2-3 days
Meconium passage: within 24 hours of birth
Growth
• Height: 2.5 cm/month
• Head Circumference: Average 1 cm/month in the first year with greatest growth in the first month • Weight: 20-30 g/day for the first 3 months
Urination: within the first 24 hours
Mother receives intravenous fluids during delivery
Colostrum (first milk secretion that contains antibodies) produced in first 2-3 days of lactation post-partum (Lactogenesis I)
GI tract maturation
Adequate dietary intake
Maturation of urinary tract
Adequate fluid intake
↑ maternal blood volume
Fluid moves between fetus and mother through placenta
Fetus’s fluid volume ↑
Infant’s urine output ↑ in first 24 hours post-partum
Low breast milk intake in first 2-3 days
↓ progesterone, ↑ prolactin in mother at birth
Infant ingests colostrum
Mostly water loss, some fat loss
↑ Breast Milk Production (Lactogenesis II)
Stomach stretches
↑ in gastrointestinal tract motility (gastrocolic reflex)
Ingestion of milk post-partum further stimulates GI maturation
110-120 kilocalories/kg/day
Gastrointestinal tract formation begins when the fetus is 4 weeks old. Maturation continues into infancy.
Normal gestational age (38-42 weeks)
Fetus ingests amniotic fluid in utero
Stimulates structural changes, enzymatic activity, and metabolic activity of GI tract
Mature detrusor sphincter complex, appropriate bladder capacity, proper renal perfusion, and regular arousal of the neonate
Breast milk: Feeding when infant demands it, approximately every 2-3 hours Formula: Feeding when infant demands it, approximately every 4 hours
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 24, 2015, updated Sept 28, 2023 on www.thecalgaryguide.com")
Alcohol Withdrawal Syndrome
: Pathophysiology & clinical findings
Authors: Rupali Manek Gurreet Bhandal Erika Russell Reviewers: Harjot Atwal Yvette Ysabel Yao Mao Ding Nureen Pirbhai* * MD at time of publication
Chronic alcohol use
↓Autonomic adrenergic systems
↓ Dopamine in the nucleus accumbens
↑ EtOH depressant effects on brain
↓ Glutamate- induced excitation
↑ GABA-induced inhibition
↑ Glutamate receptors in attempt to maintain normal arousal state
GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
Long-term physical dependence
Abrupt alcohol cessation àabrupt ↓ in blood EtOH concentration
Alcohol withdrawal Syndrome
Symptoms that occur when patients stop drinking or significantly decrease their alcohol intake after long-term dependence
↓ GABA-induced inhibition &↑ glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
↑ Autonomic adrenergic systems (rebound over-activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑ Heart rate (HR), ↑respiratory rate (RR) ↑blood pressure (BP), tremor & diaphoresis (↑sweating)
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations 6-12 hours after alcohol cessation
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals 12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (mostly visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Hypovolemia
(from diaphoresis, hyperthermia, vomiting, ↑RR & ↓oral intake)
Metabolic acidosis
(from hypoperfusion, infection, alcoholic ketoacidosis, or ↓
thiamine & other B vitamins)
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Phosphate
(from malnutrition)
Cardiac failure, rhabdomyolysis or muscle breakdown
↓ Phosphate available to make ATP
↓ ATP
↓ Magnesium (common in patients with DT)
Impaired Na-K ATPase function
Dysrhythmias
↑ Glutamate-activated depolarization in the brain
↑ Neuronal excitability
Seizures
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Apr 15, 2017, updated Oct 18, 2023 on www.thecalgaryguide.com
Alcohol Withdrawal Syndrome (AWS): Pathophysiology & clinical findings
Authors: Rupali Manek Gurreet Bhandal Erika Russell Reviewers: Harjot Atwal Yvette Ysabel Yao Mao Ding Nureen Pirbhai* * MD at time of publication
Chronic alcohol use
↓Autonomic adrenergic systems
↓ Dopamine in the nucleus accumbens
↑ EtOH depressant effects on brain
↓ Glutamate- induced excitation
↑ GABA-induced inhibition
↑ Glutamate receptors in attempt to maintain normal arousal state
GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
Long-term physical dependence
Abrupt alcohol cessation àabrupt ↓ in blood EtOH concentration
Alcohol withdrawal Syndrome
Symptoms that occur when patients stop drinking or significantly decrease their alcohol intake after long-term dependence
↓ GABA-induced inhibition &↑ glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
↑ Autonomic adrenergic systems (rebound over-activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑ Heart rate (HR), ↑respiratory rate (RR) ↑blood pressure (BP), tremor & diaphoresis (↑sweating)
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations 6-12 hours after alcohol cessation
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals 12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (mostly visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Hypovolemia
(from diaphoresis, hyperthermia, vomiting, ↑RR & ↓oral intake)
Metabolic acidosis
(from hypoperfusion, infection, alcoholic ketoacidosis, or ↓ thiamine & other B vitamins)
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Magnesium (common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate
(from malnutrition)
↓ Phosphate available to make ATP
↓ ATP
Cardiac failure, rhabdomyolysis or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Alcohol Withdrawal: Pathophysiology & clinical findings
Authors: Erika Russell Rupali Manek Gurreet Bhandal Reviewers: Yvette Ysabel Yao Harjot Atwal Nureen Pirbhai* * MD at time of publication
↓Autonomic adrenergic systems
↓ Glutamate-induced excitation
Chronic alcohol use
↑ EtOH depressant effects on brain
↓ Dopamine in the nucleus accumbens
↑ GABA-induced inhibition
↑ Glutamate receptors in attempt to maintain normal arousal state GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
↑ Autonomic adrenergic systems (rebound over- activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑ Heart rate (HR), ↑respiratory rate (RR) ↑blood pressure (BP), tremor & diaphoresis (↑sweating)
Physical dependence due to chronic alcohol use
Abrupt alcohol cessation
Abrupt ↓ in blood EtOH concentration
Alcohol withdrawal
↓ GABA-induced inhibition &↑ glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals
12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations 6-12 hours after alcohol cessation
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (mostly visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Hypovolemia (from diaphoresis, hyperthermia, vomiting,
↑RR & ↓oral intake)
Metabolic acidosis (from
hypoperfusion, infection, alcoholic ketoacidosis, or ↓ thiamine & other B vitamins)
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Magnesium (common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate (from malnutrition)
↓ Phosphate available to make ATP
↓ ATP
Cardiac failure, rhabdomyolysis or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Authors: Erika Russell Rupali Manek Gurreet Bhandal Reviewers: ↓Autonomic adrenergic systems ↓ Dopamine in the nucleus accumbens Yvette Ysabel Yao Harjot Atwal Nureen Pirbhai* * MD at time of publication
Alcohol Withdrawal: Pathophysiology & clinical findings Chronic alcohol use
↑ EtOH depressant effects on brain
↓ Glutamate-induced excitation ↑ GABA-induced inhibition
↑ Glutamate receptors in attempt to maintain normal arousal state GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
↑ Autonomic adrenergic systems (rebound over- activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑ Heart rate (HR), ↑respiratory rate (RR) ↑blood pressure (BP), tremor & diaphoresis (↑sweating)
Physical dependence due to chronic alcohol use
Abrupt alcohol cessation
Abrupt ↓ in blood EtOH concentration Alcohol withdrawal
↓ GABA-induced inhibition &↑ Glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals
12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (mostly visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations 6-12 hours after alcohol cessation
Hypovolemia (from diaphoresis, hyperthermia, vomiting, ↑RR & ↓oral intake)
Metabolic acidosis (from
hypoperfusion, infection, alcoholic ketoacidosis, or ↓ thiamine & other B vitamins)
↓ Magnesium (common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate (from malnutrition) Cardiac failure, rhabdomyolysis
or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Alcohol Withdrawal: Pathophysiology & clinical findings Chronic alcohol use
↓ Dopamine in the nucleus accumbens ↓Autonomic adrenergic systems
Authors: Erika Russell Rupali Manek Gurreet Bhandal Reviewers: Yvette Ysabel Yao Harjot Atwal ↑ GABA-induced inhibition Nureen Pirbhai* * MD at time of publication
↑ EtOH depressant effects on brain
↓ Glutamate-induced excitation
↑ Glutamate receptors in attempt to maintain normal arousal state
GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
↑ Autonomic adrenergic systems (rebound over- activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑Heart rate (HR), ↑respiratory rate (RR) ↑blood pressure (BP), tremor & diaphoresis (↑sweating)
Physical dependence due to chronic alcohol use
Abrupt alcohol cessation
Abrupt ↓ in blood EtOH concentration Alcohol withdrawal
↓ GABA-induced inhibition &↑ Glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals
12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (mostly visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations 6-12 hours after alcohol cessation
Hypovolemia (from diaphoresis, hyperthermia, vomiting, ↑RR & ↓oral intake)
Metabolic acidosis (from
hypoperfusion, infection, alcoholic ketoacidosis, or ↓ thiamine & other B vitamins)
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Magnesium
(common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate (from malnutrition)
Cardiac failure, rhabdomyolysis or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Alcohol Withdrawal: Pathophysiology & clinical findings
Authors: Erika Russell Rupali Manek Gurreet Bhandal Reviewers: Yvette Ysabel Yao Harjot Atwal Nureen Pirbhai* * MD at time of publication
↑ EtOH depressant effects on brain
↓ Glutamate-induced excitation
↑ Glutamate receptors in attempt to maintain normal arousal state
Chronic alcohol use
↑ GABA-induced inhibition
GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
↓ Dopamine in the nucleus accumbens ↓Autonomic adrenergic systems
Abrupt alcohol cessation
Physical dependence due to chronic alcohol use
Alcohol withdrawal
↓ GABA-induced inhibition &↑ Glutamate-induced excitation relative to chronic alcohol use
Central nervous system overactivity
Withdrawal seizures: Generalized tonic-clonic convulsions 24-48 hours after alcohol cessation
↑ Autonomic adrenergic systems (rebound over-activity of the brain and noradrenergic systems)
↑ Sympathetic activity: ↑HR, ↑RR ↑BP, tremor & diaphoresis (↑sweating)
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations
6-12 hours after alcohol cessation
↑ Dopamine in nucleus accumbens
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals
12-24 hours after alcohol cessation, typically resolve within 24-48 hours
Alcohol withdrawal delirium (delirium tremens or DT):
Hallucinations (predominately visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis 48-96 hours after alcohol cessation and lasts 1-5 days
Fluid and electrolyte abnormalities
Hypovolemia (from diaphoresis, hyperthermia, vomiting, ↑ RR & ↓
oral intake)
Metabolic acidosis (from
hypoperfusion, infection, alcoholic ketoacidosis, or ↓ thiamine & other B vitamins)
↓ Potassium (K) (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Magnesium
(common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate (from malnutrition)
Cardiac failure, rhabdomyolysis or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Alcohol Withdrawal: Pathophysiology & clinical findings
Authors: Erika Russell Rupali Manek Gurreet Bhandal Reviewers: Yvette Ysabel Yao Harjot Atwal Nureen Pirbhai* * MD at time of publication
↓ GABA-induced inhibition &↑ Glutamate-induced excitation relative to chronic alcohol use
CNS overactivity
Alcohol withdrawal delirium (delirium tremens or DT): Hallucinations (predominately visual), disorientation, tachycardia, hypertension, hyperthermia, agitation, and diaphoresis
48-96 hours after alcohol cessation and lasts 1-5 days
Alcohol cessation ↓ Dopamine
Alcohol withdrawal
Chronic alcohol use
↑ EtOH depressant effects on brain
in the NAc
↓Autonomic adrenergic systems
↑ Dopamine in nucleus accumbens
(NAc) relative to chronic alcohol use
Alcoholic hallucinosis: Usually visual (but can be auditory or tactile), normal vitals 12-24 hours after alcohol cessation, typically resolve within 24-48 hours
↑ Autonomic adrenergic systems relative to chronic alcohol use
↑ Sympathetic activity: ↑HR, ↑RR ↑BP, tremor & diaphoresis (↑sweating)
↓ Glutamate- induced excitation
↑ Glutamate receptors in attempt to maintain normal arousal state
↑ GABA-induced inhibition
GABA insensitivity (↑ GABA needed to maintain a constant inhibitory tone)
Early symptoms: Insomnia, tremulousness, anxiety, digestive upset, anorexia, headache, sweating, palpitations
6-12 hours after alcohol cessation
Withdrawal seizures: Generalized tonic- clonic convulsions 24-48 hours after alcohol cessation
Fluid and electrolyte abnormalities
Abbreviations:
CNS – Central nervous system K – Potassium
DT – Delirium tremens
Mg – Magnesium
NAc – Nucleus accumbens NMDA – N-methyl-D-aspartate EtOH – Alcohol
NT – Neurotransmitter
Hypovolemia (from diaphoresis, hyperthermia, vomiting, ↑ RR & ↓
oral intake)
Metabolic acidosis (from hypoperfusion, infection, alcoholic ketoacidosis, or ↓
thiamine & other B vitamins)
↓ K (renal & extrarenal K losses, alterations in aldosterone concentrations, and changes in K distribution across the cell membrane)
↓ Mg (common in patients with DT)
Dysrhythmias, seizures
↓ Phosphate (from malnutrition)
Cardiac failure, rhabdomyolysis or muscle breakdown
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 28th, 2014 on www.thecalgaryguide.com
Alcohol Withdrawal: Clinical Findings and Complications
Authors: Erika Russell Reviewers: Harjot Atwal Nureen Pirbhai* * MD at time of publication
Note: *The onset of alcohol withdrawal generally begins 6-24 hours after the last drink with symptoms peaking between 24-36 hours after and gradually lessening.
Symptoms typically progress from early symptoms and increased sympathetic activityà hallucinationsàseizures àpotentially Delirium Tremens.
Alcohol withdrawal is mild-moderate in severity for 90% of patients. Those who progressively worsen however can enter Delirium Tremens (DT) which has a mortality rate of up to 20%. More likely to have DT if had DT before, age >30 years, concurrent illness, >2 days after EtOH cessation before seeking help, and history of sustained drinking.
Long term, heavy alcohol use that leads to physical dependence
Abrupt ↓ in blood EtOH concentration
Negative physiological reactions to ↓ alcohol intake
Adaptive suppression of GABA activity from chronic alcohol enhancement
Alcohol Withdrawal*
Withdrawal symptoms alleviated by ingesting alcohol
Alcohol taken to relieve withdrawal AND/OR
Social and internal relapse cues trigger urge to use alcohol
Blood EtOH levels >600 mg% can lead to lethal respiratory depression by suppressing the respiratory centers in the brainstem
Upregulated autonomic adrenergic systems from chronic alcohol inhibition
Discontinuation of alcohol leads to rebound over-
activity of the brain and noradrenergic systems
Increased Sympathetic Activity Tachycardia, hypertension, tremor and diaphoresis
Generalized Tonic-Clonic Seizures
Usually begin within 8-24 hours of alcohol cessation and peak after 24 hours. Risk of having seizures ↑ with repeated withdrawals. 1/3 of people can progress to DT if seizures left untreated.
Discontinuation of alcohol causes a sudden relative
deficiency in inhibitory GABA activity
Reduction in dopamine in the nucleus accumbens
(NAc) from chronic alcohol exposure
Discontinuation of alcohol causes a increase in dopamine levels in NAc
Hallucinations
Commonly visual (but can be auditory or tactile), develop 12-24 hours after alcohol cessation.
Early Symptoms
Anxiety, insomnia, vivid dreams, anorexia, nausea, headache and psychomotor agitation
Delirium Tremens (DT)
Life-threatening state of greatly exaggerated withdrawal symptoms (severe tachycardia, diaphoresis etc.) with confusion/disorientation and hallucinations that generally appears 72-96 hours after the last drink and lasts 2-3 days.
Legend:
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications")
Pharmacotherapy for Dyslipidemia Overview

Bile-acid sequestrants
Bind bile acids in intestinal lumen to prevent reabsorption by enterohepatic (gut-liver) circulation
↑ Excretion of bile acids and cholesterol in stool
↓ LDL in blood
Side effects: GI disturbances, commonly interact with other drugs by interfering with absorption
See Calgary guide slide on “Bile-acid sequestrants: Mechanisms of action & side effects” for complete description of mechanism and side effects
(clinical imbalance of lipids)
Hypertriglyceridemia (if VLDL mediated & in need of treatment for pancreatitis prevention)
Hypercholesteremia
(↑ LDL in blood)
Ezetimibe
Inhibits cholesterol absorption via NPC1L1 transporter
↑ Hepatic (liver) LDL receptor expression
↑ LDL clearance from blood
↓ LDL in blood
Avoid in pregnancy
See Calgary guide slide on “Ezetimibe: Mechanisms of action & side effects” for complete description of mechanism and side effects
Combined hyperlipidemia (↑ Triglycerides and ↑ cholesterol)
Statins (ex. rosuvastatin, atorvastatin, simvastatin, pravastatin)
Competitive inhibitors of HMG-CoA reductase (rate-limiting enzyme in cholesterol synthesis)
Fibrates (ex. fenofibrate, gemfibrozil)
Activate PPAR! (nuclear receptor)
↑ Lipolysis (breakdown of lipids) and free fatty acid oxidation
↓ Triglycerides in blood
Side effects: GI discomfort, rash, pruritis
Contraindicated in pregnancy, renal failure, liver & gallbladder disease
See Calgary guide slide on “Fibrates: Mechanisms of action & side effects” for complete description of mechanism and side effects
PCSK9 inhibitors (ex. evolocumab and alirocumab which are monoclonal antibodies)
Inhibit PCSK9 (holds the LDL:LDL receptor complex together as it is internalized into the cell for destruction of LDL)
LDL receptor returns to surface without being destroyed
↑ LDL receptor expression
↑ LDL clearance from blood
↓ LDL in blood
See Calgary guide slide on “PCSK9 Inhibitors: Mechanisms of action & side effects” for complete description of mechanism and side effects
↓ Cholesterol synthesis in liver
↑ LDL receptor expression in liver
LDL receptor recognizes apoB100 (structural protein on LDL) and apoE (structural protein found on chylomicron, VLDL, IDL)
↑ Clearance of LDL cholesterol from bloodstream
↓ LDL cholesterol in blood ↑ HDL in blood
↓ Triglycerides in blood
↓ Atherosclerosis (plaque along walls of blood vessels)
Abbreviations: HDL – High density lipoprotein; HMG-CoA – Hydroxymethylglutaryl- CoA; LDL – Low-density lipoprotein; PCSK9 – Proprotein convertase subtilisin/kexin type 9; PPAR! – Peroxisome proliferator-activated receptor alpha; NPC1L1 – Niemann-Pick C1-Like 1; VLDL – Very low-density lipoprotein
Side effects: Myalgias (muscular aches), rhabdomyolysis (muscle breakdown), transaminitis (liver inflammation), liver failure, ↑ risk of diabetes mellitus
Contraindicated in pregnancy
See Calgary guide slide on “Statins: Mechanisms of action & side effects” for complete description of mechanism and side effects
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 6, 2023 on www.thecalgaryguide.com")
Death Cardiovascular Respiratory and Neurologic Mechanisms

Hypoxemia (Type I Respiratory Failure): low dissolved oxygen in blood (PaO2)
Lungs can’t oxygenate blood fast enough
Lungs can’t rid blood of CO2 fast enough
Hypercapnia / hypercarbia (Type II Respiratory Failure): elevated dissolved CO2 in blood (PaCO2)
Cerebral vasodilation
Toxins: e.g. cyanide, pesticides, arsenic Severe anemia
Distributive problems:
Systemic inflammation (sepsis, anaphylaxis, pancreatitis), adrenal insufficiency, vasodilatory drugs
Obstructive problems: Cardiac tamponade*, tension pneumothorax* or massive pulmonary embolism*
Hypovolemic* problems (low blood volume): Hemorrhage, dehydration, widespread skin disruption or burns
Cardiac valve dysfunction
Myocardial infarction* or cardiomyopathy
Cardiac arrhythmia or heart block
Disturbed electrical activity in cardiomyocytes
Peripheral metabolic disturbances
Hypokalemia*, Hyperkalemia* Acidosis* (including renal failure) Hypothermia*
Toxins* (e.g. cocaine, beta blockers, tricyclics) Severe thyroid derangement
Inappropriate systemic vasodilation
Adjacent forces impair heart filling
Low cardiac preload
Low stroke volume (SV; depends on valves, contractility, preload)
Decreased systemic vascular resistance (SVR)
Low blood pressure (BP = CO x SVR)
Decreased cardiac output (CO = SV x HR)
Disseminated intravascular coagulationàwidespread thrombi that occlude blood flow (also causes hemorrhage, see relevant box at left)
Methemoglobinemia: some hemoglobin gets stuck in a state that can’t carry O2
Hemoglobin has reduced capacity to carry or release O2
Drugs: e.g. dapsone, nitrates
Carbon monoxide poisoning
Circulatory collapse / shock: inadequate perfusion of tissue with blood
Respiratory collapse: blood has insufficient useable O2 content
Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)
Hypoxia*: inadequate O2 delivery or utilization in tissues
Hypoxia creates metabolic disturbances that impair cardiac cells. Alternatively, any of the preceding conditions marked with (*) can directly trigger cardiac arrest first
Pulseless Electrical Activity (PEA): organized activity on ECG with no cardiac output (can be preceded or mimicked by pseudo-PEA, in which there is still some output on ultrasound)
Low atmospheric pressure or oxygen content Severe lung disease
Asthma, COPD, interstitial lung disease, congestive heart failure, pulmonary hypertension, pulmonary embolism, lung collapse / atelectasis
Acute respiratory distress syndrome
Pneumonia, aspiration pneumonitis, inhalational injury, systemic inflammation, drowning
Severe hypoventilation
Respiratory fatigue, advanced COPD, chest wall disorders, neuromuscular disorders, upper airway obstruction, toxins (e.g. opioids, botulism)
Can degenerate at any time
Asystole: no cardiac electrical activity or output
Death
Respiratory arrest: cessation of breathing
Inability to protect airway
Decreased level of consciousness
Note
This is a broad overview of the many scenarios that can result in death. For detailed explanations of the various disease mechanisms, refer to the corresponding slides.
* = reversible causes of cardiac arrest (Hs and Ts)
Author:
Ben Campbell
Reviewers:
Yan Yu*
Huma Ali*
* MD at time of publication
Bradycardia
(low heart rate, HR)
Unopposed parasympathetic stimulation of heart (can also cause vasodilation, see Distributive problems)
Disruption of spinal cord sympathetic control
Injury to cervical or upper thoracic spinal cord
Irreversible cessation of cardiac, respiratory, and brain function
Prolonged seizure initially causes increased cardiovascular activity, until the system fatigues
Disruption of respiratory control center in medulla
Expanding skull contents squeeze brainstem (herniation)
Increased intracranial pressure
Edema from intracranial hemorrhage, trauma, brain mass
Edema, inflammation, hypoxia and/or metabolic derangements cause diffuse neuron dysfunction
Central nervous system infection
Dementia, particularly with delirium
Massive ischemic stroke
Seizure
activity prevents or alters breathing
Metabolic disturbances that affect the central nervous system Hypoglycemia Hypocalcemia, hypercalcemia Hyponatremia, hypernatremia Uremia
Acute liver failure (hyperNH4) Many drugs / toxins Withdrawal (e.g. EtOH)
Status epilepticus
Brainstem lesion (e.g. stroke, neoplasm, inflammatory)
Nervous System Insult
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 11, 2023 on www.thecalgaryguide.com
Respiratory System Insult
Cardiovascular System Insult Cardiogenic problems")
Turner Syndrome Pathogenesis and Clinical Findings

Partial or complete absence of second sex chromosome, leaving only one normal X-chromosome
Possible Chromosomal Profiles
Other meiotic error → deletion or misdivision of X-chromosomal material
Complete loss of one X- chromosome in all cells (45,X) (45%)
Skeletal Abnormalities
↓ Expression of SHOX gene (present on X- and Y-chromosomes)
↓ Cellular proliferation in growth plates of bones in extremities during embryonic development
Short stature
High-arched palate
Genu valgum (knock knees)
Micrognathia (smaller lower jaw)
Broad chest
Cubitus valgus (forearm angled outward)
Mosaicism (complete loss of one X-chromosome in some cells (e.g., 45,X/46,XXX, etc)) (50%)
Congenital Heart Defects (most serious)
Single copy of TIMP1 gene and presence of risk TIMP3 allele, and differential expression of KDM6A gene
Bicuspid aortic valve
Aortic coarctation
Aortic dilation (worsened by hypertension)
One X-chromosome and presence of Y-chromosomal material in some or all cells (e.g., 45,X/46,XY)
Presence of an
X- isochromosome (most commonly i(Xq))
Other structural abnormalities of X-chromsome (e.g., Ring Chromosome X, partial deletion of X, X or Y marker chromosome)
Endocrine Disorders
Turner Syndrome
The most common sex chromosomal abnormality in females (affects 1/2000-3000)
Results in deletion or non- functioning of one X chromosome
Clinical presentations vary depending on chromosome profile
Aortic dissection
Renal disease
Neurocognitive Deficits
Mechanism unknown
Deficit in social skills
Specific (non-verbal) learning disorder (otherwise normal intelligence)
↓ Executive function skills
↓ Visuospatial skills ↓ Attention
Accelerated follicular apoptosis (i.e., loss of oocytes from ovaries) → streak gonads
Ovaries are unable to respond to high gonadotropins (FSH, LH)
Hypergonadotropic hypogonadism
Premature ovarian insufficiency
↓ Expression of immune- associated genes on X- chromosome
↑ Autoimmunity
Autoimmune diseases (celiac, thyroiditis, IBD, metabolic abnormalities)
↓ Estrogen levels
Lack of breast development
↑ Liver enzymes (Additional mechanisms likely)
↓ Bone mineral density
Other Dysmorphic Features
Lymphedema Webbed (buildup of lymph neck
fluidàswelling)
Primary amenorrhea
Infertility
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com")
Sugammadex
) in plasma when administered IV
↓ Concentration of functional nNMBs in plasma
Creates a concentration gradient from muscle tissue (high) to plasma (low)
nNMBs move from muscle compartment to plasma
Sugammadex in plasma encapsulates nNMBs that moved to the plasma
↓ Concentration of functional nNMBs in the plasma
↓ Concentration of nNMBs at the nicotinic acetylcholine receptor within the skeletal neuromuscular junction
Reverses neuromuscular blockade created by nNMBs
Sugammadex
Progesterone is similar in structure to nNMBs
Sugammadex binds progesterone
↓ Progesterone activity in the body
Progesterone is critical for maintenance of early pregnancy
Unknown significance, avoid use in early pregnancy
Sugammadex-nNMB complex is cleared by the kidneys
Higher concentrations of sugammadex facilitate faster nNMB clearance
Unknown mechanisms
Post operative nausea and vomiting
Headache Bradycardia Cardiovascular Collapse
↓ Effectiveness of progesterone-based contraception for 7 days
↓ Clearance in patients with severe renal impairment
Reversal of profoundly deep neuromuscular blockade at higher doses
Binds to IgG or IgE receptors on sensitized basophils/mast cells in allergic reactions
Activation of basophils/mast cells
Degranulation of basophils/mast cells
Release of granulation products
Anaphylaxis Bronchospasm Hypotension
Authors: Arzina Jaffer, Kayleigh Yang Reviewers: Jasleen Brar, Mao Ding Joseph Ahn* * MD at time of publication
Movement of limbs or body during anesthesia
Coughing during anesthesia
Grimacing or suckling on the endotracheal tube
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 16, 2024 on www.thecalgaryguide.com")
Bacterial Infections from Transfusion
 recognize bacteria
Immune cells release pyrogens (either bacterial components or signalling molecules) upon recognition
Pyrogens bind to receptors on the hypothalamus
Hypothalamus ↑ body temperature set point
Body generates and conserves heat to reach set point
Immune cells release pro- inflammatory cytokines (messenger protein)
Cytokines activate sympathetic nervous system via hypothalamus
Adrenal glands release stress hormones (epinephrine and norepinephrine) into bloodstream
Stress hormones bind to receptors on cardiomyocytes (heart muscle cells)
↑ Heart contractility
↑ Heart rate
Cytokines circulate throughout the body
Cytokines interact with endothelial cells of the blood vessels
↑ Nitric oxide production
Relaxes smooth muscle cells of blood vessel walls
Vasodilation (↑ blood vessel diameter)
Hypotension
Systemic inflammation
Stimulate nerve endings in muscles
Stimulate nerve endings in gastrointestinal tract’s lining
Blood brain barrier’s integrity is compromised
Nitric oxide reacts with oxygen to form reactive nitrogen species
Tissue damage
Fatigue
Weakness Muscle aches
Nausea and vomiting
Immune and inflammatory cells enter the brain
Authors:
Arzina Jaffer
Kayleigh Yang
Reviewers:
Nimaya De Silva
Raafi Ali
Michelle J. Chen
Yan Yu*
Kareem Jamani*
* MD at time of publication
Inflammation in the brain
Activates pain processing centers in the brain
Headache
Damages neurons and disrupts cell communication
Confusion and altered mental state
Shivering
Fever
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 30, 2024 on www.thecalgaryguide.com")
Carbonic Anhydrase Inhibitor Diuretics

Inhibition of carbonic anhydrase on the apical surface of the brush border cells in the proximal convoluted tubule (PCT)
Activation of the Renin- Angiotensin-Aldosterone Systemfromvolume depletion
Activation of principle cell
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+ and waste K+
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical
Findings slide
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H2O available for excretion
Mild diuresis (increase in frequencyandvolumeof urine)
↓ Blood volume
Hypotension
↓ Na+ and HCO3- reabsorption in the PCT
↑ HCO3- delivery to cortical collecting duct
Urine alkalization (increased pH)
Chronic urine alkalization
↓Solubilityof citrate
↓ Urinary citrate
↓ Citrate binding with Ca2+à↑ Ca2+ complexing with oxalate
↑ Spontaneous nucleation, growth and agglomeration of calcium oxalate crystals
Formation of calcium oxalate renal calculi
↑ HCO3- is lost in the urine ↓ pH of the blood
Type II Renal Tubular Acidosis
See Type II/Proximal Renal Tubular Acidosis slide
CAI prevents the up- regulationofglutamine transporters in the PCT
Inability to correct the metabolic acidosis and impaired urinary NH3 excretion
Hyperammonemia (↑ serum NH3 )
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 3, 2024 on www.thecalgaryguide.com
Carbonic Anhydrase Inhibitor Diuretics: Renal Mechanism and Side Effects Carbonic Anhydrase Inhibitors (CAI)
Inhibition of carbonic anhydrase on the apical surface of the brush border cells of the proximal convoluted tubule (PCT)
Authors: Stephanie Happ Reviewers: Matt Hobart Name Name* * MD at time of publication
↓ Na+ and HCO3- reabsorption in the PCT
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H O available for 2
excretion
Mild diuresis
↓ Blood volume Hypotension
↑ HCO3- delivery to cortical collecting duct
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+
↑ Intracellular Na+ drives Na+/K+ ATPase activity on the principal cells (moving 2 K+ into cell and 3 Na+ out into the peritubular capillary)
↑ Intracellular K+ drives H+/K+ ATPase activity on the intercalated cells (moving 1 H+ into cell and 1 K+ out into the tubular filtrate)
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical Findings slide
Urine alkalization
↑ HCO3- is lost in the urine, leading to ↓ pH of the blood
Renal Tubular Acidosis Type II
See Type II/Proximal Renal Tubular Acidosis slide
CAI inhibit the up-regulation of glutamine transporters in the PCT
Inability to correct the metabolic acidosis and
impaired urinary NH3 excretion
Hyperammonemia
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Chronic urine alkalization leads to marked ↓ in urinary citrate
↓ Ability of citrate to bind to Ca2+ and calcium oxalate stones
↓ Inhibition of spontaneous nucleation
↓ Prevention of growth and agglomeration of crystals
Formation of calcium oxalate renal calculi
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com")
Stable Angina

↓ Blood vessel lumen diameter
↓ Volume of blood is supplied to the heart
Predictable period of physical activity or emotional stress
↑ Heart rate
↓ Time for coronary arteries to fill heart with blood (diastole)
↑ Heart contractility
↑ Oxygen demand of heart muscle tissue (myocardium)
↓ Myocardial blood supply
Imbalance between blood supply & oxygen demand causes myocardial ischemia
Angina Pectoris/Stable Angina
Myocardial ischemia causes cardiac muscle cells (cardiomyocytes) to switch from oxygen-dependent (aerobic) to oxygen-absent (anaerobic) metabolism
Anaerobic metabolism produces metabolites that stimulate cardiac spinal afferent nerves
Myocardial visceral afferent & somatic sensory nerve fibers mix & enter the spinal cord via T1-T4 nerve roots
Brain interprets ↑ nerve signaling as nerve pain coming from the skin of T1-T4 dermatomes (referred pain)
↑ lactic acid production & ↓ cellular pH impairs cardiomyocytes’ function
Damaged cardiomyocytes impair myocardial relaxation & cause ↓ left ventricular contractility & cardiac output
Blood backs up into left ventricle, atrium, & pulmonary vasculature
↑ Pulmonary capillary pressures pushes fluid out & into the lung’s alveoli
↓ Gas exchange & oxygenation
↑ Respiratory rate & Dyspnea (shortness of breath)
Blood flow begins at the epicardium (outer heart layer) & ends at endocardium (inner layer)
Subendocardium (innermost heart layer) receives the least blood flow causing non-transmural (partial thickness) heart wall ischemia
Anterior/septal & lateral wall ischemia triggers ↑ sympathetic nervous system (SNS) activity given the proximity of cardiac SNS innervation
Inferior wall ischemia triggers involuntary ↑ in Vagus nerve activity given the nerve’s proximity
Bradycardia (↓ heart rate)
Nausea
Adrenal medulla releases Norepinephrine hormone
Activation of sweat glands via SNS acetylcholine neurotransmitter release
Hypotension (↓ blood pressure)
Pain radiation to left arm, jaw, abdomen & upper back
Chest pain, pressure, or discomfort
Unstable Angina (unpredictable & worsening chest pain)
See relevant Calgary Guide slide on Unstable Angina
Binds arterial smooth muscle α1 receptors
↑ Coronary arteries’ vascular tone (vasoconstriction)
Hypertension (↑ blood pressure)
Activates β1 receptors in the heart
Tachycardia (↑ heart rate)
Diaphoresis (↑ sweating)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 8, 2013; updated Feb 5, 2024 on www.thecalgaryguide.com")
Gestational Diabetes Risk factors and pathogenesis

Authors:
Amyna Fidai
Maharshi Gandhi Reviewers:
Laura Byford-Richardson Shahab Marzoughi
Yan Yu*
Hanan Bassyouni*
* MD at time of publication
High risk population (Aboriginal, Hispanic, South Asian, Asian, African)
Previous or current macrosomia (>4000g) or polyhydramnios
Other conditions associated with Diabetes Mellitus such as polycystic ovarian syndrome, hypertension, metabolic syndrome
Placental counter regulatory hormones (particularly Human Placental Growth Hormone) oppose the action of insulin
↑ Insulin resistance (liver, muscle, adipose tissues become less responsive to insulin)
↑ Fetal demands after 18 weeks gestation
(fetus requires 80% of its energy from maternal glucose)
↑ Carbohydrate intake to keep up with the demands
Previous history of gestational diabetes or glucose intolerance
Family history of diabetes
Advanced maternal age
Obesity
Previous unexplained stillbirth
Multiples (larger placental mass and activity)
Corticosteroid use
↑ Risk for pregnancy induced glucose intolerance (mechanism unclear and/or complex)
↑ Insulin requirements Initially pancreatic beta cells work
overtime to keep up with the ↑ insulin demands
Eventually insulin demands are not met due to the exhaustion of pancreatic beta cells
Plasma glucose rises (Fasting plasma glucose ≥5.3 mmol/L)
Gestational Diabetes (or exacerbation of pre-existing DM)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 28, 2017, updated Feb 24, 2024 on www.thecalgaryguide.com")
Infectious Small Bowel Diarrhea

May produce Shiga toxins (a specific family of toxins that can lead to complications)
Authors: Noriyah Al Awadhi Yan Yu Sara Cho Reviewers: Paul Ratti Jason Baserman Shahab Marzoughi Kerri Novak* * Indicates MD at time of publication
Y. enterocolitica
(also milk, cheese)
Shellfish, undercooked seafood
V. parahaemolyticus V. cholerae
Enterohemorrhagic E. coli (EHEC)
Daycare centers/nurseries
Drinking/swimming in bad water — mountains/wells
S. aureus
B. cereus
Noroviruses
Rotavirus
G. lamblia
C. parvum
May produce emetic toxins (toxins that cause vomiting)
Adequate amount of organism and/or toxin is ingested
Organism adheres to the intestinal liningàorganism colonizes the small intestine Organism releases enterotoxin (a toxin that affects the intestines)
Binds to and disrupts intestinal transporters used in secretion and absorption of water and electrolytes
Toxin enters systemic vasculature
Shiga toxins inhibit ADAMTS13 (cleaving enzyme)
Failure to cleave von Willebrand Factor (vWF) multimers
Accumulation of vWF multimers
Platelets and thrombi accumulate in microvasculature
Hemolytic uremic syndrome (hemolytic anemia, thrombocytopenia, and acute renal damage)
↑ Water and electrolyte secretion
↓ Fluid absorption
Chemoreceptor trigger zone in medulla detects circulating emetic toxins
Nausea & vomiting
Triggers release of inflammatory mediators and cytokines that travel to the central nervous system
Prostaglandin is synthesized and released
Neurotransmitter cyclic AMP (cAMP) is released
cAMP ↑ hypothalamic thermoregulation set point
Fever
Large volume profuse diarrhea
Loss of water
Distention (swelling) of intestines stimulates visceral sensory pain fibers
Visceral pain fibers crosstalk with somatic nerves from the same spinal cord level
Occasional referred pain/cramping (typically diffuse pain around the abdomen)
Loss of bicarbonate, sodium, potassium, magnesium, and chloride
Dehydration
Electrolyte deficiency
Metabolic acidosis (pH < 7.4 & serum bicarbonate < 24)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 7, 2012; updated Mar 25, 2024 on www.thecalgaryguide.com")
Post-Renal Acute Kidney Injury AKI
: Pathogenesis and clinical findings
Blood clot or cellular debris
Foreign body
Neurogenic bladder
Obstruction intrinsic to urine excretion system
Nephrolithiasis (kidney stones)
Anatomical defect(s)
Intra- abdominal adhesions
Retroperitoneal fibrosis (scar-like tissue)
Benign or malignant masses
Prostate cancer
Benign prostatic hyperplasia
↓ Urine flow across point of obstruction Obstruction extrinsic to urine excretion system
Urine buildup distends urine collecting system (hydronephrosis)
Compression of renal vasculature due to mass effect
↑ Volume/pressure proximal to obstruction
↑ Intratubular pressure
↓ Pressure gradient between glomerular afferent arteriole and Bowman’s space
Casts occlude tubules
↓ Filtration of plasma into nephrons
↓ Glomerular Filtration Rate (GFR)
Obstruction is relieved ↓ Intratubular pressure Rapid GFR ↑
Rapid diuresis of fluid and electrolytes
Dilated pelvicalyceal system on ultrasound
↓ Urine output
↓ Venous drainage
and arterial supply
Local ischemia and inflammation of kidney
Impaired resorption, excretion, and fine tuning by tubules
Acute Tubular Necrosis (ATN) with granular casts
↓ Urine output
↓ Clearance of free water and solutes
↑ Intravascular volume
↑ Serum creatinine
↓ Medullary solute concentration, ischemia, ↓ response of collecting ducts to antidiuretic hormone
Lasts > 24hrs
Post-obstructive diuresis causes hypovolemia and electrolyte derangements
Authors: David Campbell, Matthew Hobart Reviewers: Raafi Ali, Luiza Radu Huneza Nadeem, Marissa Zhang, Julian Midgley* * MD at time of publication
Resolves < 24hrs in euvolemia
Physiologic post- obstructive diuresis
↑ Na+ and Cl- delivery to distal convoluted tubule is sensed by macula densa
Secretion of adenosine by macula densa
Adenosine constricts afferent arterioles
↓ GFR
↓ Renal clearance of drugs and waste products
↑ Venous hydrostatic pressure
↑ Volume in arterial system overwhelms pressure regulation mechanisms
Hypertension
Fluid extravasation from veins and capillaries
Generalized Edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 25, 2024 on www.thecalgaryguide.com")
Operative Vaginal Delivery Indications
: Indications
Authors: Taylor Pigott Akaya Blair Reviewers: Michelle J. Chen Sylvie Bowden* Stephanie Cooper* Sarah Glaze* * MD at time of publication
Abnormal fetal heart rate/fetal distress
↓ Risk of maternal and fetal morbidity/ morality
Rupture of membranes without fetal head adequately applied to maternal pelvis
Small pelvic outlet Narrow vaginal canal
Cardiovascular disease
Diabetes Hypertension Abdominal trauma
Short umbilical cord
Large for gestational age (LGA) fetus
Neurological/ muscular disease
↑ Pain during labor
Maternal contraindication to Valsalva maneuver (e.g., cardiac disease, cystic lung)
Rush of fluid past the fetal head out through cervix
Umbilical cord prolapse
Umbilical vasoconstriction
Umbilical cord compression
↓ Blood flow through umbilical cord
Fetal presenting part applies pressure on umbilical cord
Impaired vascular function and narrowed vessels ↓ blood flow around the body
↓ Oxygen transfer across the placenta
Fetal oxygen deprivation and hypoxia
Operative vaginal delivery with forceps or vacuum expedites delivery
Placenta partially or completely separates from uterine wall (abruption)
Increased tension of umbilical cord on placenta
Fetal shoulder is lodged behind maternal pubic symphysis
Delivery of the body is delayed
Inability to adequately bear down to push
Myometrium runs out of energy from repeated contractions and becomes less able to contract (↓ uterine tone)
Uterine spiral arteries dependent on contractions for vasoconstriction remain dilated, allowing blood flow
Postpartum hemorrhage
Uterine rupture
↑ Risk of future pelvic organ prolapse
↑ Risk of future incontinence
Prolonged labour
Repeated contraction/ relaxation of the uterus without progress tears and damages uterine muscles
↓ Maternal endurance
Inadequate fluid and food intake prior to/ during labor
Multiples
↑ Sympathetic nervous system activation during labor
Maternal exhaustion
Uterine muscles stretch to accommodate multiple growing fetuses
↑ Pushing against pelvic floor and perineum
Pushing force damages pelvic floor muscles and nerves
↓ Myometrial contractility
↑ Need for vaginal exams to check on labour progress
Bacterial overgrowth in vagina and/or uterus
Maternal infection
Fetal infection
↓ Strength of contractions
Epidural anesthetic
Inability to ambulate to urinate
↑ Urinary catheterizations
↑ Epinephrine secretion from adrenal cortex
Blood is shunted away from uterus/internal organs and towards heart and skeletal muscle
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published 03, ##, 2023 on www.thecalgaryguide.com")
Sickle Cell Disease Pathogenesis Clinical Findings and Complications
 Liu Priyanka Grewal Reviewers: Alexander Arnold Luiza Radu JoyAnne Krupa Yan Yu* Lynn Savoie* * MD at time of publication
Hemoglobin S (HbS) variant formed instead of normal Hemoglobin A (HbA)
Hb electrophoresis shows approximately 45% HbS, 52% HbA (ααββ), 2% HbA
Hb electrophoresis shows approximately 90% HbS, 8% HbF, & 2% HbA .
No HbA present
(ααδδ), & 1% HbF (ααγγ;2 fetal hemoglobin)
Heterozygous: point mutation in one of the two chromosomes (Hb AS)
Sickle cell trait
(asymptomatic unless severely hypoxic)
Homozygous: point mutation in both chromosomes (Hb SS)
Sickle cell disease
An inherited blood disorder characterized by defective hemoglobin that leads to red blood cells sickling
2
Dehydration Hypoxemia
Acidosis
↓ Volume of RBC cytoplasm
↓ O2 Saturation of Hb
O morereadily 2
released from Hb in low pH environment
↑ Concentration of deoxygenated HbSinred blood cells (RBCs)
Hydrophilic glutamate→ hydrophobic valine substitution makes HbS less soluble in the cytoplasm & more prone to polymerization & precipitation in its deoxygenated state
↑ Concentration of deoxygenated Hb in RBC leads to ↑ polymerization rate Polymerized & precipitated HbS forms long needle-like fibers
RBC shape becomes sickled
Sickle cells on peripheral blood smear
Vaso-occlusion
(sickled RBCs lodge in small vessels, blocking bloodflow to organs & tissues)
Blockage of venous outflow
Occlusion of vessels in lungs ↑ pulmonary blood pressure
Fluid extravasates into interstitial tissue leading to pulmonary edema
Acute chest syndrome (chest pain, hypoxemia (↓blood oxygen), etc.)**
to the penis:
to the spleen:
Priapism (persistent, painful erection)
Splenic Sequestration (blood pools in spleenà splenomegaly & hypotension)
Extravascular hemolysis (macrophages in the spleen phagocytose sickled RBCs)
Normocytic anemia
↑Marrow erythropoiesis (RBC production) to compensate for hemolysis
Infarction of bone
Pain crises
If occurring in hands
Dactylitis (inflammation of digits)
Blockage of arteries ↓ oxygenation of organs & tissues
Vaso-occlusion of the splenic artery
Splenic infarction (↓ blood supply leads to tissue death)
RBC inclusions (structures found in RBCs) not removed by spleen
Howell-Jolly bodies (RBC DNA remnants) on blood smear
Vaso-occlusion of other arteries (cranial, renal, etc)
Stroke, renal failure
↑ RBC breakdown
↑ Unconjugated bilirubin released from RBC breakdown
RBC precursors (reticulocytes) are released into the blood stream
Reticulocytosis (increased number of immature red blood cells) on peripheral blood smear
Patient’s RBC level becomes dependent on increased marrow activity
Bone marrow infarction or viral infections (i.e. Parvovirus B19) suppresses bone marrow activity
Aplastic crises (profound anemia)
** See corresponding Calgary Guide slide(s)
↑ Serum level of unconjugated bilirubin
Some of the circulating unconjugated bilirubin deposits in the skin
Jaundice (yellowing of skin)
↑ Conjugation of bilirubin in liver
↑Amounts of conjugated bilirubin released into bile
Gallstone formation
Cholelithiasis (presence of gallstones in the gallbladder)
Spleen releases invasive encapsulated bacteria (eg. Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis) into circulation, which causes infections
Meningitis
Sepsis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 16, 2013, updated Apr 29, 2024 on www.thecalgaryguide.com")
Gynecomastia

Hyperthyroidism
Klinefelter Syndrome (males with > 1 X chromosome)
Liver cirrhosis
Certain tumors (e.g., germ cell, adrenal, Leydig cell, Sertoli cell)
Anabolic steroid usage (containing testosterone)
Finasteride (treatment for benign prostate hyperplasia and male pattern baldness)
Cimetidine - inhibits stomach acid production
Spironolactone (diuretic
used to treat high blood pressure and heart failure)
Ketoconazole (antifungal)
Cytotoxic agents (e.g. alkylating agents, vincristine, methotrexate)
Imbalance between estrogens and androgens
Estrogen stimulates breast tissue growth in newborn
Changes in metabolic rate ↑ fat production
Unclear mechanism
↑ Proinflammatory mediators and cytokines (e.g. prostaglandin E2, TNF⍺, IL-1, IL-6, cyclooxygenase-2)
Prostaglandin E2 and IL- 6 upregulate aromatase enzyme expression
Available estrogen is higher than available testosterone
↑ Aromatase enzyme activity, converting androgens to estrogen
↓ Testosterone release from the testes
↓ Testosterone
↑ Serum sex hormone binding globulin (SHBG)
SHBG binds estrogen with less affinity to testosterone
Thyroid hormone stimulates liver to express more sex hormone binding globulin
Thyroid hormone stimulates aromatase activity
Overexpression of aromatase enzyme
Seminiferous tubules in the testes hyalinize and fibrose
Suppression of the hypothalamic pituitary thyroid axis through an unclear mechanism
Tumor may produce estradiol
Tumor produces β- human chorionic gonadotropin (β-HCG)
↑ serum testosterone
Inhibits 5-α reductase
Blocks binding of 5-DHT to androgen receptors
↓ 2-hydroxylation of estradiol
Mimics structures of testosterone
Inhibits 17,20 desmolase and 17α-hydroxylase
Damage to Leydig cells in testes
↑ Estrogen to androgen ratio
Pathological causes
Impaired spermatogenesis and testosterone production
↓ GnRH secretion from hypothalamus
↓ Testosterone
↓ Luteinizing hormone (LH) release from anterior pituitary
↓ 5-DHT and/or testosterone binding to androgen receptors in chest tissue
↓ inhibition of breast development
Normal or increased estrogen acts on estrogen receptor on chest tissue
Estrogen receptors stimulate breast development
Estradiol negatively feedbacks on luteinizing hormone
β-HCG stimulates LH receptors on Leydig cells in the testes
Aromatase enzyme converts excess testosterone into estrogen and estradiol
↓ conversion of testosterone to 5- dihydrotestosterone (5-DHT), a more potent form of testosterone
Glandular proliferation in male breasts
Gynecomastia
(development of breast tissue in males)
Drug side- effects
↓ Metabolism of estradiol
Competitively binds to androgen receptors
↑ Serum estradiol levels
Exhibits physical attributes that do not align with gender identity
Psychological distress
In some cases, hormones stabilize
Involution and atrophy of ducts
Gynecomastia resolves
↓ Steroid synthesis
↓ Androstenedione produced (testosterone precursors)
↓ Serum testosterone levels
↓ Testosterone production
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jun 9, 2024 on www.thecalgaryguide.com")
Anesthetic Considerations in Pregnancy

↑ Progesterone serum levels
↓ Esophageal tone & sphincter pressure
↑ Aspiration risk >20 weeks gestation & during labor
Aspiration prophylaxis
Rapid sequence induction
Nonparticulate antacid prophylaxis (e.g., sodium citrate, famotidine)
Pre-operative fasting & gastric ultrasound to assess volume
Breathing
↑ Minute ventilation
↓ PaCO2 at baseline
Uterine artery vasoconstriction with maternal PCO2 levels exceeding 32 mmHg
Impaired uteroplacental perfusion
Maintain physiologic alkalosis, avoid maternal hypercapnia
Maintain
maternal arterial PCO2 28–32 mmHg
Avoid permissive hypercapnia
↑ Progesterone serum levels
Disproportionate ↑ in plasma volume
↓ Serum colloid osmotic pressure
Drug-specific alterations in absorption, distribution, metabolism & excretion (e.g. ↑ distribution of acidic drugs due to ↓ albumin; ↑ clearance of renally- metabolized drugs)
Optimize anesthetic dosing for altered pharmacokinetics
Adjust dosages based on drug recommendations
Circulation
↑ Maternal blood volume
Peripheral vasodilation
↓In systemic vascular resistance by 25–30%
↓ Blood pressure
↑Abdominal pressure
Compression of the aorta & inferior vena cava
Supine hypotension
Impaired uteroplacental perfusion
Fetal ischemia
Optimize
placental blood flow
Position patient on left side to maintain uterine displacement
Diaphragmatic elevation & lung compression
↓ Functional residual capacity
↑ Risk of rapid desaturation
Fetal hypoxemia
Maintain maternal & fetal oxygenation
Optimize positioning (e.g., patient on left side to maintain uterine displacement)
& supplement oxygen as needed
Heart rate ↑ 15-25%
↑ Cardiac output
Manifestations of significant blood loss are delayed
Avoid hypotension
↑ Stroke volume
Avoid fluid overload
Treat abnormal variation in blood pressure at lower values
Fetus
Requirement to assess & treat two patients
Achieve optimal anesthetic dosing for mother while maintaining fetus safety
Maintain oxygenation of both mother & fetus & ensure adequate uteroplacental perfusion
Consider fetal-drug transfer & adjust agent & dose accordingly
Monitor maternal vital sign & fetal heart rate
Utilize a multidisciplinary team (e.g., pharmacy, nursing, physical & occupational therapy)
Legend:
Pathophysiology
Mechanism
Goal
Management
Published July 5, 2024 on www.thecalgaryguide.com")
Diabetes Mellitus Pathophysiology Behind Lab Findings

↓ Glucose uptake into cells
Autoimmune destruction of pancreatic beta cells (type 1 diabetes mellitus)
Insulin resistance (type 2 diabetes mellitus)
Other causes of diabetes mellitus (genetic, drug- induced, pregnancy, etc.)
↑ Lipolysis (fat breakdown) in adipose tissue
↑ Free fatty acids & glycerol in bloodstream
↑ Oxidation of fatty acids in liver to form acetyl CoA
↑ Conversion of acetyl CoA to ketone bodies (ketogenesis) to be used as fuel for the brain
Relative or absolute insulin deficiency
↓ Activation of adipose (fat tissue) & muscle cell transmembrane insulin receptors
↓ Activation of intracellular insulin signaling pathways (PI3K & MAP kinase)
Cells cannot use glucose as a source of energy; thus body reacts as if it is starving
↑ Protein breakdown in muscle tissue ↑ Amino acids & lactate in bloodstream
↑ Substrates (glycerol, amino acids & lactate) available to produce glucose in the liver
↑ Glycogenolysis (breakdown of stored glucose - glycogen) & gluconeogenesis (production of glucose) in liver
Glucose in bloodstream glycates (coats) hemoglobin in red blood cells; thus ↑ blood glucose leads to ↑ glycated hemoglobin
↑ Hemoglobin A1C
↑ Fasting blood glucose level ↑ Random blood glucose level
↑ Blood glucose following oral glucose tolerance test
Diabetic ketoacidosis (DKA) in absolute insulin deficiency *See DKA slide
Filtered ketone bodies exceed the reabsorption capacity of renal tubules
Ketonuria (↑ ketones in urine)
↑ Glucose in bloodstream
Build-up of glycation end products causes damage to glomerular tissue
Transient glomerular hyperfiltration followed by long-term ↓ in glomerular filtration rate
Albuminuria (↑ albumin in urine)
Diabetic nephropathy *See slide
Filtered glucose exceeds reabsorption capacity of renal tubules in the kidney
Glucosuria (↑ glucose in urine)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 8, 2024 on www.thecalgaryguide.com")
Neonatal Hypoglycemia Pathogenesis
, glycogenolysis (breakdown of glycogen into glucose), and fatty acid oxidation (conversation of fatty acids to ATP)
Low glucose levels stimulate the neonate’s appetite, allowing them to adapt to intermittent feeds
Infant feeding regularly on a diet with sufficient carbohydrates creates a consistent plasma glucose concentration
Pregnant Parent Causes
Impaired Glucose Production
Inadequate Glucose Supply
Pregnant parent using β-blockers
β-blockers prevent epinephrine from binding to adrenergic receptors in skeletal muscle and liver
Blocked sympathetic signaling in these organs prevents glycogenolysis
↓ Breakdown of glycogen into glucose
Infant of a parent with diabetes
Parent has a high level of glucose in their blood
The fetus receives a glucose-rich blood supply
Fetal pancreatic β cells ↑ insulin production
Post-birth, glucose levels in the infant’s circulation ↓ but insulin levels
remain high
Excessive glucose uptake into cells
Fetus born with a metabolism disorder (e.g. organic amino acid disorder, disorder of glycogen metabolism, disorder of gluconeogenesis)
Genes that make proteins or hormones responsible for production, breakdown and regulation of glycogen are mutated
Fetus born with an endocrine disorder (e.g. congenital adrenal hyperplasia, hypopituitarism, Turner Syndrome)
Pituitary and/or adrenal gland dysfunction ↓ release of hormones that regulate glucose balance
Fetal growth is restricted, fetus is small for gestational age, or is premature (<37 weeks gestation)
Glycogen is deposited during the 3rd trimester of pregnancy. Infants born early have fewer stores; smaller infants born at term have ↓ stores, ↑ insulin sensitivity, & poorly coordinated counter- regulatory hormones
↑ Glucose demand for the transition to life out of the womb
Glycogen stores used up quickly
Perinatal stress (e.g. sepsis, asphyxia)
Stress stimulates fetal adrenal glands to ↑ epinephrine secretion
Fetal pancreatic ⍺- cells ↑ glucagon secretion
↑ Breakdown of muscles and fat for glucose- building blocks
Glycogen stores used up quickly
↑ Glucose usage as fetal metabolic demands ↑ to manage stress
Fetal β-cells secrete inappropriately high levels of insulin despite hypoglycemic state; this hyperinsulinism state can last for months & resolve spontaneously
↓ Serum glucose Neonatal hypoglycemia
Authors: Dasha Mori Reviewers: Michelle J. Chen *Dr. Danielle Nelson *MD at time of publication
Blood glucose < 2.6 mmol/L in term & preterm infants within 72 hours of birth or < 3.3 mmol/L after 72 hours of birth
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 19, 2024 on www.thecalgaryguide.com")
Generalized Anxiety Disorder GAD
: Pathogenesis and clinical findings
Authors: Keira Britto Reviewers: Sara Cho, Luiza Radu, *Margaret Oakander *MD at time of publication
Altered cognition
Scan environment for perceived threats
Genetic predisposition & family history: polygenic, >30% heritability
Adverse childhood & life experiences: e.g., abuse, neglect, divorce, bereavement
Morbidity & stressors from chronic medical conditions
Hypersensitivity & reactivity to stimuli
áHPA axis activity
Neurobiological differences
Trait neuroticism (emotional instability & nervousness)
Reacts to unfamiliarity with withdrawal & fear
áLevel of uninhibited excitatory signaling
Psychomotor agitation
Frequent sympathetic nervous system (fight or flight) activation to perceived threats
Cycles of epinephrine surges
Inadequate recovery
State of hyperarousal
Disturbed sleep
Ongoing sleep deprivation
Easily fatigable
áACTH released from hypothalamus
áCortisol released from adrenal glands
áSerotonin uptake
âSerotonin Impaired
neuroplasticity &âcomplexity of synaptic connections in amygdala & hippocampus
âAbility to deal with emotional stressors
Impaired engagement of prefrontal cortex
âRegulation of emotional reactions
áAnticipatory emotional responses
âInhibition from GABA
áAmygdala volume & activity
áFear & anxiety circuits
Attentional focus directed towards worries & perceived threats
Divert blood to muscles
Skeletal muscle activation
Muscle tension
Psychomotor agitation (excessive motor activity associated with a feeling of inner tension)
áEmotional intensity
Chronic state of high physiological stress
âHippocampal BDNF (brain derived neurotrophic factor)
Hippocampal atrophy &â hippocampal neurogenesis
â Inhibitory control of the hippocampus over the HPA axis
áAlertness & wakefulness
Disturbed sleep
Strengthening of memories rooted in fear, to prevent encounters with future threats
Behavioural & cognitive changes to facilitate coping with threats
Irritability
**Excessive, persistent
Bottom up, stimulus driven attention
áDistractibility
Difficulty concentrating
anxiety & worry that is distressing &/or impairs functioning
Irritability
Generalized Anxiety Disorder:
**occurring more days than not for ≥ 6 months; **difficult to control; presence of ≥ 3 remaining symptoms
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 21, 2024 on www.thecalgaryguide.com")
Underfill Edema Pathogenesis

Vasodilatory medications
Various mechanisms
Right-sided heart failure
Compromised right heart function ↓ forward flow
↓ Hepatic albumin synthesis
Blood is unable to pass through hepatic vessels disrupted by cirrhosis and backs up in portal vein
↑ Blood pressure in portal vein (portal hypertension)
Less blood volume in hepatic veins and vena cava (underfilling)
Pregnancy
↑ Estrogen, progesterone and relaxin
Vasodilation
Gravity causes fluid accumulation in peripheral veins
↑ Capillary hydrostatic pressure
↑ Net fluid movement into interstitial space
↓ Serum albumin
↓ Capillary oncotic pressure
Fluid extravasation into interstitial space
More blood in portal vein ↑ capillary hydrostatic pressure in venous system
Pressure creates net fluid
movement from vascular space into interstitial space
Less blood volume in arteries (underfilling)
↓ Effective arterial blood volume (EABV)
↓ Renal blood flow activates the renin-angiotensin-aldosterone system (RAAS)
Angiotensin and aldosterone ↑ Anti-diuretic hormone released by tubular Na+ and H2O resorption posterior pituitary ↑ H2O resorption
↑ Fluid in circulation, worsening existing venous congestion
↑ Hydrostatic capillary pressure and fluid extravasation into interstitial space Underfill edema (edema worsened by activation of RAAS)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 19, 2015; updated Aug 5, 2024 on www.thecalgaryguide.com")
IgA Nephropathy
 created by mucosa- bound IgA1 plasma cells is secreted into plasma instead of onto mucosal surface
IgA1 plasma cells hyper- responsive to triggers (eg. URTIs, gastroenteritis) ↑ synthesis of GD-IgA1 → spill-over into plasma
Immunoglobulin A1 (IgA1) plasma cells destined to reside in mucosa (eg. gut or respiratory tract) travel to and
reside in inappropriate site(s) (eg. bone marrow) releasing GD-IgA1 into plasma
GD-IgA1 is not cleared from plasma as quickly as IgA1 → ↑ plasma GD-IgA1 levels
Hit 3:
GD-IgA1-IgG complexes deposit in mesangium
C3 predominant complement activation amplifies inflammatory response
Renal biopsy:
IgA deposits in mesangium (100% sensitive)
Renal biopsy: Complement in mesangium (C3 predominant) (90-95% sensitive)
A cascade of multiple immunologic hits is initiated
Hit 1: ↑ Serum levels of GD-IgA1 multiple immunologic hits
GD-IgA1 hinge region is structurally distinct from IgA1 that would normally circulate in plasma (lack of galactosyl groups)
GD-IgA1 hinge region may mimic pathogens (ex. bacteria and viruses) or other antigens
Cross reactivity of IgG against GD-IgA1, or synthesis of anti-GD-IgA1 IgG antibodies
Immunoglobulin G (IgG) binds GD-IgA1 hinge region Hit 2: GD-IgA1-IgG immune complex formation
Circulating GD-IgA1-IgG complexes have high affinity for glomerular endothelial cells where they damage the glycocalyx → ↑ permeability of immunoglobulins into the mesangium
↑ Production of chemokines, cytokines and complement → ↑ mesangial cell proliferation and matrix expansion
Leukocyte recruitment and activation damages glomerulus and mesangium
Hit 4:
Inflammatory response to GD-IgA1 complexes in mesangium induce glomerular structure disruption (endothelium, basement membrane, podocytes, mesangium)
and impaired glomerular function
Loss of barrier functions of glomerulus allows for extravasation of blood & proteins into Bowman’s space and subsequently through tubules
Renal biopsy: Glomerulosclerosis, tubulointerstitial fibrosis, glomerular vasculitis, podocyte damage
Eventual end-Stage Renal Disease (ESRD)
Progressive ↓ of filtration surface area within glomeruli and ↓ number of functional glomeruli
Proteinuria
Synpharyngitic hematuria (hematuria with dysmorphic red cells co-occurring with pharyngitis)
↓ Glomerular Filtration Rate (GFR)
Nephrotic Syndrome
↑ Serum creatinine
Chronic kidney disease and eventually ESRD
IgAN is an autoimmune disease where IgA deposition in the glomerulus leads to an inflammatory cascade, endothelial dysfunction and mesangial expansion that damages glomeruli causing kidneys to leak blood and protein into urine and decreased kidney function. IgA nephropathy is a multifactorial disease requiring multiple immunologic hits
IgA Nephropathy (IgAN)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 5, 2024 on www.thecalgaryguide.com")