SEARCH RESULTS FOR: pharyngitis
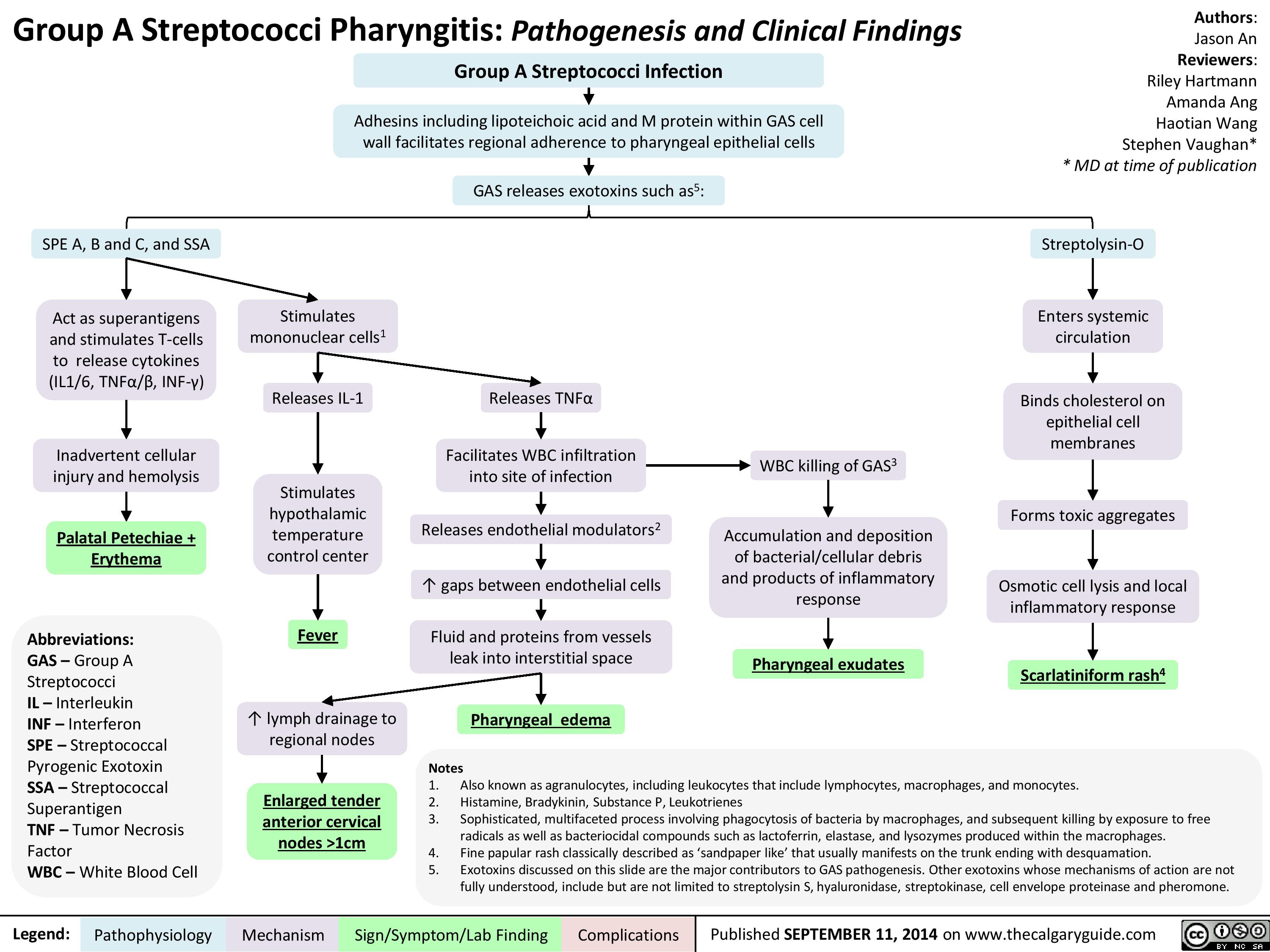
Group A Streptococci Pharyngitis Pathogenesis and Clinical Findings
Scarlet Fever: Pathogenesis and clinical findings

0-1 days post- pharyngitis
Pastia’s lines5
1-2 days post- pharyngitis
Appears on upper trunk and axillae
3-4 days post- pharyngitis
Spreads to remainder of body, sparring face6, palms and soles
7-10 days post- pharyngitis
Fades Desquamation7
Otitis media, sinusitis, pneumonia, bacteremia, osteomyelitis, meningitis, arthritis, erythema nodosum, hepatitis, acute poststreptococcal glomerulonephritis, and acute rheumatic fever
Fine maculopapular rash
Blanchable with Non-pruritic and pressure painless
Notes:
1. While the majority of infections are cases of GAS pharyngitis, rarely, it is possible to develop scarlet fever from a GAS skin infections. 2. Scarlet fever is most common in patients of this age group although, rarely, it can occur in adults.
3. White strawberry tongue is characterized by a white coating on the tongue through which edematous lingual papillae project.
4. Red strawberry tongue is characterized by a beefy red, edematous tongue covered in edematous lingual papillae.
5. Prominent erythema and petechiae in the body folds, especially the antecubital fossae and axillary folds. They tend to appear before the rash and persist through the desquamation phase.
6. Typically, the rash does not occur on the face, although facial flushing may be noted. When this occurs, there is perioral sparring.
7. Desquamation tends to occur ~1 week after the rash fades, most severely effecting the hands and feet, and lasts 2-6 weeks. While a classical presentation, not
everyone gets it.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Sinusitis: Pathogenesis and clinical findings

Erythema Nodosum pathogenesis and clinical findings
 ~28-48% of cases
Medications (Ex. Birth Control Pills, Sulfa drugs) ~3-10% of cases
Malignancy (ex. Lymphoma)
Autoimmune conditions (ex. Sarcoidosis and
Inflammatory Bowel Disease) ~11-25% of cases
Pregnancy ~1-3% of cases
Antigenic Stimuli / Bacteria / Viruses / Chemical Agents all could trigger the following process: Phase 1. Neutrophils Infiltrate the fibrous septa between fat lobules in the subcutaneous fat
Phase 2. Neutrophils release reactive oxygen species, leading to oxidative tissue damage and inflammation
Phase 3. Opening of inter-endothelial junction and the migration of more inflammatory cells into the septal venules, including macrophages, histocytes, and eosinophils
Phase 4. Macrophages secrete inflammatory cytokines, which stimulates the proliferation of more helper T cells (Th1)
Phase 5. Th1 cells secrete more cytokines, leading to the further release of Th1 cytokines and mediating the immune complexes deposition in the septal venules of the subcutaneous fat (panniculitis). The Th1 immune reaction is called Type IV Delayed Hypersensitivity Reaction
Phase 6. Activated macrophages produce hydrolytic enzymes and transform into multi- nucleated giant cells, called Miescher’s Radial Granulomas. These consist of small, well defined aggregations of small histocytes arranged radially around a small cleft of variable shapes in the septal venules of the subcutaneous fat
Phase 1-4. Lesions are red tender nodules, poorly defined, vary in size from 2-6 cm, and usually on shins ( 1st week)
Fat Lobules T lymphocytes
Macrophages
Note: we’ve done extensive research and can’t figure out why erythema nodosum happens mostly on the shins. If you have an answer, please email us!
Phase 5. Lesions become tense, hard, and painful; and they change in color into bluish or livid. (2nd week)
Phase 6. Lesions become fluctuant as in abscess, but do not ulcerate. Lesions fade to a yellowish color
Epidermal layer Dermal-Epidermal Junction
Dermal layer Subcutaneous Fat Layer
Phase 6. Miescher’s Radial Granulomas
Fat Lobules
T lymphocytes
Macrophages
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 25, 2019 on www.thecalgaryguide.com")
necrotizing fasciitis

Laceration
Recent surgery
Injection
Burn
Blunt force trauma
Childbirth
Lower extremity wounds
Bacteria enters tissue through open wound
Infection of muscle fascia Local immune response
Production of exotoxins by bacteria
Disruptions of protective skin barrier
Bacteria introduced into tissue during injury
Necrotizing Fasciitis
Type I infection: mixed aerobic and anaerobic bacteria Type II infection: group A streptococcus
Type III infection: marine organisms, clostridial infections Type IV infection: fungal organisms
Poor blood supply of muscle fascia allows for progressive spread of infection
Systemic immune response
Pyrogens produced by immune system
Pyrogens travel through
the bloodstream to the hypothalamus and alters the body’s thermal setpoint
Transmission of bacteria from infected tissue to blood
Sepsis
Streptolysin (exotoxin) causes blood clot formation
Blood clots in vessels
Tissue ischemia in epidermis, dermis, subcutaneous fat, muscle fascia, and/or muscle
Stimulation of programmed cell death
Tissue destruction
Pain more severe than clinical findings
↓ blood flow fails to meet tissue’s needs
Tissue death
Build up of gas in subcutaneous
tissue from bacteria metabolism
Crepitus
↑ serum creatinine
kinase from protein breakdown
↑ blood flow to infected tissue
Warmth Erythema
Immune cells release vasoactive cytokines into the blood
Capillary vasodilation
Fluid and proteins shift from cells and capillaries to interstitial space
Blood
vessel dilation
↓ perfusion of vital organs
Organ failure
Hypotension
↑ heart rate to perfuse vital organs
Tachycardia
Bacteria releases toxins which are taken up into the bloodstream
Immune cells produce inflammatory cytokines
Circulating toxins activate T cells, over- activating the systemic immune response
Toxic Shock syndrome
Infection ↑ white blood cell production in bone marrow
↑ white blood cells
Destructionof peripheral nerve endings
Insensitivity to pain
Tissue hypoxia à anaerobic metabolism
Poor perfusion of lungs impairs gas exchange
Tachypnea
Cytokines affect dopamine production in the basal ganglia
Acute malaise
Production of non-specific acute phase reactants
↑ C reactive protein and erythrocyte sedimentation rate
Fluid-filled blisters
Edema
Fever Compartment syndrome (see relevant Calgary Guide slide)
Amputation ↑ serum
lactate
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published Nov 20, 2013, updated Dec 19, 2021 on www.thecalgaryguide.com")
IgA Nephropathy
 created by mucosa- bound IgA1 plasma cells is secreted into plasma instead of onto mucosal surface
IgA1 plasma cells hyper- responsive to triggers (eg. URTIs, gastroenteritis) ↑ synthesis of GD-IgA1 → spill-over into plasma
Immunoglobulin A1 (IgA1) plasma cells destined to reside in mucosa (eg. gut or respiratory tract) travel to and
reside in inappropriate site(s) (eg. bone marrow) releasing GD-IgA1 into plasma
GD-IgA1 is not cleared from plasma as quickly as IgA1 → ↑ plasma GD-IgA1 levels
Hit 3:
GD-IgA1-IgG complexes deposit in mesangium
C3 predominant complement activation amplifies inflammatory response
Renal biopsy:
IgA deposits in mesangium (100% sensitive)
Renal biopsy: Complement in mesangium (C3 predominant) (90-95% sensitive)
A cascade of multiple immunologic hits is initiated
Hit 1: ↑ Serum levels of GD-IgA1 multiple immunologic hits
GD-IgA1 hinge region is structurally distinct from IgA1 that would normally circulate in plasma (lack of galactosyl groups)
GD-IgA1 hinge region may mimic pathogens (ex. bacteria and viruses) or other antigens
Cross reactivity of IgG against GD-IgA1, or synthesis of anti-GD-IgA1 IgG antibodies
Immunoglobulin G (IgG) binds GD-IgA1 hinge region Hit 2: GD-IgA1-IgG immune complex formation
Circulating GD-IgA1-IgG complexes have high affinity for glomerular endothelial cells where they damage the glycocalyx → ↑ permeability of immunoglobulins into the mesangium
↑ Production of chemokines, cytokines and complement → ↑ mesangial cell proliferation and matrix expansion
Leukocyte recruitment and activation damages glomerulus and mesangium
Hit 4:
Inflammatory response to GD-IgA1 complexes in mesangium induce glomerular structure disruption (endothelium, basement membrane, podocytes, mesangium)
and impaired glomerular function
Loss of barrier functions of glomerulus allows for extravasation of blood & proteins into Bowman’s space and subsequently through tubules
Renal biopsy: Glomerulosclerosis, tubulointerstitial fibrosis, glomerular vasculitis, podocyte damage
Eventual end-Stage Renal Disease (ESRD)
Progressive ↓ of filtration surface area within glomeruli and ↓ number of functional glomeruli
Proteinuria
Synpharyngitic hematuria (hematuria with dysmorphic red cells co-occurring with pharyngitis)
↓ Glomerular Filtration Rate (GFR)
Nephrotic Syndrome
↑ Serum creatinine
Chronic kidney disease and eventually ESRD
IgAN is an autoimmune disease where IgA deposition in the glomerulus leads to an inflammatory cascade, endothelial dysfunction and mesangial expansion that damages glomeruli causing kidneys to leak blood and protein into urine and decreased kidney function. IgA nephropathy is a multifactorial disease requiring multiple immunologic hits
IgA Nephropathy (IgAN)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 5, 2024 on www.thecalgaryguide.com")
Tonsillitis Pathogenesis and clinical findings

Group A Streptococci (GAS) (most common bacteria)
Group B, C & G Strep,
Fusobacterium necrophorum
Age 5-15 (tonsils have ↑ role in immune function at this age)
Tonsillitis
Inflammation of the tonsils
Infectious agent exposure
Susceptible host Pathogen colonizes the oropharynx
Acute suppurative disease
Immune cells release proinflammatory cytokines & antibodies
Inflammatory mediators ↑ vascular permeability of tonsils
Leakage of protein & fluid into surrounding tissue
Regional nodes receive ↑ lymph
Enlarged anterior cervical nodes
Sinusitis**
Pharyngitis**
Local spread of pathogen
Acute otitis media**
Pneumonia**
Cervical lymphadenitis
Bacteria spread from
tonsils into lymphatic system & bloodstream
Bacteremia
F. necrophorum
invades lateral pharyngeal space & soft tissue in neck
Thrombosis forms in peritonsillar vein
Thrombosis extends into internal jugular vein
Lemierre’s syndrome
Systemic inflammatory cytokines disrupt hypothalamic regulation
Fever
Additional immune cells are recruited to facilitate immune response
Macrophages phagocytize pathogen
Bacteria invade distant tissue & elicit local inflammatory response
Hepatitis Osteomyelitis
Infective endocarditis
Bacteria illicit systemic response
Sepsis
Tonsillar tissue become swollen & irritated
Tonsillar hypertrophy
Localized collection of pus forms
Immune cells cause inadvertent cellular injury & hemolysis
Palatal petechiae
Meningitis
Products of immune response & cellular debris are deposited into tonsillar tissue
Peritonsillar or Tonsillar retropharyngeal abscess** exudate
** See corresponding Calgary Guide slide
Toxin-mediated disease
Bacteria release exotoxins into bloodstream
Inflammatory mediators & cytokines are overactivated (cytokine storm)
Skin has local inflammatory response
Toxic shock syndrome**
Scarlet fever**
Post-infectious disease
Antibodies to GAS cross react with host tissue
Acute rheumatic fever** Post-strep glomerulonephritis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 5, 2018; updated Mar 14, 2025 on www.thecalgaryguide.com")
Acute Infectious Mononucleosis
, Cytomegalovirus
(CMV), human immunodeficiency
virus (HIV), etc) through saliva
(most commonly in adolescents
& young adults aged 15-24)
Virus infects epithelial
cells of the oropharynx
Virus infects & immortalizes
circulating B lymphocytes
Virus replicates in infected B-cells
Immune cell proliferation
in lymphatic system
(primarily lymph nodes & spleen)
Infected B-cells enter
systemic circulation
Systemic inflammatory
response activated
Inflammation &
edema of sinuses
Bilateral periorbital &/or palpebral edema
Pharyngitis**
(often with grey/white
exudative secretions)
Palatal petechiae
Blood vessel damage
in the soft palate
Edema of soft palate & tonsils
Airway obstruction
↑ Immunoglobulin M (IgM) antibodies
to EBV viral capsid antigen (VCA) Positive IgM-VCA
Immortalized B-cells
produce ↑ antibodies
Production of heterophile antibodies
(weakly reactive & non-specific)
Positive monospot (heterophile antibody)
test (↓ sensitivity in children <4 years)
Virus may remain dormant in B-cells
Latent infection with periodic reactivation
Generalized lymphadenopathy (enlarged lymph nodes)
Massive cervical, mediastinal or hilar lymphadenopathy
Posterior cervical
lymphadenopathy
Platelets sequestered (trapped) within spleen &
overactive spleen (hypersplenism) discards ↑ platelets
Thrombocytopenia
(↓ platelets)
Weak reticular tissue in the spleen stretches
Splenomegaly Splenic rupture
& becomes more susceptible to injury
Inflammatory response ↑ energy demand
Fatigue
Longstanding impacts from
unknown mechanism Chronic Fatigue Syndrome
Inflammatory cytokines
released into circulation
↑ Thermo-regulatory
set-point at hypothalamus Fever
Lymphocytosis (↑ lymphocytes)
(markedly CD8+ T-cells & NK cells) Immune cells infiltrate the liver Hepatomegaly
↑ Aminotransferases
Leukocytosis (↑ leukocytes)
CD8+ T-cells & NK cells
indirectly damage hepatocytes
↑ Bilirubin & jaundice**
Systemic immune response &/or
antibiotic hypersensitivity reaction
CD8+ T-cells
respond to virus
Atypical lymphocytes
on blood smear
Generalized maculopapular rash
Authors:
Ayden Hansen, Griselle Leon
Reviewers:
Charissa Chen, Emily J. Doucette
Danielle Nelson*
* MD at time of publication
Published Sept 3, 2015; updated Apr 22, 2025 on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications")
Infection-Related Glomerulonephritis
 trigger the inflammatory cascade
Common infection sites include pharyngitis (infection of the mucous membranes in the oropharynx) &
endocarditis (inflammation of the endocardium) but bacterial infections can originate anywhere in the body
In streptococcal infections, bacteria release nephritis (inflammation of the kidney) associated plasmin receptor antigens (NAPlr) & streptococcal
pyrogenic exotoxin B antigens (SPeB) into the systemic circulation from the infection site. Other bacterial infections may have different pathophysiology
Immune response generated against circulating NAPlr & SPeB antigens includes
↑ production of IgG antibodies (critical for immune response & memory)
IgG antibodies bind with self-antigens (molecules
recognized by the immune system as belonging to the
host) including plasmin & glomerular proteins (proteins
found in the kidney’s filtering unit, the glomerulus)
IgG antibodies activate plasmin
(enzyme responsible for breaking
down protein in the kidneys)
Plasmin degrades
protein in the kidneys
IgG antibodies bind to
glomerular proteins in
the kidney & form
immune complexes in
glomeruli basement
membrane & sub-
epithelial podocytes
(highly specialized
cells in the glomerular
filtration barrier)
Degradation of key
glomerulus components,
including the glomerular
basement membrane
(GBM) & mesangial matrix
Damage to key
glomerulus
components leads to
abnormal regulation
of blood filtration
↓ Selective
permeability of the
glomerular membrane
IgG antibodies bind with NAPIr & SPeB antigens &
form immune complexes (antibody & antigen
combinations involved in immune system signalling)
Immune complexes circulate & deposit in glomeruli
basement membrane & sub-epithelial podocytes
RBCs escape through
the glomerulus into
renal tubules &
progress into the urine
Dysmorphic
hematuria (blood
in the urine
characterized by
misshapen RBCs)
Author:
Joanna Keough
Reviewers:
Britney Wong
Luiza Radu
Jessica Revington
Veronica Hammer*
Louis Girard*
*MD at time of publication
**See corresponding Calgary Guide slide
Legend: Pathophysiology Mechanism
Immune complexes activate
complement (C3, oxidizing
agents, proteases)
Complement activation helps ↑
proliferation of glomerular mesangial
cells (cells with specialized proteins
capable of producing motile forces)
Mesangial cells produce
extracellular matrix in
the glomerulus
Excess
extracellular
matrix
blocks
glomerular
capillaries
Mesangial cells release chemoattractants
(signalling molecules) into the glomerulus
& attract various immune cells
Lymphocytes follow
chemoattractants to the
glomerulus & activate
Neutrophils follow chemoattractants to the
glomerulus & release lysosomal enzymes
Lymphocytes accumulate in the glomerulus
& obstruct glomerular capillaries
Impaired blood flow through glomerular capillaries
Capillary injury Podocyte injury or death
Infection-Related Glomerulonephritis
Glomerular kidney damage sustained after a bacterial or viral infection
↓ Glomerular
filtration rate (GFR)
Creatinine builds
up in the blood
↑ Glomerular membrane permeability allows
large molecules to pass through the membrane
(e.g., red blood cells (RBCs), protein)
↓ GFR impairs the kidney’s
ability to filter & excrete fluid
↓ Estimated GFR
Prolonged
(eGFR)
renal damage
Protein escapes into renal tubules
& progresses into the urine
Chronic kidney disease
Proteinuria (loss of
protein through the urine)
↑ Fluid retention
in systemic
circulation & ↓
renal blood flow
Impaired
potassium
excretion
↓ Urine
output
Impaired
acid waste
product
excretion
Urine contains ↑ large
proteins (e.g., albumin)
Activation of the
intrarenal renin-
angiotensin-aldosterone
system (RAAS)**
Hyperkalemia
(↑ serum
potassium)
Oliguria
(↓ urine
volume)
Metabolic
acidosis**
Albuminuria (loss of
albumin through the urine)
Intrarenal RAAS activation
leads to ↑ angiotensin II
(Ang II) production
↑ Sodium & water retention in systemic
circulation & ↓ excretion in urine (↓ GFR)
Hypertension**
Edema (swelling due to ↑ fluid in body tissues)
Circulating blood volume exerts ↑ pressure on blood vessels & forces the heart to pump harder
Left ventricle thickens & enlarges over time & demonstrates
progressive cardiac injury (e.g., fibrosis, loss of cardiac muscle cells)
Impaired cardiac output
Heart failure
Sign/Symptom/Lab Finding Complications
Published November 15, 2025 on www.thecalgaryguide.com")
Diphtheria
 is
incomplete, absent, or waning
Poor hygiene
environments
Exposure to respiratory droplets or
direct contact with infected surface
Colonization of the pharynx or cutaneous sites
with corynebacterium diphtheriae (C. diphtheriae)
C. diphtheriae proliferate locally
& secrete diphtheria exotoxin
Exotoxin enters nearby host cells &
inhibits host cell protein synthesis
Local epithelial tissue necrosis &
activation of inflammatory response
Accumulation of dead
cells, fibrin, bacteria
& inflammatory cells
Lymphatic & hematogenous spread of exotoxin to distant
tissues (preferentially tissues with ↑ metabolic activity)
Author: Julia Fox
Reviewers:
Steven Quan,
Emily J. Doucette,
James D. Kellner*
*MD at time of publication
**See corresponding Calgary Guide slide
Cutaneous Diphtheria
Cutaneous skin
breakdown
Vesicle/pustule
formation
Superficial, non-healing ulcers
with grey pseudomembrane
Respiratory Diphtheria
Presence of inflammatory
mediators in the pharynx
Mucosal edema
& sensitization
of nociceptors
Dense necrotic pseudomembrane forms &
adheres to larynx, pharynx, or tonsils
Pseudomembrane dislodgment
or extension into the airway
Diphtheria antigens drain
to cervical lymph nodes
Cervical lymphadenitis
Pain & inflammatory
response at infection
site (eg. pharyngitis,
tonsillitis, etc.)
Diphtheritic membrane
(grey mucous membranes)
Localized airway obstruction
(severe laryngeal cases)
Bull neck
appearance
Systemic Manifestations
Protein synthesis inhibition
in myocardial cells
Protein synthesis inhibition in
neurons & Schwann cells
Focal myocardiocyte necrosis,
inflammation, & fibrosis
Demyelination, ↓ myelin
regeneration, & axonal injury
Myocarditis**
Damaged myocardium
disrupts conduction
pathways & contractility
Cranial nerve conduction impaired first (especially
CN IX, X, III) due to ↓ length, ↑ metabolic activity
& proximity to mucosal infection sites
ECG changes (arrhythmias
& heart block)
Palatal &
pharyngeal paralysis
Oculomotor
palsy
Dysphonia, dysphagia,
& loss of gag reflex
Protein synthesis inhibition in glomeruli
& renal tubular epithelial cells
Tubular necrosis &
interstitial inflammation
Renal failure
Endothelial injury ↑
glomerular permeability
Long peripheral nerve conduction
impaired later (2-6 weeks after
initial infection)
Ascending
muscle weakness
Paresthesia
& numbness
Acute
tubular
necrosis
Granular
casts in urine
Proteinuria
Microscopic
hematuria
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published Dec 18, 2025 on www.thecalgaryguide.com")